Neurology
Care of the Child with a Neurological Disorder (NUR 430)
Child vs. Adult Head
Differences in Head Structure:
Poor head control
Rapid myelination
Larger head size relative to body.
Thinner skulls
Abnormal Neuro Exam Associations
Key Areas to Consider:
Head
Reflexes
Musculoskeletal
Gastrointestinal
Eyes
Behavior
Warning Signs
Behavioral Changes:
Change in behavior is the first warning sign.
High-pitched cry
Lethargy
Loss of milestones
Poor feeding
Late vs. Early Signs:
Traumatic Brain Injury (TBI)
Types of TBI:
Concussion: NO SIGNS ON IMAGING
Severe head trauma: Accidental & non-accidental
Risk Factors for TBI
Developmental stage (infants, toddlers, adolescents).
Lack of supervision
Inappropriate/absent safety practices
Improper use of safety devices (helmets, seat belts).
Prevention is the greatest PROTECTION
Abusive Head Trauma
Types of Abusive Head Trauma:
Shaken Baby Syndrome.
Blunt head trauma
Diffuse brain injury.
Classic signs of Abusive Head Trauma
Apnea
Subdural & retinal hemorrhage
History/story does not match what you’re seeing
Nursing Interventions
Maintain airway
Promote skin integrity
Promote pain relief
Nutrition
Safety first
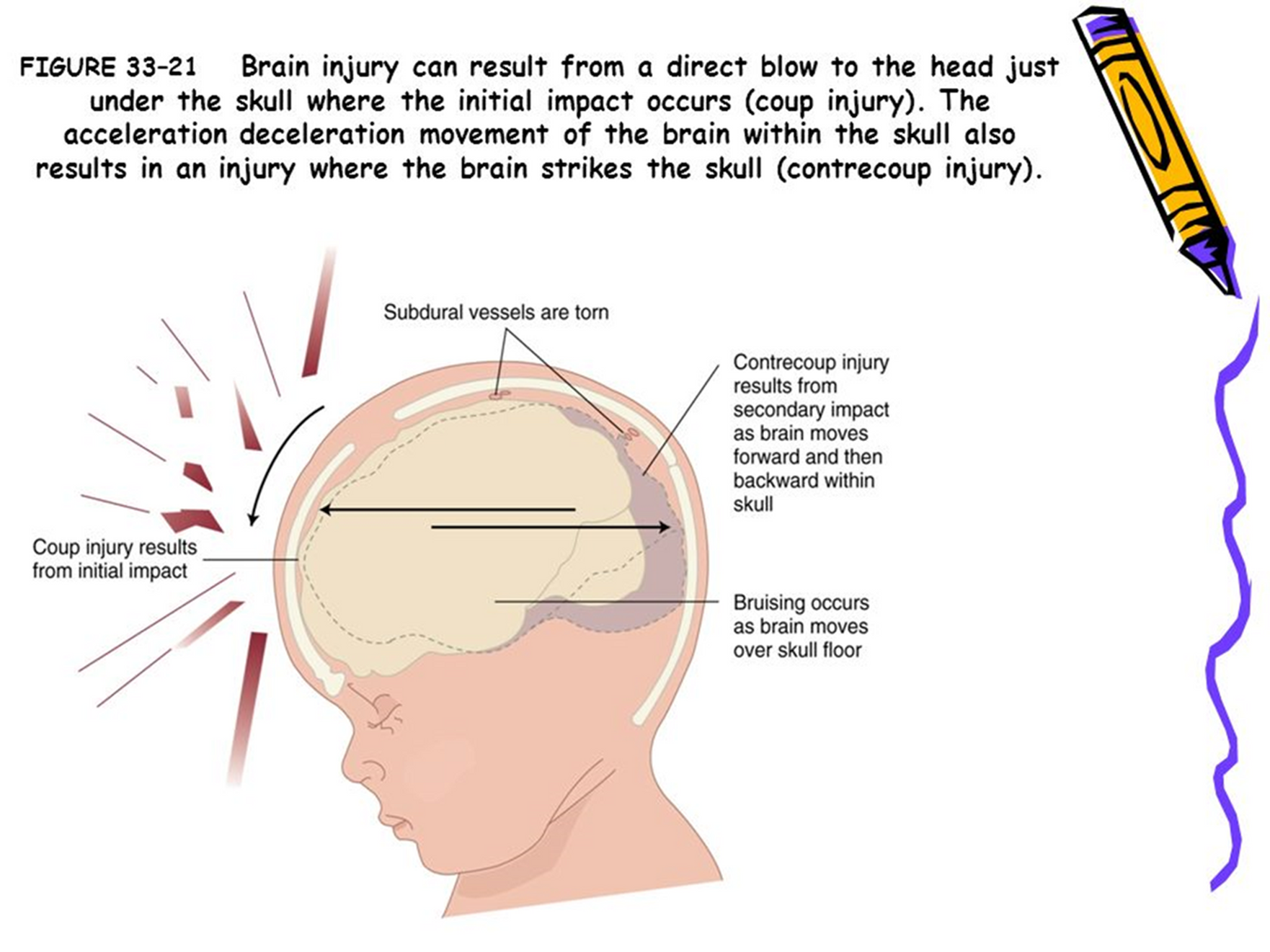
Injury Types:
Coup injury: direct blow to the head.
Contrecoup injury: secondary impact as the brain moves.
Signs of abusive head trauma and discrepancies in history.
Nursing Interventions for kid with Increased Intracranial Pressure (ICP)
Elevate HOB 15-30 degrees
Maintain head in midline position
Avoid pressure on neck veins
Avoid flexion or hyperextension of neck
Avoid respiratory procedures such as suctioning
Prevent constipation
Prevent/relieve pain
Monitor ICP
Must treat if > 20 mmHg
Life threatening if > 40 mmHg
Use gentle movements with ROM exercises
Minimize emotional stress & crying
Keep noise level & lights down
Use padded restraints for clients who have agitation to prevent injury.
Assess for clear fluid drainage from ears or nose (cerebral spinal fluid) and report to the provider.
Assess for bleeding from the ear (indicates basal skull fracture) and report to the provider.
Implement measures to prevent complications of immobility (turn every 2 hr, maintain footboard and splints). Specialty beds might be used.
Insert and maintain an indwelling urinary catheter.
Monitor fluid and electrolyte values and osmolarity to detect changes in sodium regulation, the onset of diabetes insipidus, or severe hypovolemia.
Provide adequate fluids to maintain cerebral perfusion. When a large amount of IV fluids is prescribed, monitor the client for excess fluid volume, which might increase ICP.
Maintain the client’s safety (side rails up, padded side rails, call light within reach.
Provide nutritional support (parenteral nutrition, enteral nutrition). If nasogastric tube is used for nutritional support, do not overfeed due to the risk for aspiration
What if a child bumps their head?
Guide to mild head injury
NO ICP SUSPECTED
Watch closely
Ice 20 mins on/off
Clear liquids 2 hours
When to call back
What is a concussion?
Physical
Mood
Sleep
Thinking
Remembering
Myths on concussions-
Returning to sports-
Headaches
Most important thing:
Rule out worrisome vs. non-worrisome headaches.
Headaches that progress in frequency and severity
Headaches that awaken a child from sleep
Headaches that occur early in the morning
Headaches that become worse upon arising
Headaches that are accompanied by nausea and/or vomiting that are unexplained (not related to flulike illnesses)
Headaches that are persistent and located in the frontal or occipital areas
Headaches that are accompanied by a change in gait, personality, or behavior
Headaches that are made worse by the Valsalva maneuver
Non-Worrisome Headaches
Management:
Keep a journal for patterns and triggers.
Headache Hygiene
Adequate sleep, regular meals, hydration.
Ibuprofen as an effective treatment if needed.
Migraines
Migraine article
What comorbidities are associated with migraines?
What testing should a child w/ migraines have?
What classifies a migraine?
Are kids more likely to have unilateral or bilateral migraines?
What is the first line of tx for migraines?
Which type of headache is hard to treat?
What should the school nurse do to help?
What group of meds should be avoided?
What is second line tx?
What happens if you take too much Acetaminophen or Ibuprofen?
Child vs. Adult Migraines:
Seizures
What is Epilepsy?
Seizure- there can be multiple reasons for a seizure. It does not mean a person has epilepsy from just one seizure
Epilepsy- 2 or more unprovoked seizures
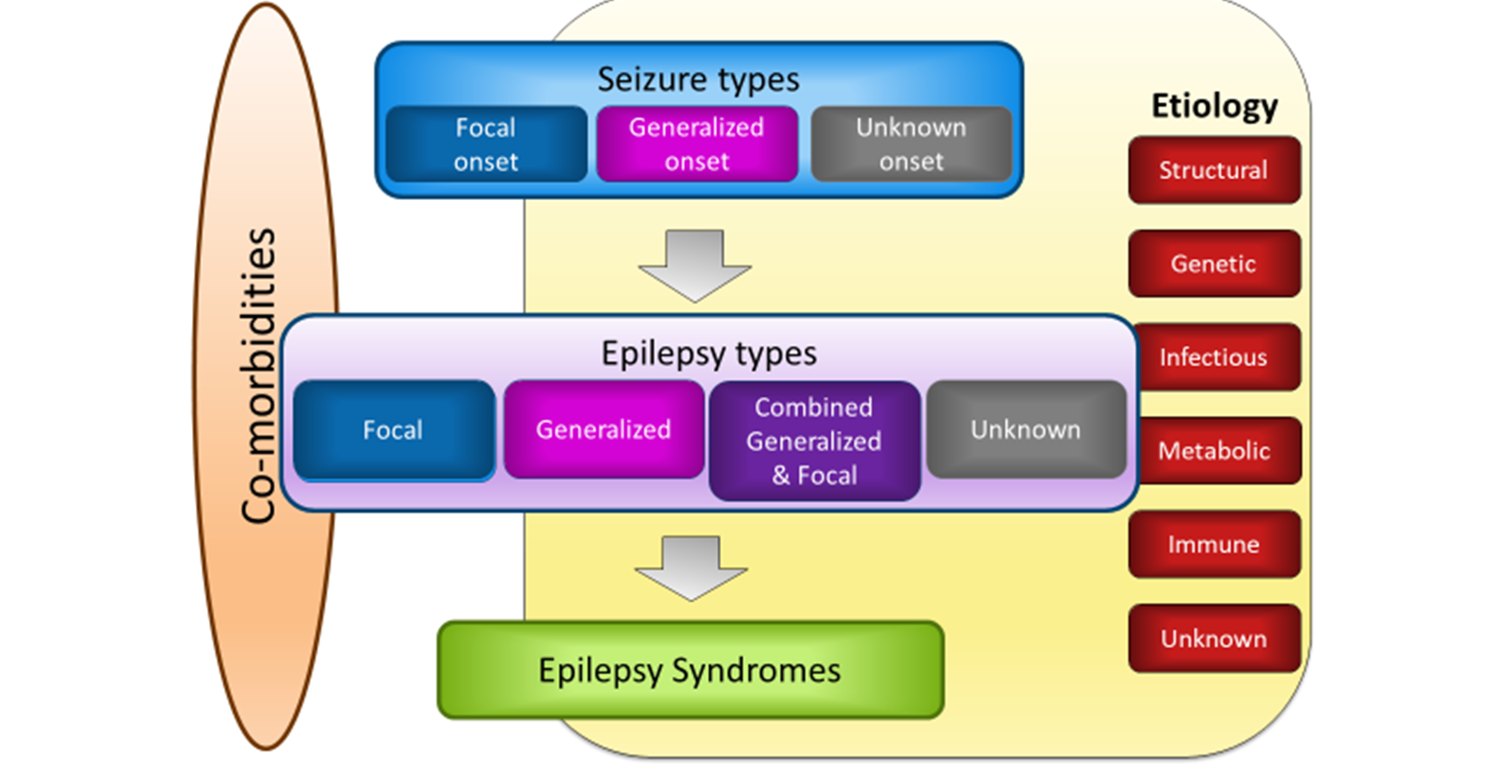
Seizure Types and Etiology
Risk Factors for Seizures
Genetic conditions
Brain tumors
Fever
Toxins
Metabolic conditions
Lead poisoning
Cerebral edema
Intracranial infection
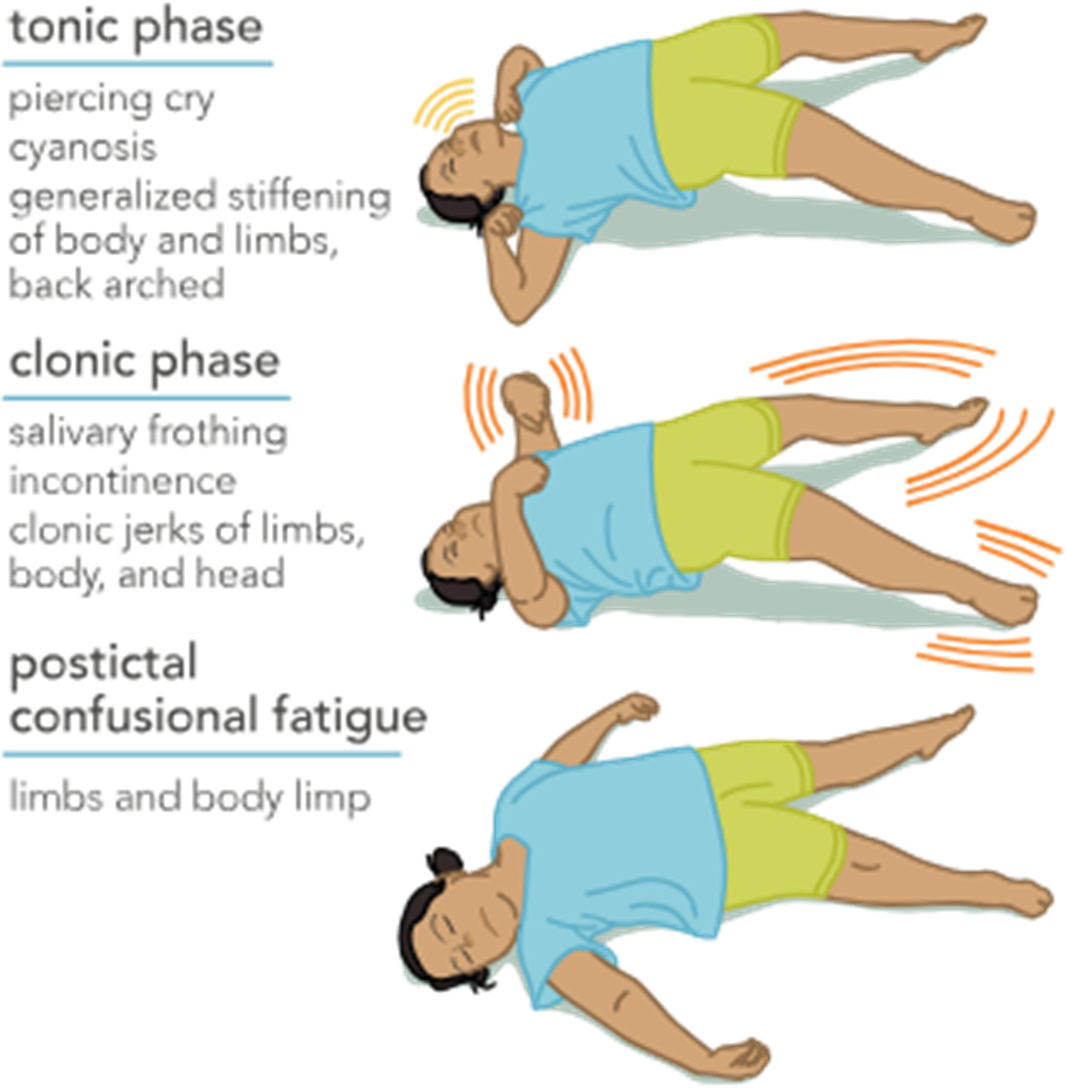
Seize the day: My patient is seizing..what do I do?
Post-Seizure Care
Maintain seizure precautions
Pads; bed in lowest position, emergency equipment ready
Vital signs
Neuro check
Do not offer anything to eat until fully awake
Keep child in the side lying position until fully awake
Find out if they had an aura before seizure
Determine triggers
Treatment for Epilepsy
Treatment Options:
Medications
Brain mapping
Vagal nerve stimulator
Keto diet
Medications for Seizures
Scheduled vs. PRN
Monotherapy & broad spectrum
Drug levels for some
Give meds on time
Start after 2nd unprovoked seizure
Carbamazepine, Valproic Acid, Phenytoin
Seizure Education for Caregivers
Triggers and Precautions:
Importance of awareness and management of seizure triggers.
Parents must learn CPR
Know triggers
Educate do not stop medicine suddenly
Wear a helmet and keep area safe.
Obtain a medical bracelet
Health Inequities
Discussion on Health Inequities:
Developmental Concerns
Plagiocephaly- No ICP
Frequent repositioning 30-60 mins/day of tummy time; orthotics if severe
Risk Factors
Premature birth
Developmental milestone delays
Decreased time in prone position

Craniosynostosis: risk of ICP
Increased ICP & head malformations
Surgery before 6 months with post-op helmet afterwards
Surgery can cause large blood loss- monitor for signs of shock & neuro changes

Reye's Syndrome
Can lead to permanent neurological problems & liver failure