Endocrine MedSurg
Assessment & Management of Patients with Endocrine Disorders
Endocrine System
Releases hormones to regulate organ function
Works in conjunction with the nervous system
Pituitary Disorders
Pituitary Gland: known as the master gland
Two lobes- anterior & posterior
Anterior pituitary gland:
Thyroid-stimulating hormone (TSH)
Adrenocorticotropic hormone (ACTH)
Growth hormone (GH)
Posterior pituitary gland:
Antidiuretic hormone (ADH)
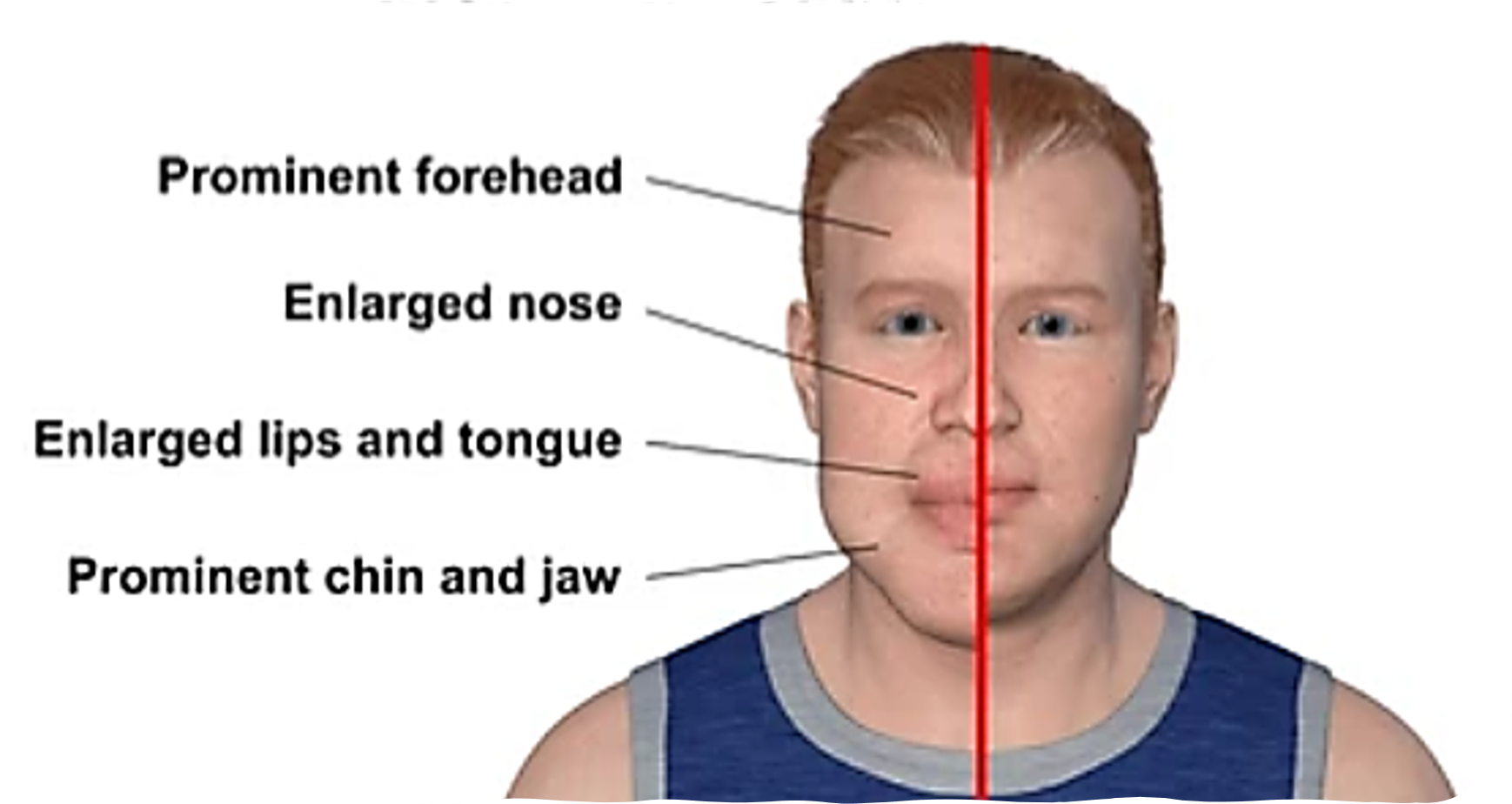
Acromegaly:
Cause: Over-secretion of growth hormone (HG) in adults
Clinical manifestations: excessive skeletal growth in feet, hands, nose, chin, bones of forehead & jaw
Diagnostics: imaging of skull (XR, CT or MRI)
Diabetes Insipidus (DI)
Cause:
inadequate secretion of ADH
occurs as result of an injury to the hypothalamus or pituitary gland
Results in…
excretion of large volumes of dilute urine & extreme thirst
Etiology:
Central DI:
head trauma
surgery
infection
inflammation
brain tumors
cerebral vascular disease
Nephrogenic DI:
kidney injury
meds (lithium)
hypokalemia
hypercalcemia
Dipsogenic DI:
defect in hypothalamus
may be result of damage to pituitary gland from head injury, surgery, infection, inflammatory process or tumor
Clinical manifestations:
polyuria
very dilute urine
intense thirst
s/s of dehydration
confusion, decreased LOC
Diagnostics:
Fluid deprivation test:
fluids are withheld for 8-12 hours (or until 2-5% of body weight is lost)
Patient weighed frequently during test
plasma & urine osmolality studies obtained at beginning & end of test
if pt has DI, there will be no increase in the specific gravity or osmolality or urine
Expected labs:
concentrated blood
serum sodium: high
serum osmolality: high
dilute urine:
urine sodium: low
urine osmolality/specific gravity: low
Collaborative management:
Objective of therapy:
replace ADH
ensure adequate fluid replacement
identify/correct underlying intracranial pathology
Pharmacologic therapy:
Desmopressin
synthetic ADH
causes vasoconstriction
expect life-long therapy
Nursing considerations:
monitor BP
monitor I&O’s
monitor serum sodium levels, urine & plasma osmolality & creatinine clearance
Nursing management:
encourage fluids (PO/IV)
daily weight
monitor vitals
monitor I&O’s
monitor urine output for color & clarity
monitor for s/s of hypernatremia
Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
Cause: over-secretion of AHD
Results in… excretion of concentrated urine, fluid retention, & the development of a sodium deficiency known as dilutional hyponatremia
Etiology:
Disorders of the CNS:
head injury
brain surgery/tumor
infection
Nonendocrine origin:
bronchogenic carcinoma
severe pneumonia, pneumothorax, other lung disorders
Clinical manifestations:
oliguria
fluid retention/overload
hyponatremia (water intoxication)
Diagnostics:
Expected labs:
dilute blood
serum sodium- low
serum osmolality- low
concentrated urine
urine sodium- high
urine osmolality/specific gravity- high
Collaborative management:
objectives of therapy:
eliminate underlying cause if possible
restrict fluid intake
Pharm therapy:
diuretics & fluid restriction
Hypertonic saline (3%)
Nursing management:
daily weight
fluid restriction
monitor vitals
monitor I&O’s
monitor neuro status
DI vs SIADH
Di-
not enough adh secreted ‘
Body unable to conserve water
Thyroid Disorders
Hormones:
Thyroid simulating hormone (TSH)
Thyroxine (T4)
Triiodothyronine (T3)
Hypothyroidism:
Cause: inadequate secretion of thyroid hormones (T3 & T4)
Etiology: primary(thyroidal) hypothyroidism; pituitary (secondary) hypothyroidism; hypothalamic (tertiary) hypothyroidism
Clinical manifestations:
fatigue
lethargy
impaired memory
weight gain
dry skin
constipation
cold intolerance
bradycardia
hypotension
brittle hair/hair loss
Diagnostics:
Radioactive iodine uptake test:
measure rate of iodine uptake by thyroid gland
pt w/ hypothyroidism will have very low uptake
Expected labs:
TSH- high
T3 & T4- low
Collaborative management:
objective of treatment:
restore a normal metabolic state by replacing the missing thyroid hormone
prevention of disease progression & complications
Pharm therapy:
Levothyroxine
synthetic thyroxine (T4)
expect life-long replacement therapy
Nursing considerations:
give daily on an empty stomach (at least 30-60 mins before breakfast w/ full glass of water)
Collaborative Management:
prevention of cardiac dysfunction
Nursing management:
monitor for CV changes
monitor for LOC
monitor respiratory status
monitor vitals
provide extra layer of clothing or extra blanket(s) prn
Complications of hypothyroidism: Myxedema Coma
life-threatening condition that occurs when hypothyroidism is untreated, poorly managed or when a stressor affects a pt w/ hypothyroidism
Clinical manifestations:
hypotension
hypothermia
bradycardia
decreased LOC & lethargy, progressing to coma
respiratory failure
Treatment:
maintain patent airway
intubation & mechanical ventilation PRN
continuous cardiac monitoring
monitor vitals
warm blankets
IV push levothyroxine
Hyperthyroidism:
Cause: over-secretion of thyroid hormones (T3 & T4) by the thyroid
Etiology:
Graves disease
Toxic multinodular goiter
toxic adenoma
thyroiditis
excessive ingestion of thyroid hormone
Clinical manifestations:
anxiety
restlessness/irritability
fine tremors in hand
tachycardia, palpitations
heat intolerance, increased perspiration
increase in appetite
diarrhea
weight loss
thin skin
exophthalmos
pics on slide 37
Diagnostics:
Radioactive iodine uptake test
measures rate of iodine uptake by thyroid gland
pt w/ hyperthyroidism will have high uptake
Physical assessment: auscultating thyroid may reveal a bruit
Expected labs:
TSH- low
T3 & T4- high
Collaborative management:
objective of tx:
depends on underlying cause
directed toward reducing thyroid hyperactivity to relieve symptoms & preventing complications
Surgical Intervention
reserved for special circumstances:
surgical candidates:
pregnant women allergic to anti-thyroid meds
pts with large goiters
pts unable to take anti-thyroid agents
subtotal thyroidectomy:
approx 5/6 of thyroid tissue removed
remaining thyroid usually supplies enough thyroid hormone for normal function
total thyroidectomy:
all thyroid tissue removed
pt will need lifelong thyroid hormone replacement therapy
Nursing considerations:
post-op respiratory distress can occur
what supplies would nurse need at bedside?
Pharm therapy
radioactive iodine- iodine-131
RI is taken up by the thyroid & destroys some of the hormone-producing cells
most common tx for Graves disease
use precautions to prevent radiation exposure to others
Anti-thyroid- propylthiouracil (PTU)
prevents synthesis of thyroid hormone
make take several weeks until symptom relief occurs
Beta blockers- propranolol
used as adjunct therapy for symptomatic relief
monitor cardiac status
Hold for bradycardia
Nursing Management:
promote calm environment
monitor vs
monitor EKG for dysrhythmias
maintain cool, comfortable environment
provide eye protection for pts w/ exophthalmos
Complications of hyperthyroidism: Thyroid Storm
Etiology: results from sudden surge of large amounts of thyroid hormones into the bloodstream, causing an increase in body metabolism
Causes:
uncontrolled hyperthyroidism
infection
extreme emotional stress
thyroid/non-thyroid surgery
vigorous palpation of the thyroid
Clinical manifestations:
hyperthermia >38.5 C (101.3F)
extreme tachycardia (>130bpm)
htn
delirium
abdominal pain/vomiting
dyspnea
chest pain/palpitations
Management:
maintain patent airway
continuous cardiac monitoring
Hypothermia mattress, ice packs, cool environment & acetaminophen
PTU or methimazole
Propranolol
supplemental oxygen
IV fluids for hydration & volume
HYPOthyroidism vs HYPERthyroidism
Adrenal Disorders
Adrenal Glands
steroid hormones are produced by adrenal cortex
gluccocorticoids (cortisol)
mineralocorticoids (aldoesterone)
Addison’s Disease
Causes: insufficient levels of steroids in body
Etiology:
primary adrenal insufficiency
autoimmune disorder
TB
surgical removal of both adrenal glands (adrenalectomy)
metastatic cancer
secondary adrenal insufficiency
sudden cessation while taking short-term corticosteroids
Clinical manifestations
decreased appetite
N/V/weight loss
weakness/fatigue
hyperpigmentation of skin/mucous membranes
hypotension
hypoglycemia
hyperkalemia
Diagnostics:
CT or MRI
evaluate pituitary /adrenal glands
expected labs: ACTH high; cortisol low, sodium low, potassium high
Collab treatment
objective- preventing circulatory shock
Pharm therapy:
gluccocorticoids- hydrocortisone
used as adrenocorticoid replacement
increase dosage during periods of stress or illness if necessary
taper dose if discontinueing0 avoid acute adrenal insufficiency
mineralocorticoids- fludocortisone
Diagnostics
used as adrenalcorticoid replacement
CT scan or MRI, lab values (ACTH, cortisol, sodium, potassium)
Collaborative Objectives
Preventing circulatory shock
Pharmacologic Therapy
Glucocorticoids (hydrocortisone), mineralocorticoids (fludrocortisone)
Mineralocorticoids
used as andrenocorticoid replacement
dosage night need to be increased during times of stress/illness
monitor: weight, BP & electrolytes
Nursing management:
monitor vitals
monitor for fluid & electrolyte balance
monitor daily weight
monitor for s/s pf Addison’s disease
Complications of Addison’s: Addisonian Crisis
occurs when there’s an acute drop in body’s steroid level due to sudden discontinuation of gluccocorticoids or when induced by severe trauma, infection or stress
Life-threatening
Clinical manifestations:
severe hypotension
cyanosis
fever
N/V
tachycardia
severe weakness
Interventions:
administer IV fluids & corticosteroids
monitor vs
place pt in recumbent position w/ legs elevated
Cushing’s Syndrome
Cause: excessive level of cortisol in body
Etiology:
long-term use of corticosteroid meds
excessive gluccocorticoid production by adrenal glands
pituitary gland tumor that produces ACTH & stimulates the adrenal cortex to increase its secretion of cortisol
Clinical manifestations
“buffalo hump:
“moon face”
hirsutism
adipose tissue around trunk, thin extremities
thin skin, bruising
weakness
sleep disturbances
hypertension
hyperglycemia
hypokalemia
Diagnostics:
serum cortisol level- serum cortisol levers are usually higher in AM & lower in PM
urinary cortisol level- 24 hr urine collection
low-dose dexamethasone suppression test- dex given PO late in PN or at HS; plasma cortisol level obtained at 0800 next am
Two out of three tests need to be abnormal to diagnose Cushing’s
CT or MRI- evaluate pituitary gland/adrenal glands
Expected labs:
ACTH- low
Cortisol- high
sodium-high
potassium- low
Collab management:
tx depends on the cause
if related to corticosteroid medication use, determine if regimen can be decreased or replaced with alternative meds
if related ti pituitary gland tumor, pt should have surgery to remove tumor
if related to excessive gluccocorticoid production by adrenal glands, pt should have surgery to remove one or both glands
Surgical Intervention:
hypophysectomy- surgical removal of pituitary gland
post-op nursing care
monitor neuro status
monitor drainage to mustache drip (drop pad)
notify doc if presence of glucose in drainage
high-fowler’s
limit coughing but encourage deep breathing
Adrenalextomy
unilateral or bilateral
post-op nursing csre
monitor for s/s of Addison’s crisis
pt will need hormone replacement therapy
unilateral adrenalectomy requires temporary therapy
bilateral adrenalectomy requires life-long therapy
Nursing management:
monitor I&O’s daily
provide meticulous skin care
monitor & protect against skin breakdown & infection
Addisonian crisis:
pt w/ cushing’s at risk for addisonian crisis when…
circulating hormone level is decreased rapidly because of surgery (adrenalectomy) or abrupt cessation of corticosteroid med
tx on slide 60