Kidney for Dentists
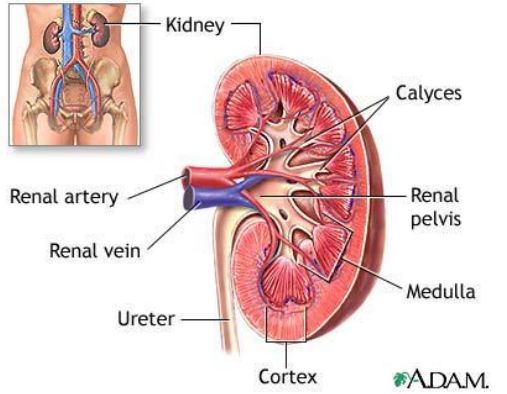
Gross Anatomy
2 Kidneys that sit in the retroperiteneum
5th of cardiac output via the renal artery
Filtrate is turned into urine drained through the renal pelvis
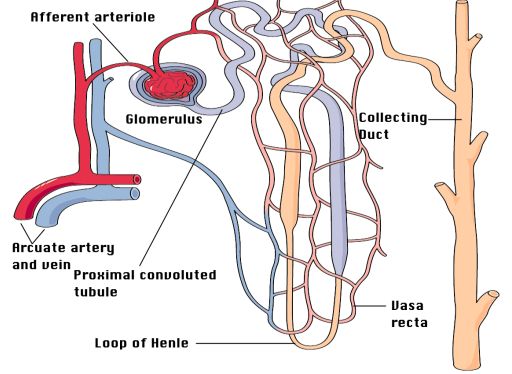
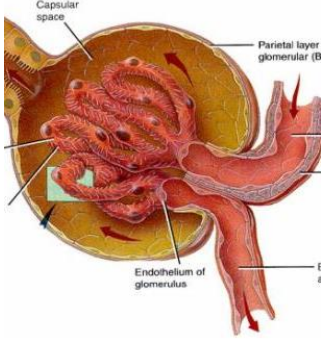
Micro Anatomy
Renal artery → Arcuate artery → Afferent arteriole
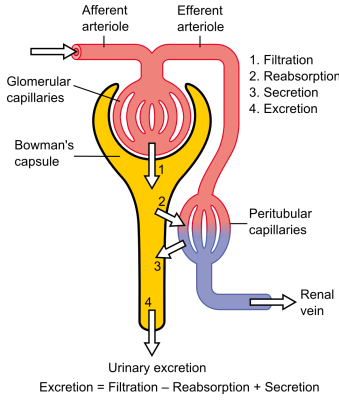
The functional unit of the kidney = nephron
Filtration barrier = podocytes, endothelial cells, basement membrane
Cells larger than 65kDa won’t get past (red blood cells, proteins, etc)
100ml per minute being filtered into Bowman’s capsule
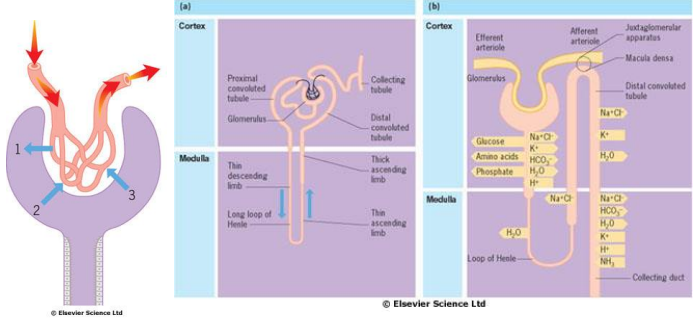
Functional Anatomy
Filtration barrier
Reabsorption by ATP-consuming processes
Generate concentration gradient for water reabsorption
Function of Kidneys
• Excretion
Salt
Water
Uraemic toxins
Drugs
• Metabolic
Regulation of body fluid composition
pH
• Endocrine
EPO
Vitamin D
RAAS
• Blood Pressure Control
Consequences of Renal Disease.
• Accumulation of uraemic toxins.
• Salt and water retention.
• Hyperkalaemia.
• Anaemia.
• Vitamin D deficiency
What is the composition of bone?
• The matrix
– 40% organic
• Type 1 collagen (tensile strength)
• Proteoglycans (compressive strength)
• Osteocalcin/Osteonectin
• Growth factors/Cytokines/Osteoid
– 60% inorganic
• Calcium hydroxyapatite
• The cells
– osteo-clast/blast/cyte/progenitor
Calcium metabolism
What is the recommended daily intake?
• 1000mg
What is the plasma concentration?
• 2.2-2.6mmol/L
How is calcium excreted?
• Kidneys - 2.5-10mmol/24 hrs
How are calcium levels regulated?
• PTH and vitamin D (+others)
Phosphate metabolism
Normal plasma concentration?
• 0.9-1.3 mmol/L
Absorption and excretion?
• Gut and kidneys
Regulation
• Not as closely regulated as calcium but PTH is the most important
PTH
• Physiological role
• Production related to plasma calcium levels
• Control of calcium levels
– target organs
• bone - increased Ca/PO4 release
• kidneys
– increased reabsorption of Ca
– increased excretion of PO4
• gut - indirect increase in calcium reabsorbs by stimulating activation of vitamin D metabolism
Calcitonin
• Physiological role
• Levels increased when serum Ca >2.25mmol/L
• Target organs
– Bone - suppresses resorption
– Kidney - increases excretion
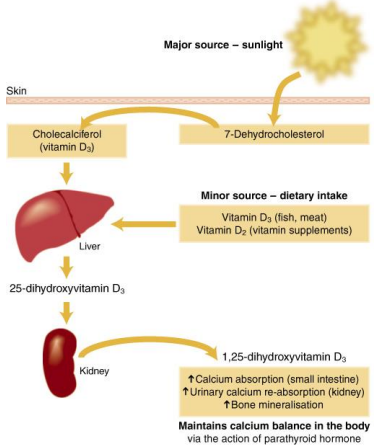
Vitamin D (cholecalciferol)
• Sources of vit D
• Diet
• UV light on precursors in the skin
• Normal daily requirement
• 400IU/day
• Target organs
– bone - increased Ca release
– gut - increased Ca absorption
Vitamin D metabolism
Metabolism of 7-Dehydrocholesterol
To generate Vitamin D3
Which is then hydroxylated by the liver to 25-dihydroxyvitamin D3
Which is then hydroxylated by the kidney to 1,25-dihydroxyvitamin D3
Vitamin D deficiency – under-recognised
Rickets
• Failure of bone mineralisation due to vitamin D deficiency
• Worldwide – due to malnutrition
• UK – lack of sun?
• Bone pain, fractures, myopathy, hypocalcaemia
Osteomalacia
Definition?
• Rickets - growth plates affected, children
• Osteomalacia - incomplete mineralisation of osteoid, adults
Aetiology?
• Decreased intake/production(sun/diet/malabsorption)
• Decreased processing (liver/kidney)
• Increased excretion (kidney)
Osteoporosis
Definition?
• Decrease in bone mass per unit volume
• Fragility (perfusion of trabecular plates)
• Primary (post-menopausal/senile) Secondary
Osteomalacia vs osteoporosis
Osteomalacia:
• dens
• Ill
• General ache
• Weak muscles
• Loosers
• Alkaline pH increase
• PO4 decrease
• Ca x PO4 <2.4
Osteoporosis:
• Aging fem, fractures, decreased bone
• Not ill
• Asymptomatomatic until fracture
• Normal
• Nil
• Normal
• Normal
Ca x PO4 >2.4
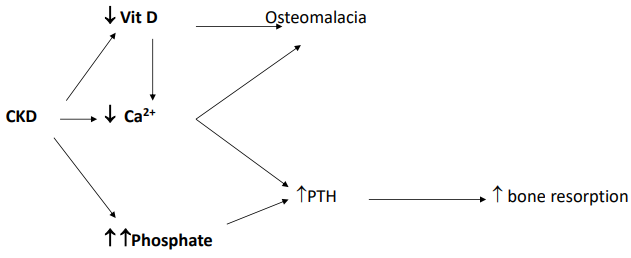
Hyperparathyroidism
• Primary
• Secondary
• Tertiary
Renal Osteodystrophy
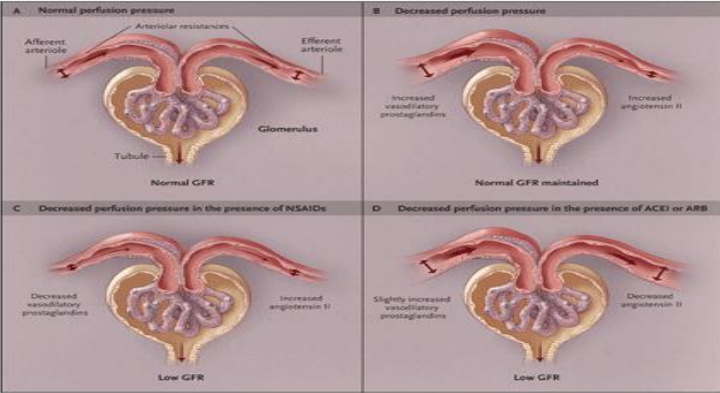
Renin-angiotensin-aldosteron system
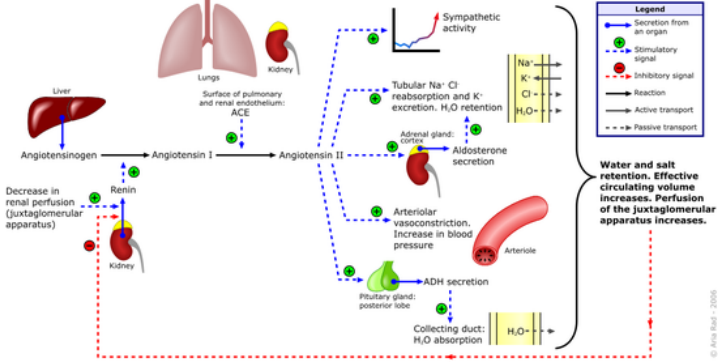
Renal blood flow
• Renal blood flow 1000 ml/min (20% of cardiac output)
• Autoregulation of glomerular perfusion over wide range of systemic BPs
– Myogenic reflex
– Tubuloglomerular feedback
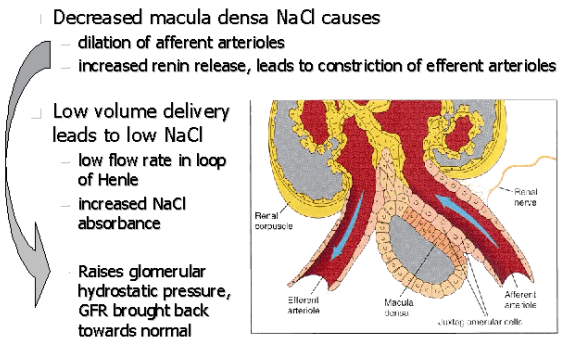
Role of Macula Densa
Glomerular filtration rate
• Flow rate of filtered fluid through the kidney
• Creatinine clearance – volume of plasma cleared of creatinine per unit time
Estimating GFR in clinical practice
Serum creatinine
eGFR
Creatinine clearance
Chromium-EDTA GFR measurement
Relationship between GFR and serum creatinine
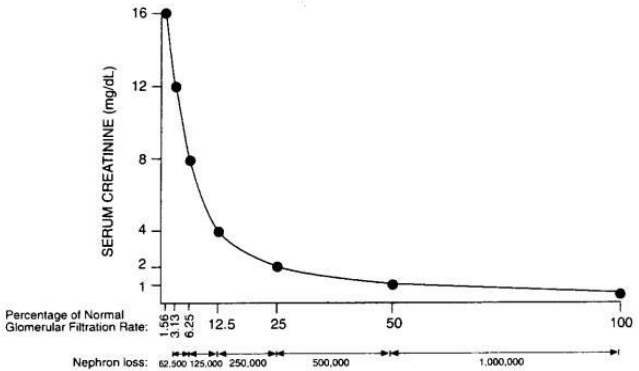
As GFR declines from normal (around 100), down towards kidney failure levels, the relationship between creatinine and GFR isn’t linear. You can lose almost half your kidney function and the creatinine level in the blood has barely changed.
Size does matter:
• Serum creatinine of 110
– His GFR = 140ml/min
– Her GFR = 60ml/min
Meet John……
• A 40y old man who was previously fit and well
• Admitted to maxillofacial unit with severe dental abscess and sepsis requiring surgical intervention following extension into the neck
• Hypotensive and feverish on admission
• Taking oral antibiotics and ibuprofen pre-admission
• Poor oral intake for 4 days with small volumes of dark urine
• AKI at admission
Diagnosis and management of his AKI
• What has caused his AKI?
• Is his AKI important, and is it common?
• What are the complications of AKI?
• How is it managed?
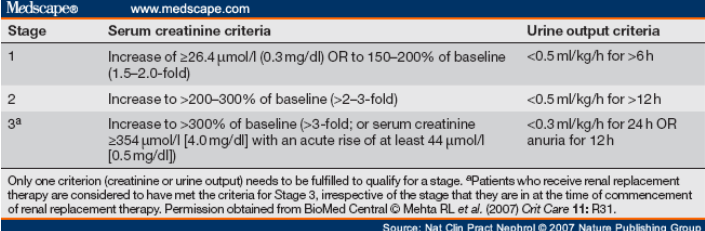
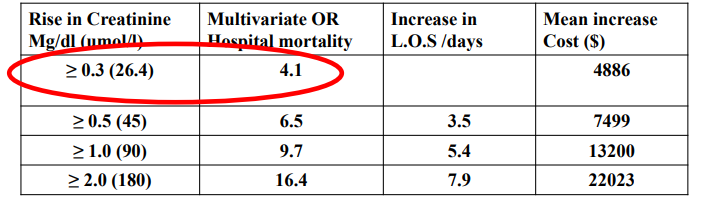
Diagnostic Criteria for Acute Kidney Injury
Epidemiology of AKI – RIFLE in hospital patients
• 20,126 patients included
• According to the RIFLE criteria, AKI close to 20% of hospitalised patients (>40% septic to ITU)
– Risk 9.1%, Injury 5.2%, and Failure 3.7%
• Mortality: Risk 15.1%; Injury 29.2%; and Failure 41.1%
• Odds ratios from Risk 2.5, Injury 5.4, Failure 10.1
•AKI – 13-18% hosp admissions
•Mortality 25-30%
•Therefore modest improvement in outcomes will save many lives
Pathophysiology
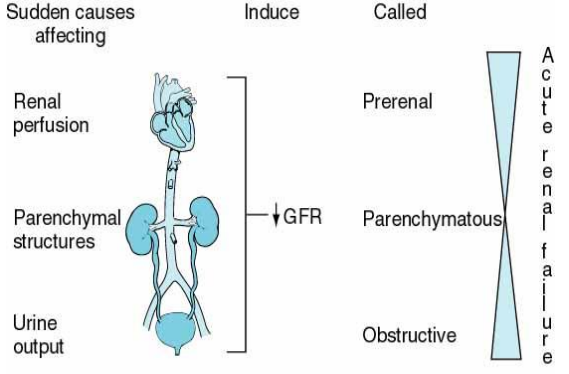
Aetiology
• Pre-renal and ATN (50-65%)
– Low BP
– Sepsis
– Drugs
Aetiology
• Renal (20-35%)
– Nephrotoxins e.g. gentamicin
– Radio-contrast
– Hepatorenal syndrome
– Rhabdomyolysis
– Tumour lysis syndrome
– Myeloma
– Glomerulonephritis
– Acute interstitial nephritis
– HUS/TTP
– Malignant hypertension
– Renal vein thrombosis or embolism
Back to John….
• Differential diagnosis
– Intravascular volume depletion
– Sepsis
– Hypotension
– NSAID causing deranged glomerular haemodynamics
– Antibiotic-related interstitial nephritis
– NSAID-related GN/AIN
If his presentation was complicated by endocarditis…
• Immune complexes form when antibody binds to antigen
• Complement is activated
• Tissue damage and vasculitis occur
Life-threatening complications of AKI
• Hyperkalaemia
• Pulmonary oedema
• Acidosis
• Uraemia (fits, pericarditis)
Treatment
• Treat life-threatening complications
• Eliminate and treat underlying cause
How did John do….
• Survived, but did not regain full renal function
• Left with eGFR 28….
John’s neighbours in the Renal ward
• Nephrotic syndrome
• Normal glomerular filtration barrier
• Triad
– Proteinuria
– Hypoalbuminaemia
– Oedema
• Due to glomerular pathology
Nephrotic syndrome
• 29y South African female with recurrent severe folliculitis re-presents with leg oedema and facial puffiness in the morning
• Dipstick protein +++
• Serum albumin 28 and eGFR > 60 (creat 110)
• ACR 511
• Diagnosis?
– Nephrotic syndrome?
HIVAN
Visible haematuria
• Tumour
• Stones
• Infection
• Prostatic hypertrophy
• Trauma
• Haemorrhagic cystitis
• AVM
• Glomerular pathology (any other evidence?)
• Exclude infection
• Cystoscopy
• Ultrasound/CT/IVP
• Refer nephrology
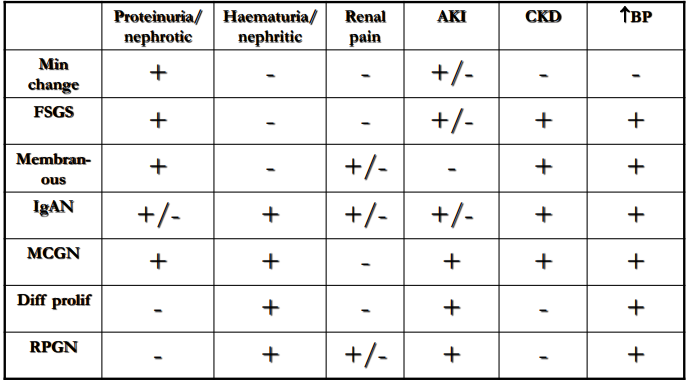
Clinical presentations of kidney disease
Back to John….
• Under follow up with his GP and Nephrologist for CKD…
Classification of CKD using GFR and ACR categories
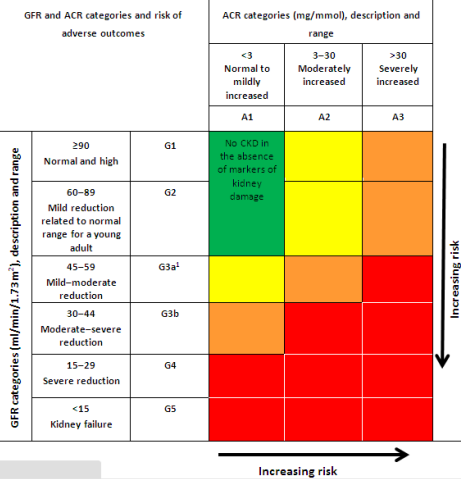
Interpretation
eGFR = % kidney function
Does it matter?
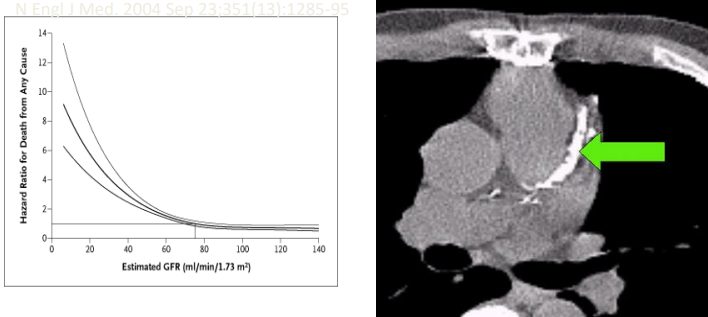
Ask GFR declines from normal (around 100) to abnormal, your risk of death from any cause skyrockets.
GFR of 28 is 4x the increased risk of dying
One possible explanation is the disturbance that you get in calcium phosphate, vitamin D and PCH metabolism that results in early vascular calcification which results in premature cardiovascular events.
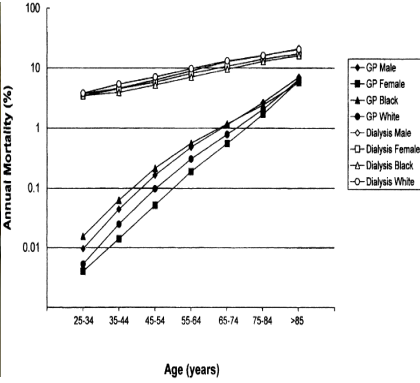
Logarhythmic scale of dialysis
Your risk of mortality goes up from about 0.01% per year to almost 10% per year at 35-44 years old.
Preventing the progression of CKD will reduce their risk of cardiovascular events and risk of ending up in kidney failure and dying.
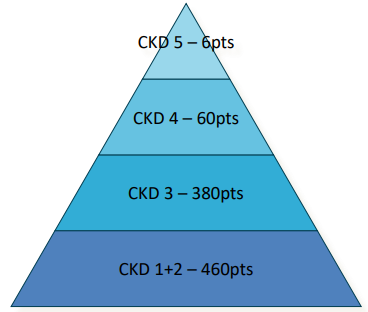
Approx. Numbers of Patients with CKD in a typical 10,000 pt GP Practice
Causes of CKD
• Diabetes – 25%
• Glomerulonephritis – 15%
• Hypertension/renovascular – 15%
• Pyelonephritis/reflux – 12%
• Polycystic/familial – 11%
• Unknown – 16%
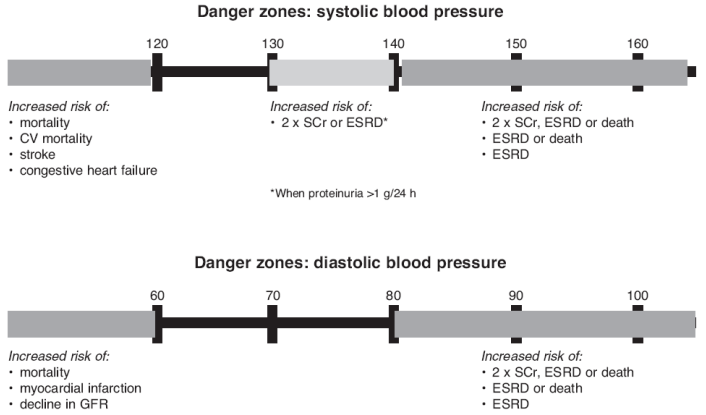
Risk factors for progression of renal failure
• Hypertension
• Proteinuria
• Diabetes
• CV disease
• Smoking
• NSAID use
• Black/Asian ethnicity
• Urinary outflow tract obstruction
Management – all stages
• Lifestyle advice
– Smoking
– Weight
– Exercise
– Salt
– Alcohol
Prescribing in CKD
• Drugs that are excreted by the kidneys
– Digoxin, lithium, opiates
• Drugs that are toxic to the kidneys
– Trimethoprim, aminoglycosides, ACEi, ARB, NSAID
• Some patients on bisphosphonates
Osteonecrosis of the jaw – associated with dental intervention in patients on long term high potency bisphosphonates
Other considerations when managing renal patients
• Platelet dysfunction
• Antiplatelet therapy
• Anticoagulation
• Timing treatment in relation to dialysis
• Immunosuppression – especially in the transplant patient….
Back to John..
• Now aged 48y
• Has 2 children, one of whom wants to go to Dental School
• eGFR down to 14
• What next?
Renal Replacement Therapy in ESRF
• Haemodialysis
• Peritoneal Dialysis
• Renal Transplantation
• Conservative Management
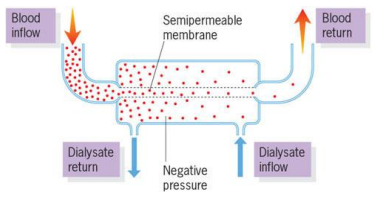
Haemodialysis - Diffusion of ureamic solutes across a semi-permeable membrane
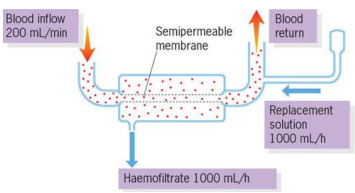
Haemofiltration - Convection of water with ‘solute drag’ across membrane and replacement with fluid balanced solution.
Peritoneal Dialysis
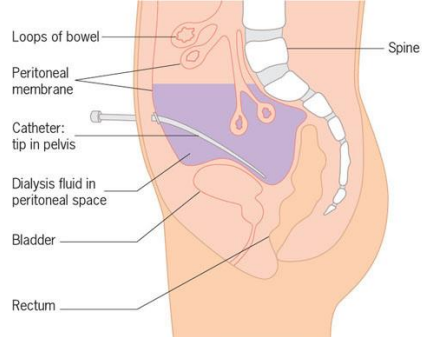
Catheter placed in peritoneal cavity
Through the tube, you pour (every day, several times a day) clean fluid into your peritoneal cavity and in the peritoneal cavity that fluid is seperated by your blood by a semi-permeable membrane.
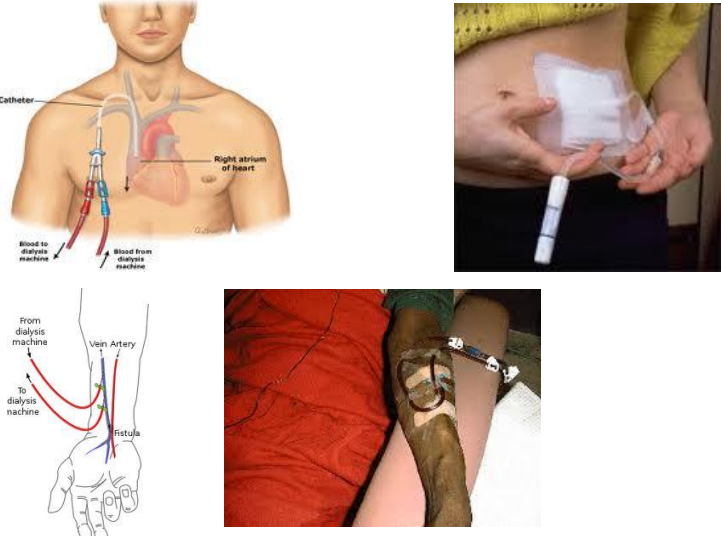
Need to get the blood from the machine back into the patient which can be done through:
Catheter in the internal jugular vein
Catheter in the femoral vein
These tubes are at risk of infection so it is better to have a formation of an arterial venous fistula where you do an operation to join the artery to the vein
Two needles are then connected to the vein where one takes blood to the dialysis machine and the other returns it to the patient
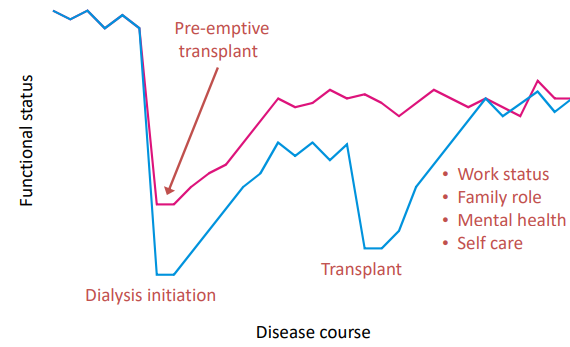
Why Transplantation?
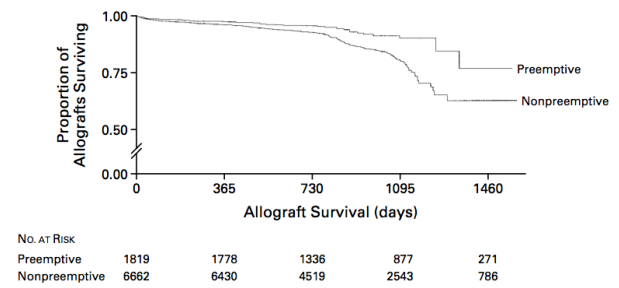
Survival after transplantation compared with those on the waiting list
Potential Pre-Emptive Transplant Advantages
Transplantation
• Live donor vs cadaveric donor
• Lifelong immunosuppression
• Risks of CV disease, infections, PTLD, cancer, NODAT
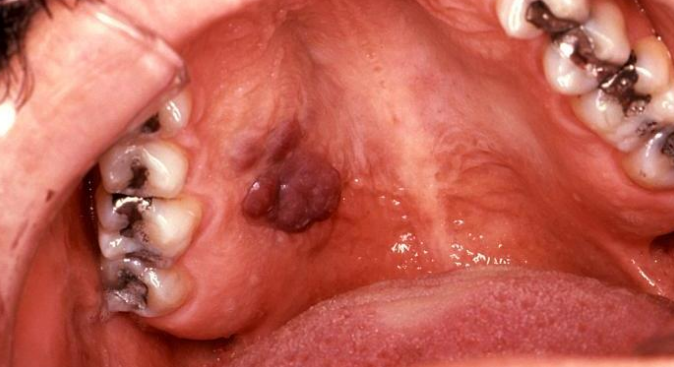
Dental problems and transplantation
• Care with prescribing, and be aware of patient’s medical history, drug history
• Antibiotic prophylaxis (NICE guidelines)
• Bleeding considerations (may need antifibrinolytic therapy, vitamin K, FFP)
• Eliminate/stabilise dental sepsis pre-transplant
• Avoid treatment for first 3 months after transplantation
• Will be at increased risk of infection and drug side effects
Drugs in transplantation
• Cyclosporin – poor wound healing, gingival hyperplasia, exacerbated by CCBs
• Tacrolimus – less hyperplasia, but oral ulceration
• Azathioprine – bone marrow suppression
• MMF – marrow suppression
• Steroids – poor healing, risk of adrenal insufficiency