History of Reconstructive and Aesthetic Surgery
History of Reconstructive and Aesthetic Surgery
Synopsis
Closure of wounds is one of the earliest acts of reparative surgery.
Historical evidence suggests nearly every conceivable local flap has been documented historically, showcasing the boundless creativity of plastic surgeons.
Contemporary understanding of "new" flaps shows they are often innovations on previously established techniques.
Acknowledging that "nothing is new under the sun" is essential for humility in the field.
Historical Definition of Plastic Surgery
In 1597, Gaspare Tagliacozzi (1545–1597) defined plastic surgery as:
“the art devoted to restore what Nature has given and chance has taken away.”
The primary aim is not the restoration of beauty, but rather the rehabilitation of the affected area, addressing congenital or acquired defects, aiming for normal appearance and function.
The term "plastic" derives from Greek (πλαστικóς), meaning moldable.
Origin of Plastic Surgery
The Distant Past – Wound Management
The historical origins trace back to managing wounds inflicted by weaponry and animal bites, looking through the lens of primitive human experience.
Early problems concerning woundry management included:
Closing post-traumatic defects
Controlling bleeding
Preventing infection
Alleviating pain
Initial attempts to promote faster wound healing by shifting from secondary to primary intention represent the first reparative efforts, albeit rudimentary due to the lack of tools, hemorrhaging, and absence of anesthesia.
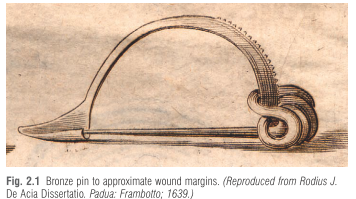
Early interventions lacked documented stitching; evidence from ancient Hindu medicine suggests rudimentary methods employed fibers or animal tendons, leading to eventual use of bronze pins.
Ancient Egyptian Medicine
The Edwin Smith Papyrus (circa 1650 BC) is an ancient medical text, considered the oldest known surgical treatise, that outlines 48 surgical cases, including wound healing, fractures, and tumors. Key points include:
Fresh wounds treated conservatively with honey and grease, utilizing linen swabs, suggesting antiseptic and anti-inflammatory properties of honey.
For nasal fractures, it suggests removing clots and repositioning bony fragments using rolls of linen for internal support or splinting, indicating early methods for impacting nasal injuries.
The text demonstrated a systematic observation of patients, diagnosis, and treatment, rather than magical remedies.
Surgery instruments weren’t mentioned, highlighting that cases assumed pre-existing wounds.
Mesopotamian Contributions
Mesopotamia, particularly prominent for cuneiform tablets, contained medical insights from around 600 BC (earliest from 2000 BC).
Some tablets offered remedies using local plants for wound treatments, although surgical procedures were rarely documented despite being practiced.
The Hammurabi Code (circa 1700 BC) acknowledged surgical malpractice, detailing repercussions for physicians causing harm during operations.
Innovations in Indian Medicine
The Samhita, attributed to Sushruta (around 600 BC), documented reconstructive techniques for facial anomalies, notably procedures regarding eyelid and nasal reconstruction.
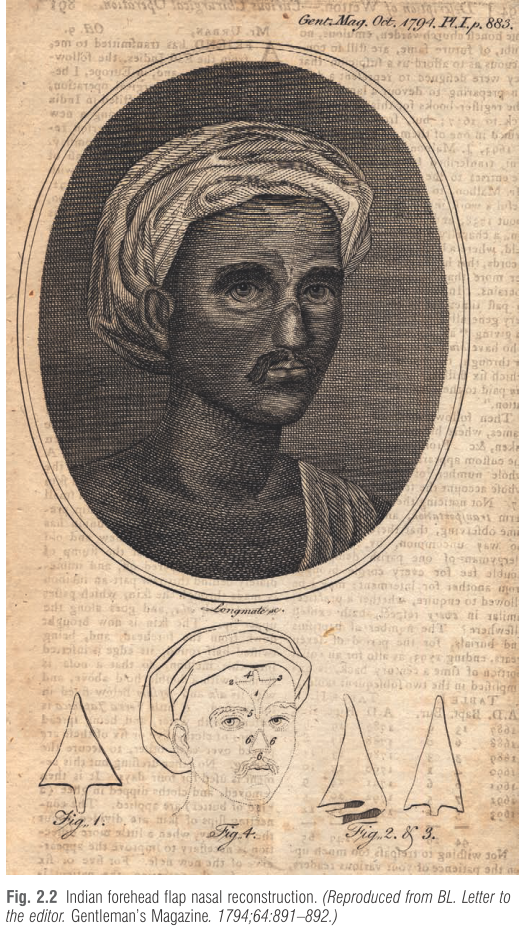
Sushruta described a detailed method of rhinoplasty (nasal reconstruction) using a flap of skin from the cheek or, more famously, the forehead (the "Indian method"). This technique involved taking a pedicled flap of skin, rotating it to cover the nasal defect, and then suturing it in place.
Noteworthy practices involved local flaps for various defects, and a wide array of surgical tools (sharp and blunt, totaling over 100 instruments) were implicated in nasal repairs and other reconstructive procedures, including earlobe repair.
The Samhita detailed hygienic practices and surgical training, influencing future medical traditions.
Greek and Roman Contributions
Greek Medicine - Significant influence stemmed from Hippocrates (around 460 BC) who advocated for evidence-based practices within the Asklepieion. His extensive writings, potentially compiled into the Corpus Hippocraticum, highlighted diverse surgical practices and treatments involving cauterization, fracture treatment, and cranial trephination.
Key writings included specific techniques for treating injuries, describing foundational principles of surgery and emphasizing observation and prognosis.
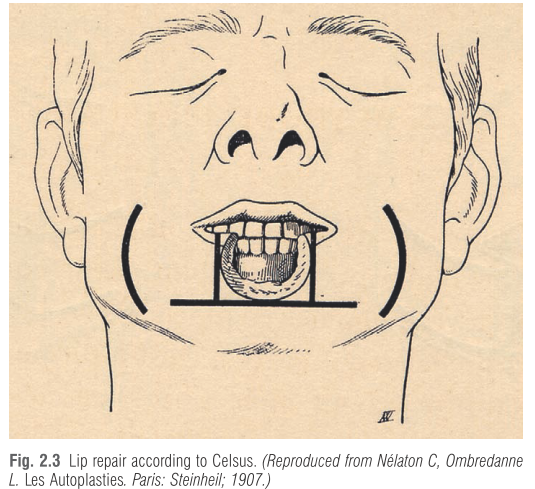
In Roman Medicine, records show a sophisticated understanding of surgical needs. Aulus Cornelius Celsus in De Medicina (30 AD) described surgical practices including flaps for closing ear, lip, and nose defects, introducing various surgical techniques and tools suitable for the era.
CELSUS introduced the four cardinal signs of acute inflammation, “redness and swelling with heat and pain” (rubor et tumor, cum calore et dolore).
Claudius Galen's contributions included extensive anatomical investigations, with notable claims regarding anatomy and nerve functions based on animal dissection, which heavily influenced Western medicine for over a millennium. Claudius Galen (c. 129–201 AD) was born in Pergamon
(Turkey), studied medicine at the Asklepieion (see above) in his native city and moved to Rome. He wrote about head traumas, techniques of Mtrephination for evacuating hematomas and various types of bandaging. An excellent anatomist,,he described more than 300 muscles, the seven pairs of cranialMnerves and contributed to neurology, demonstrating that
nerves arise from the brain or spinal cord. He observed that section of the laryngeal nerve resulted in dysphonia. For management of wounds he used sutures and cautery. Numerous works of Galen were lost, but 82 survived. Originally written in Greek, many were translated into Arabic and Latin.
Post-Roman Innovations
Byzantine Surgery:
Oribasius documented reconstructive methods for various defects while Paulus of Aegina outlined surgical techniques such as tracheotomy and tonsillectomy.
Arabian Contributions:
Albucasis (936–1013 AD) authored Al Tasrif, a 30-volume medical encyclopedia, with its surgical section filled with detailed descriptions of surgical instruments and cauterization techniques, thereby significantly enhancing the surgical understanding of wounds and procedures.
The Middle Ages and Education
The establishment of universities, notably in Bologna (1088), advanced medical and anatomical study, notably through extensive cadaver dissections, challenging older anatomical beliefs. The rise in printed texts in medicine fostered the spread of surgical knowledge across Europe, leading to greater standardization.
The Renaissance
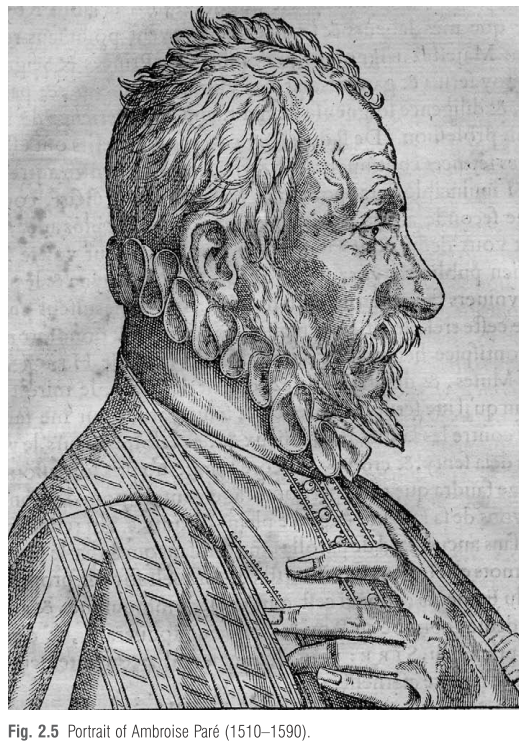
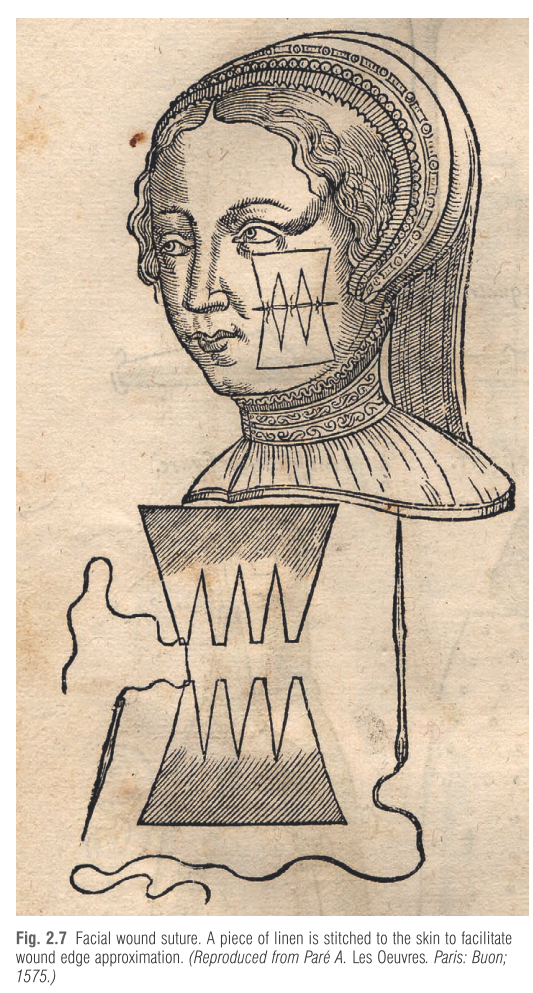
Ambroise Paré (1510–1590), a military surgeon, introduced less invasive treatment for wounds, advocating for the ligation of arteries over painful cauterization for hemorrhage control, and made significant techniques for facial surgery and cleft lip repairs. He is also credited with advancing prosthetic limbs.

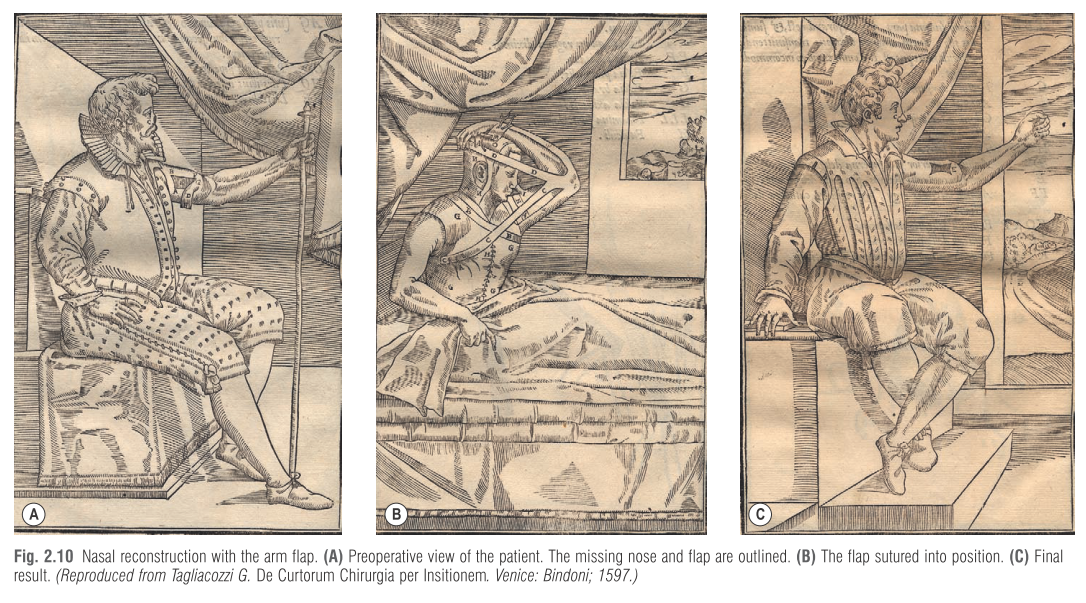
In 1597, Gaspare Tagliacozzi’s celebrated work De Curtorum Chirurgia per Insitionem (On the Surgery of Mutilation by Grafting) provided the first organized documentation on nasal reconstruction, detailing a complex method using a pedicled flap from the upper arm. This "Tagliacozzi flap" involved attaching a skin flap from the patient's arm to the nose, allowing it to vascularize there for several weeks before detaching the base, a highly advanced and systematic technique for his time.
Possibly Fioravanti’s book came to the attention of Gaspare Tagliacozzi who successfully applied the technique on some patients and published his famous textbook in 1597. Although Tagliacozzi was not the discoverer of rhinoplasty, and the arm flap operation is now rarely performed, he deserves credit for being the first to make a work of art out of a surgical practice, for systematizing and promulgating nasal reconstruction. He is rightly considered the founder of plastic surgery.
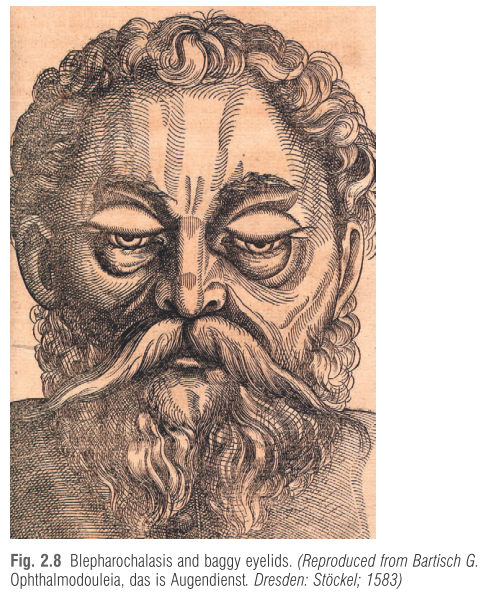
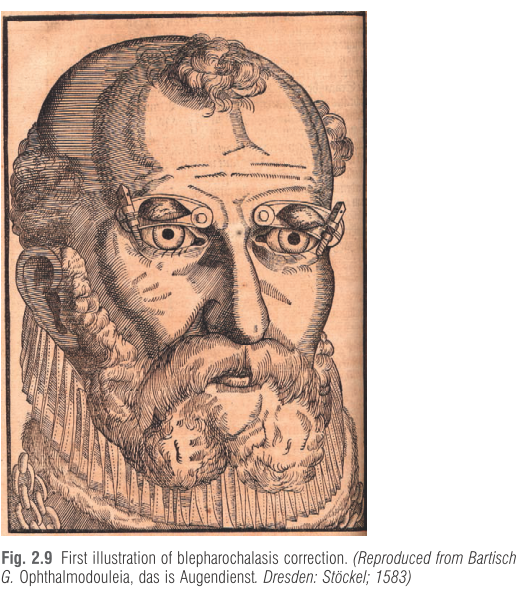
The year 1583 marks a great breakthrough in ophthalmology and eyelid surgery with “Ophthalmodouleia, das ist Augendienst” (Ophthalmodouleia, or the Service of the Eyes) by Georg Bartisch (1535–1607), oculist to the Elector August of Saxony. The book constitutes the first comprehensive treatise on the care and management of the diseases of eye and adnexa
and is embellished by dozens of detailed anatomical images of the eye, eyelids and brain, as well as of surgical instruments. Besides this, it includes the first clinical illustration of blepharochalasis and baggy eyelid (Fig. 2.8) and the report of an original technique for surgical excision of the overhanging skin fold above the tarsus for correcting blepharochalasis,
using a curved clamp in the form of a guillotine (Fig. 2.8 e 2.9).
The decline of plastic surgery
After Tagliacozzi’s death, apart from his pupil G. B. Cortesi (1554–1634), who published a book on nasal reconstruction in 1625, 20 the operation, which was difficult to perform, became obsolete for almost two centuries. Sporadic cases were reported in 17th- or 18th-century literature. Instead of recommending autologous tissue for restoring a missing nose, surgeons like Fallopio (1523–1562), Heister (1683–1758), Camper (1722–1789), and others advocated the application of a prosthesis, convinced that noses made out of wood or silver were far superior to those of skin.
The 19th Century - The golden age of plastic surgery
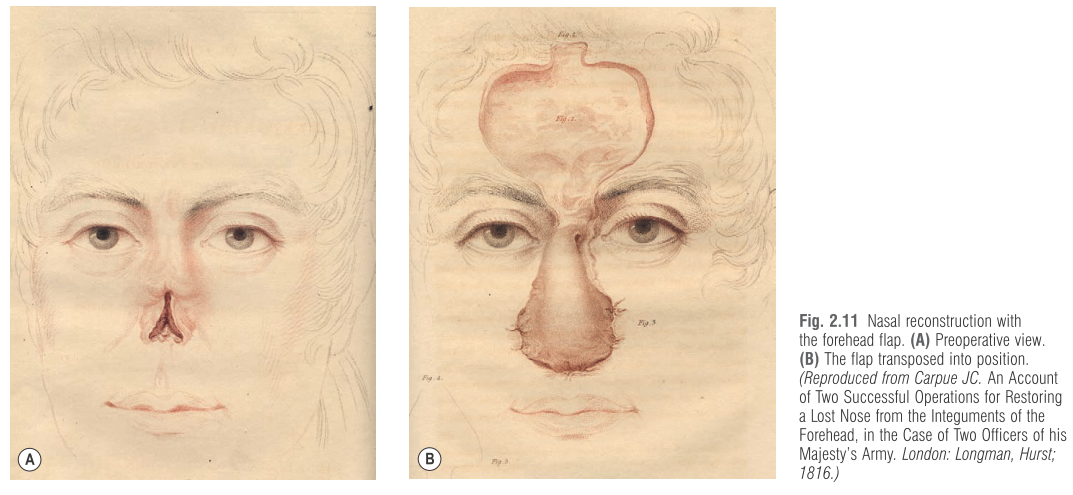
Joseph Carpue (1814) successfully performed the first modern rhinoplasty in England using the "Indian method," recreating a nose with a forehead flap, signifying a revival of ancient techniques and their adaptation to contemporary practice.
Carl Ferdinand von Gräfe (1818) popularized rhinoplasty in Europe, developing his own "German method" using a free skin graft or regional transposition flaps, further advancing the field.
Bernard von Langenbeck (1859) made significant advances in closures for cleft palates, introducing the mucoperiosteal flap technique for surgical repair, which became foundational for modern palatoplasty.
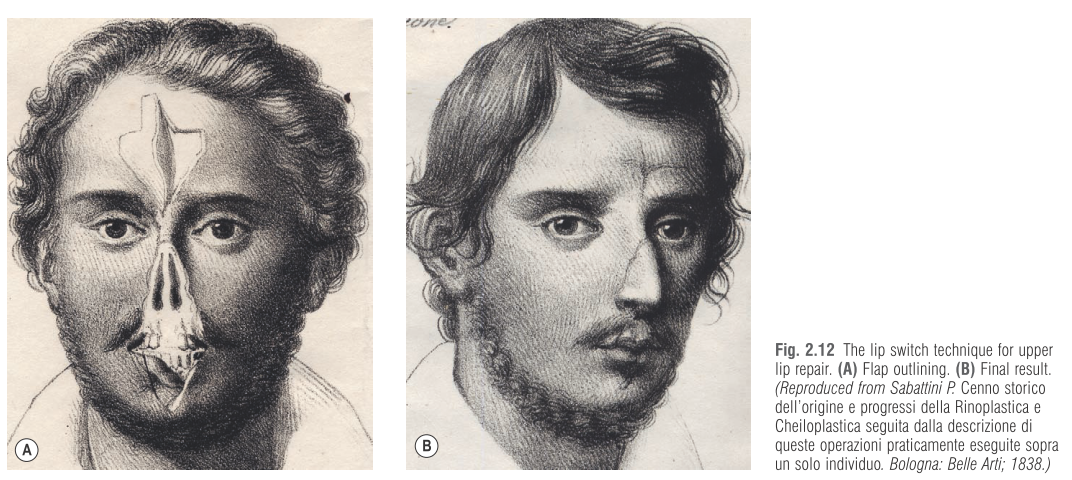
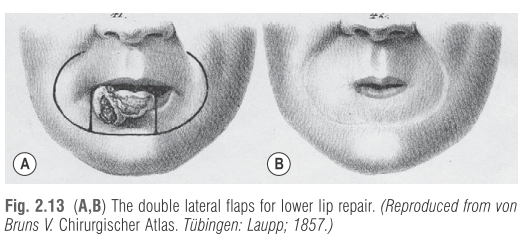
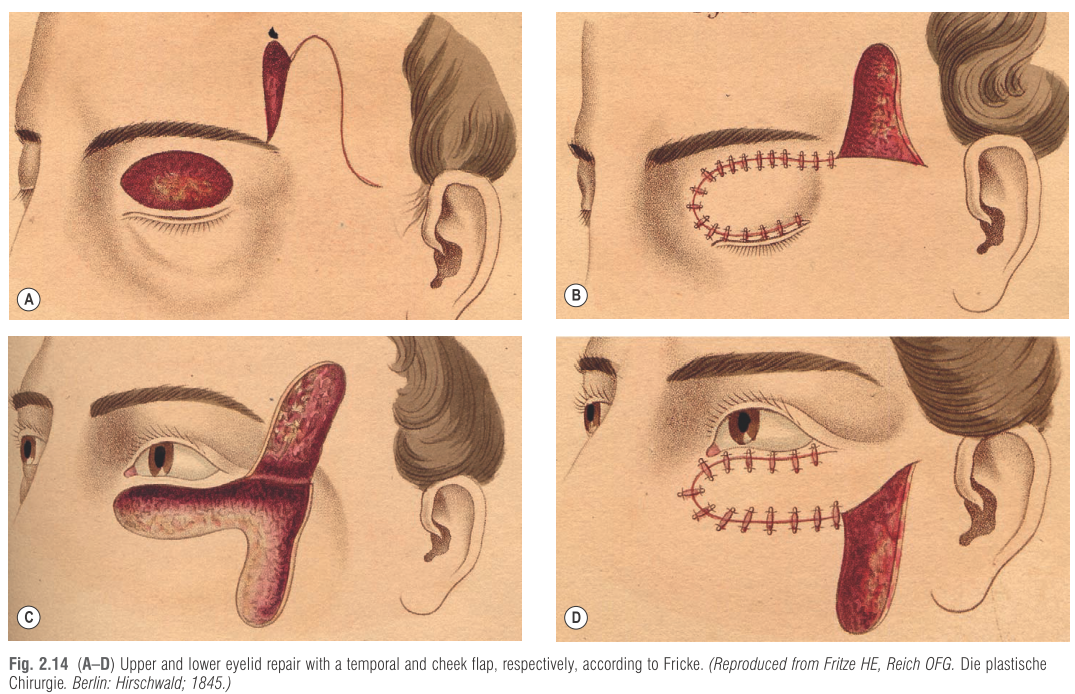
Reconstructive procedures for lip 37 were reported by Pietro Sabattini in 1838, using the lip switch technique 27,38 (Fig. 2.12), and by Victor von Bruns (1812–1883) in 1857, using double lateral flaps for oral sphincter restoration 39 (Fig. 2.13), whereas eyelid repair was reported by Johann Fricke (1790–1841) in 1829, who described a pedicled skin flap from the ipsilateral temple or cheek region to correct upper or lower eyelid defects, respectively 40 (Fig. 2.14).
Advances in surgical techniques including anatomical precision and skin grafting developed significantly through the century. This became possible through the pioneering work of Giuseppe Baronio (1758–1811) from Milan, who performed the first autologous skin graft in a ram in 1804 (Fig. 2.15). Sixty five years later, Jacques Reverdin (1842–1929) carried out the first successful epidermic graft on a human being at Hôpital Necker in Paris. A few years later, Louis Ollier (1830–1900) transferred a large piece of split-thickness skin, which included the superficial layers and underlying dermis. Carl Thiersch (1822–1895) and John R Wolfe (1824–1904) made further advances in the procedure. In the late 1800s, skin grafting became the preferred solution for the management of chronic and granulating wounds.
The introduction of anesthesia (ether in 1846, chloroform in 1847) and antisepsis (Lister's work in the 1860s) revolutionized surgery by enabling longer, more complex procedures and drastically reducing infection rates, making widespread plastic surgery feasible.
The 20th Century - World Wars Impact
The horrors of WWI unveiled the critical importance of reconstructive surgery, compelling rapid advancements in techniques for severe facial disfigurements and other traumatic injuries.
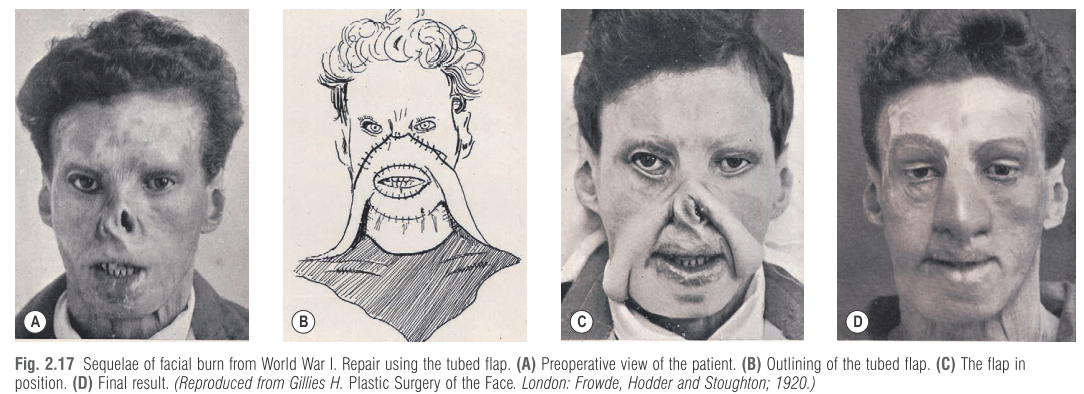
Figures like Sir Harold Gillies (often considered the father of modern plastic surgery) established specialized units for facial reconstruction during WWI. He systematized new reconstructive procedures, like the tubed flap, described by the Russian Vladimir Filatov (1875–1956), which allowed the
coverage of large skin defects, but also skin flaps, bone, cartilage, and skin grafts (Fig. 2.17).
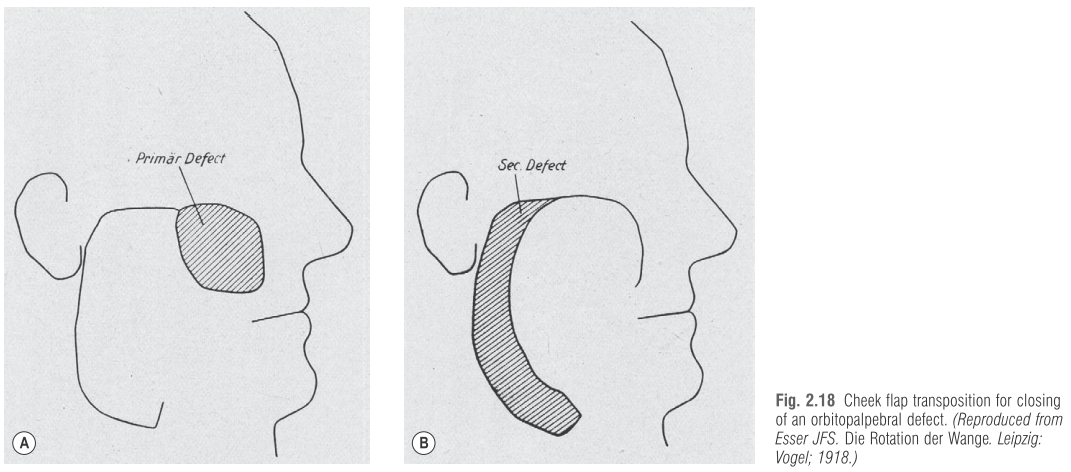
The Dutch surgeon Johannes Esser (1877–1946) was activenat Tempelhof Hospital, Berlin, and in Vienna. Between 1916 and 1918. Esser codified some of the flaps currently used today: cheek rotation (Fig. 2.18), bilobed, island, and arterialized flaps, which he called biological flaps.
In the US the specialty only grew after World War I. Vilray Blair (1871–1955), trained at Sidcup, established the first independent unit in the US for the care of complex maxillo facial injuries at Walter Reed Hospital
Training and Specialization
Post-war developments saw the establishment of formal training programs and societies aimed at refining and promoting plastic surgery, addressing the public’s perception and delineating professionalism in the field. This led to plastic surgery becoming a recognized specialty with rigorous training standards.
The birth of the scientific societies - The aim of the scientific societies was to improve the scientific level of the specialty and to defend the public from charlatans. The first society was the American Association of Oral and
Plastic Surgeons, established in 1921 by Truman Brophy (1848–1928), who strongly supported close cooperation between oral and plastic surgeons. Initially membership required the MD and DDS degrees.
In Europe, the first society was the Société Française de Chirurgie Réparatrice Plastique et Esthétique, established in 1930 by Charles Claoué (1897–1957) from Bordeaux and Louis Dartigues (1869–1940) from Paris. It only lasted 2 years. In 1931, Jacques Maliniak (1889–1976) founded the American Society of Plastic Surgeons.
In 1946, the Plastic and Reconstructive Surgery Journal was established and Warren B. Davis was appointed as an editor.
Postwar plastic surgery
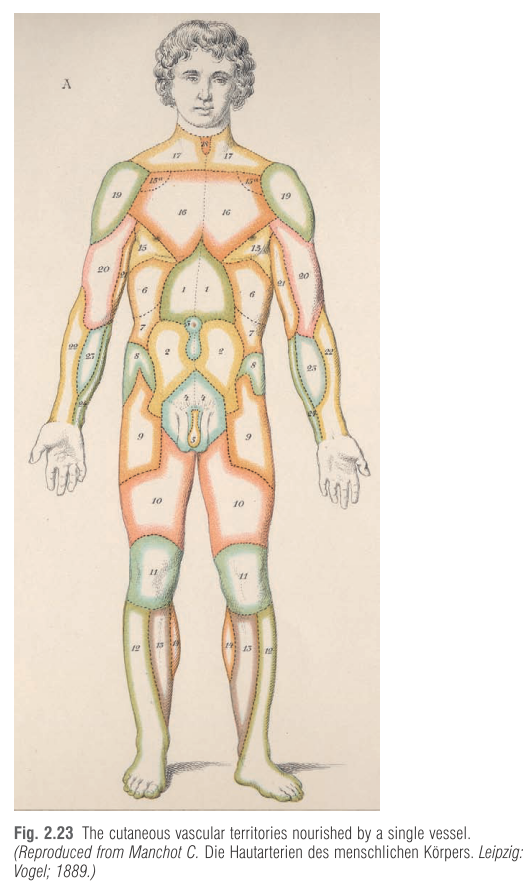
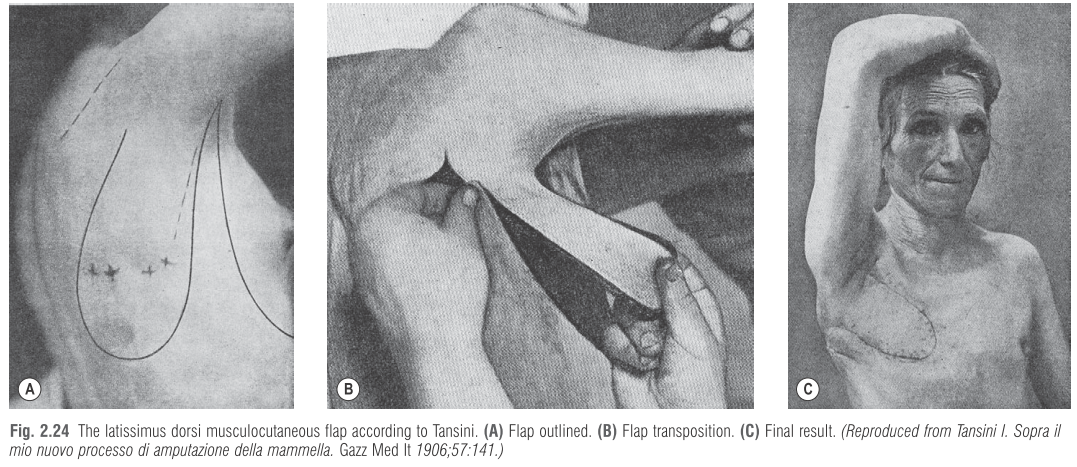
Recent history sees an incredible development of new reconstructive procedures, initiated in the 1960s with the recognition of arterialized flaps, continuing with the clinical definition of the cutaneous vascular territories nourished by a single vessel, first identified by Carl Manchot (1866–1932) in 1889 (Fig. 2.23), and culminating with their microvascular transfer. The application in surgical practice of musculocutaneous flaps, originally described by the Italian Iginio Tansini (1855–1943) 56 (Fig. 2.24), the introduction of craniofacial techniques, developed in the late 1960s by Paul Tessier (1917–2008), 57 the systematization of breast reconstruction, the use of fat grafting for numerous aesthetic and reconstructive indications, and even the most recent face transplantation, constitute further achievements of our specialty.
Aesthetic Surgery and Its Evolution
Aesthetic surgery's roots are cataloged back to the mid-19th century, evolving with increasing patient attention and procedures expanding to encompass various body parts, often culminating in significant societal implications regarding appearance. From early cosmetic procedures to modern-day interventions, the demand for enhancing or altering appearance has continuously shaped the field.
In Europe, aesthetic rhinoplasty started in Berlin, in about the same period, with Jacques Joseph (1865–1934), who codified the steps of the technique
in a rigorous sequence, still used today after almost 100 years, with minimal variations.
The problem of the beauty doctors -The real explosion of aesthetic surgery took place in Europe and in the US between the two world wars. To establish a barrier against beauty doctors and in an attempt to isolate them, true plastic surgeons, practicing reconstructive as well as aesthetic procedures, founded plastic surgical societies (see above). However, it was not an easy task because the general public was more interested in the achievements of cosmetic surgery than in the outcome of reconstructive procedures. An example is given by Charles C. Miller (1880–1950), regarded as an “unscrupulous charlatan” by some or “the father of modern cosmetic surgery” by others for having published in 1907 The Correction of Featural Imperfections, a pioneering work on aesthetic procedures, where facial operations, such as double-chin excision, eyelid and nasolabial fold modification, were illustrated. 67 Miller made extensive use of paraffin injections, considered the ideal filler for improving saddle nose and cutaneous depressions. When paraffin was abandoned because of devastating local and systemic sequelae (paraffinomas, pulmonary embolism, phlebitis), he replaced it with crude rubber mixed with gutta-percha and ground in a mill.
In Paris, Suzanne Noël (1878–1954), active feminist and founder of the Soroptimist Club of Europe, established a successful solo practice in the very exclusive 16th arrondissement. Her operations were simple but effective, mainly related to facial rejuvenation and entirely performed on an outpatient basis (Fig. 2.26). Major surgery, such as abdominoplasty or mammoplasty, was executed in a private clinic. In 1926, she published La Chirurgie Esthétique. Son Rôle Sociale, one of the first textbooks on this topic and the first written by a woman.
In Berlin, Jacques Joseph carried out a wide variety of cosmetic operations from rhinoplasty to reduction of prominent ears, facelifting and reduction mammoplasty. Eugen Holländer (1867–1932) is credited with being the first one who reported on a facelifting. “Victim myself of the art of feminine persuasion, a few years ago, I performed the excision of a piece of skin along the hairline and the natural folds of the ageing wrinkles and I rejuvenated the drooping cheek for the satisfaction of the beholder”.
Management of the hypoplastic breast - Over the years it was treated with paraffin, sponge implants, fat grafts, and liquid silicone, with poor or unpleasant results. In the mid-1960s the silicone mammary prosthesis appeared on the market, representing the first convincing solution. Liposuction, introduced in the mid-1980s, soon became one of the most popular procedures. Faceliftings, fillers, botulinum toxin, and fat injection favorably improved the demand for facial rejuvenation.