Block 2: Back and Thorax
Back
Know the primary and secondary curvatures of the spine, as well as the number of vertebrae in each curvature. For the secondary curvatures, at what age do each develop?
cervical curvature (concave): 7 vertebrae, C1- C7
secondary: form when we are in infants and start to move, start picking up their head
thoracic curvature (convex): 12 vertebrate, T1-T12
primary: born with
lumbar curvature (concave): 5 vertebrae. L1-L5
secondary: when babes stand up
sacral curvature (convex): 5 fused vertebrate sacrum
primary: born with
coccyx: 4 fused vertebrae
Know the Clinical significance of the following: scoliosis, kyphosis, and lordosis
scoliosis:
abnormal curvature of the thoracic curvature,
spine is S or C shape
if caught during childhood can put on a brace
kyphosis:
thoracic spine curves outward
apart of the aging process
loss in muscle tonicity and tissue and bone age
lordosis:
“swoyvac“ lumbar spine curves inward
can be born with or do a lot of activities that manipulate the spine, like gymnasts
Know the common and unique characteristics for each type of vertebrae.
cervical vertebrate (smallest and lightest)
Ccervical vertebrae (smallest and lightest)
C3-C7
rransverse foramen
body is wider
spinous process is short and is bifid
vertebral foramen large and triangular
transverse processes
superior articular facets face superposteriosly
C1 (atlas)
lacks a spinous process
supports the skull
superior articular facets receive the occipital condyles
allows flexion and extension of neck (nodding yes)
lateral masses
anterior/posterior arch/tuberculate
C2 axis
has body and spinous process
dens (odontoid process)
formed the fusion of the body of the atlas and axis '
acts as a pivot for rotation of the atlas and skull
C3-C7
???
thoracic vertebrae
all articulate with ribs
heart shaped bodies from the superior view
each side of the body of T1-T10 bears demifacets for articulation with ribs
T1 has a full facet for the first rib
T10-T12 have only a single facet
spinous processes are long and point inferiorly
vertebral foramen are circular
transverse processes articulate with tubercles of ribs
superior articular facets point posteriorly, outwards
inferior articular facets point anteriorly, outwards
allows rotation and prevents flexion and extension
costo-vertebral joints:
the head of each rib articulates with 2 adjacent vertebrae and the disk between them
costo-transverse joints:
between the tubercle of the rib and transverse process of its own vertebra
lumbar vertebrae
bodies are thick and robust (weight of entire body)
transverse process are thin and tapered (not receiving ribs)
spinous processes are think and blunt and pointed posteriorly
vertebral foramina are triangular
superior and inferior articular facets directly medially
allows flexion and extension - rotation prevented
sacrum
shaped the posterior wall of pelvis
formed 5 fused vertebrae
superior surface articulates with L5
interiorly articulates with coccyx
sacral promontory
where the first sacral vertebrae bulges into pelvic cavity
center of gravity is 1cm posterior to sacral promontory
ala:
develops from fused rib elements
anterior sacral foramina:
spinal nerves passing through
coccyx
tailbone
formed from 3-5 fused vertebrae
offers only slight support to pelvic organs
Injury to coccygeal vertebrae
falling on buttocks, specially in females
painful delivery
coccydynia:
pain in coccyx
What are the contents of the following: vertebral foramen, intervertebral foramen, and transverse foramen of the cervical vertebrae?
vertebral foramen:
spinal cord
dorsal
ventral roots
meninges
CSF
fat
intervertebral foramen
spinal nerves branching off spinal cards
transverse foramen of cervical vertebrae
transverse foramina;
vertebral artery (pass through the 6 upper cervical vertebrae
enter skull through the foramen magnum (extra: converge and form the conbasler artery and participate in the formation of circle of willis and internal carotid artery)
What is the Clinical significance of the “Hangman Fracture?” Which specific vertebrae is effected?
hangman fracture:
when someone is hanged, at the end of rope= arch of axis pushes the dens posteriorly and compresses the brain stem which causes death.
fracture of dens is a common fracture of C2 when we have traumatic injury of the neck.
What is the function of the intervertebral disc? What does it mean for a disc to herniate? What is the most common site of herniation?
/
function:
acts as shock absorber
is compressible
permits slight degree of movement of the vertebrae over each other
makeup approx. 20% of the total length of the vertebral column (taller in the mornings)
herniation:
injury to the back, abnormal displacement of tissue
mostly posterolaterally where annulus fibrosus is thinner
four stages:
degeneration, prolapse, extrusion, sequestration
Know the location and function of the following muscles: trapezius, latissimus dorsi, and levator scapula.
trapezius:
location: either side of upper back
elevation, retraction, and rotation of scapula
helps in adduction and slight elevation of arm'
innervation: spinal root of accessory nerve and c3-c4
descending: from external occipital protuberance, superior nuchal line, and ligamentum nuchae
insertion: lateral 3rd of clavicle
transverse: from C7-T3 spinous process
insertion: to clavicle and scapula
ascending: from T3-T12 spinous process
insertion: spine of scapula
latissimus dorsi (coughing muscle):
location: on lower back, extending from below the shoulder balde down to teh pelvis
adduction and lowering the arm,
medial rotation and extension of the arm(humerus),
raises the body toward the arm when climbing
innervation: by thoracodorsal nerve C6,C7,C8
vertebral part T7-T12 spinous process
thoracolumbar part (from fascia)
lliac part (from iliac crest)
costal part: 10-12th rib
inferior angle of scapula
insertion: crest of the lesser tubercle of humerus
levator scapula:
location: runs from neck to the shoulder blade
elevates the scapula
innervation: innervated by dorsal scapular nerve C4-C5
the transverse process of C1-C4
insertion: superior angle of the scapula
Know the location, function, and innervation of the rhomboid major and minor.
location: located in the upper back
function: press the scapula to the thoracic wall, retraction of scapula medially
innervation: dorsal scapular nerve (C4-C5)
minor: spinous process of C6-C7
insertion: medial margin scapula
major: spinous process of T1-t4
insertion: median margin of scapula
Which muscles are included in the erector spinae? What are their locations?
intermediate intrinsic back muscles
lateral group muscles: iliocostalis lumborum, thoracis, cervicis; and longissimus thoracis, cervicis, capitas
medial group muscles: spinalis thoracis and cervicis (capitas might be missing)
What are the boundaries and contents of the suboccipital triangle?
boundaries: rectus capitis posterior major, obliques capitalist superior and inferior
contents: suboccipital nerve (dorsal ramus of C1), III part of vertebral artery, and occipital venous plexus
At what level of the vertebral column does the spinal cord end? How is this information relevant when performing a lumbar puncture?
spinal cords end at L1-L2= conus medullaris.
tapers off and spinal nerves come off of it called the cauda equina (horse hairs: course and thick)
spinal cord is anchored on the coccyx→ from a fine piece of pia mater.
lumbar puncture: done at L3-L5 region.
the intercristal line (iliac crests) is at the level of L4 approximately (safe region).
here you collect the CSF (do not try to puncture spinal cords because it will severe axons) at this safe spot L4.
On the vertebral column, where is the site for epidural anesthesia? Why would this be given?
caudal epidural: given at sacral hiatus point, and diffuse into S1-S2 region.
why: for labor and delivery, the nerve in the primnimeal area; pudendal nerve that innervates the muscles of the pelvic floor.
manage pain and block pudendal nerves.
given through knee scoping and awake
epidural anesthesia: is given through the sacral hiatus to block pelvic nerves
also given through knee scoping and awake, pain management technique
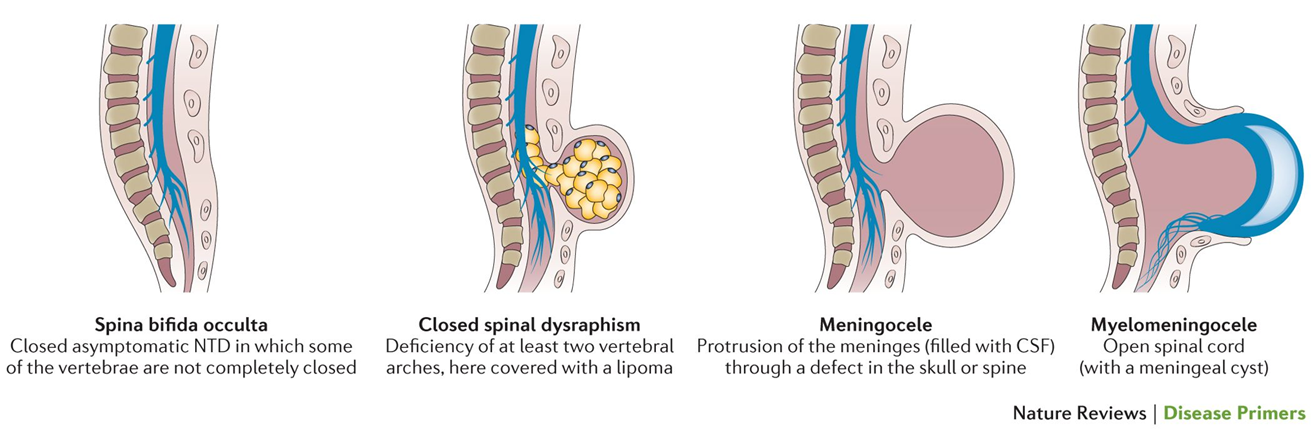
What is the Clinical significance of spina bifida and spina bifida occulta?
spina bifida occulta:
folic acid substitution in conception and during pregnancy decreases the risk of spina bifida.
closed asymptomatic NTD in which some of the vertebrae are not completely closed.
Thorax
What is the Clinical significance of fractures in the 1st, middle, and lower rib cage?
first rib:
superior surface and 2 grooves for subclavian artery + lower brachial plexus and subclavian vein
is atypical bc its flattened from the superior to inferior and is quite board bc its flattened from the superior to inferior and is quite broad
rarely fractured (danger to vessels) typically the clavicle would be fractured as well if the first rib was fractured
middle rib:
most commonly fractured
lower rib:
may damage the pleura and abdominal viscera(kidney,liver,spleen)
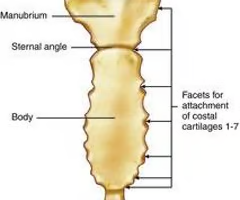
Know the parts of the sternum and rib. For the rib, know which structures articulate with the body and transverse process of the vertebrae.
sternum:
top part: the manubrium, the line that cuts: sternal angle
middle part: body, then the bottom piece will be the xiphisternal joint attaching to the xiphoid process
ribs:
12 ribs in total 7 true 5 false ribs 11th & 12th are floating ribs
the tubercle of the rib articulates with the transverse costal facet or the transverse process of the same thoracic vertebra of the same number.
the head of the rib articulates with the superior costal facet that is on the body of the vertebra

Which muscles elevate the thoracic cage?
scalene muscles (posterior, anterior, and middle)
pectoralis major/minor
sternocleidomastoid

In regards to the ribs, where is the location of the intercostal vessels and nerves? What is the Clinical significance of this information?
location: intercoastal groove therefore each of the muscles has a nerve that innervates them. the intercostal vessels pass beneath the inferior border of the ribs
clinical significance:
coarctation of aorta:
all theses arteries are dilated (eben braches off the subclavian artery)
IMA is associated with coarctation of the aorta because it is one of the 3 branching points that can become dilated
any structures that it would give blood to can be compromised due to the increase in the pressure
thoracentesis:
produce performed due to the increase of fluid in thoracic, involves using a needle to extract fluid
Know the internal structures of the breast, including the importance of the retromammary space and suspensory ligaments.
internal structure:
situated in the superficial fascia and is separated from pectoral muscles by a deep (pectoral) fascia
composed of lobules of 15-20 glandular tissue (mammary gland); each lobule is drained by a lactiferous duct which opens into the nipple
lactiferous sinus
mammary gland is an apocrine gland (modified sweat gland)
during puberty, the lactiferous ducts undergo branching; an increase in fat deposition leads to breast enlargement
retromammary space
between the breast and deep fascia, a tumor here may contract the pectoralis major
suspensory ligaments
extend from the skin to deep fascia and support the breast; their invasion by tumor may cause dimpling of skin PROVIDES SUPPORT FOR BREAST
Which hormones are responsible for breast growth, and what specific structures are under the influence of each?
estrogen:
growth of tubular system which is the lactiferous ducts
estrogen coming from ovaries helps develop the tubular system
progesterone:
development of milk secreting lobules which is seen durong post ovulation and pregnant women
What is the Clinical significance of the following: Breast cancer, mastectomy, and gynecomastia?
breast cancer:
cancer can be indicated by what is called orange peel: this is dimpling (invagination) thickening of the skin especially if the lymphatic system is blocked
blockage due to suspensory ligaments are being pulled on, invasive resulting in blockage of lymphatic drainage
mastecomy:
is the removal of breast the long thoracic nerve (holds scapula in place) could be in danger which results in "winged scapula"
lumpectomy: most of the time if the cancer lump is removed via lumpectomy. specimen sent off to pathology in order to determine if margins are clear in order to make sure they got all of the cancer, whereas a biopsy (needle biopsy) is different.
gynecomastia (Klinefelter syndrome):
XXY; most common congenital cause of infertility in males
What is the Clinical significance of a sucking and tension pneumothorax?
sucking:
air enters and leaves the pleural cavity; mediastinal flutter \
mediastinal flutter (mediastinum shifted toward the normal side in inspiration and to the injured side in expiration)
tension:
air enters the pleural cavity but not leaving it
mediastinal shift: the mediastinum is shifted toward the normal side, increased intrathoracic pressures
patient has dyspnea and/or cyanosis
hyper-resonant percussion tone, radiolucent area in lung, in radiography
Know the types of pleural effusion: hydrothorax, pyothorax, chylothorax, and hemothorax.
pleural effusion: fluid in the pleural cavity
hydrothorax:
congestive heart failure
pyothorax:
infection pus
chylothorax:
injury to thoracic duct
hemothorax:
blood in pleural cavity
injury to right subclavian vein during catheterization
What is the Clinical significance of pleuritis and thoracocentesis?
pleuritis (pleurisy): inflammation of the pleura
pain only if parietal pleura is involved, not the visceral layer
puncturing the intercostal space: always go superior to the inferior rib
thoracocentesis (pleural tap): a procedure to drain pleural fluid in pathological conditions, performed posterior to the midaxillary line while patient is seated
first determine the fluid level by percussion and go 1-2 intercostal spaces below the fluid level but, not below the 9th intercostal space (danger to injure the liver on the right side)

Know the innervation of the lungs.
sympathetic: from 5-6 upper thoracic
segments; postsynaptic fibers end on SA and AV nodes
action: increases heart rate and contraction force, coronary dilatation
parasympathetic: vagus nerve terminates on many small ganglia on the heart
action: decreases heart rate and force and vasoconstrictor coronary arteries
Know the tracheal divisions and bronchopulmonary segments within each lung, noting any unique features.
trachea: main bronchus and lobar bronchi
is 12 cm long and 2 cm wide, from C6 to T4
trachea contains C-shaped cartilage rings, posteriorly, it has the muscle layer covered by the mucus membrane
trachea divides to:
main bronchi (primary bronchus) at T4 (sternal angle), carina; right main i shooter (2.5 cm), wider and more vertical; left main is longer (5 cm), less steep
main bronchi divide into: lobar bronchi (secondary bronchus)
lobar bronchi divide into segmental bronchi (tertiary bronchus)
bronchopuolmonary segments (10 on each side)
segmental bronchus
branch of pulmonary artery
branch of bronchial artery
tributaries of the pulmonary vein are found in the periphery between the adjacent bronchopulmonary segments
surgical landmarks
Understand the process of gas exchange within the lung in regards to the blood-air barrier
little sacs called alveoli → oxygenated air fills the little alveoli and each sac has a branch of artery and a branch of vein interacting with it.
fluid in sacs called surfactant secrets by an air cell, secretes the surfactant (because water is the universal solvent) so it makes easier gas exchange if dissolve gas in water to get across the blood air barrier.
passive diffusion where gas exchange goes from higher concentration to lower concentration.
oxygen is higher in the alveoli so it moves from the alveoli in higher concentration to the blood where it is in lower concentration.
carbon dioxide goes from higher concentration to lower concentration
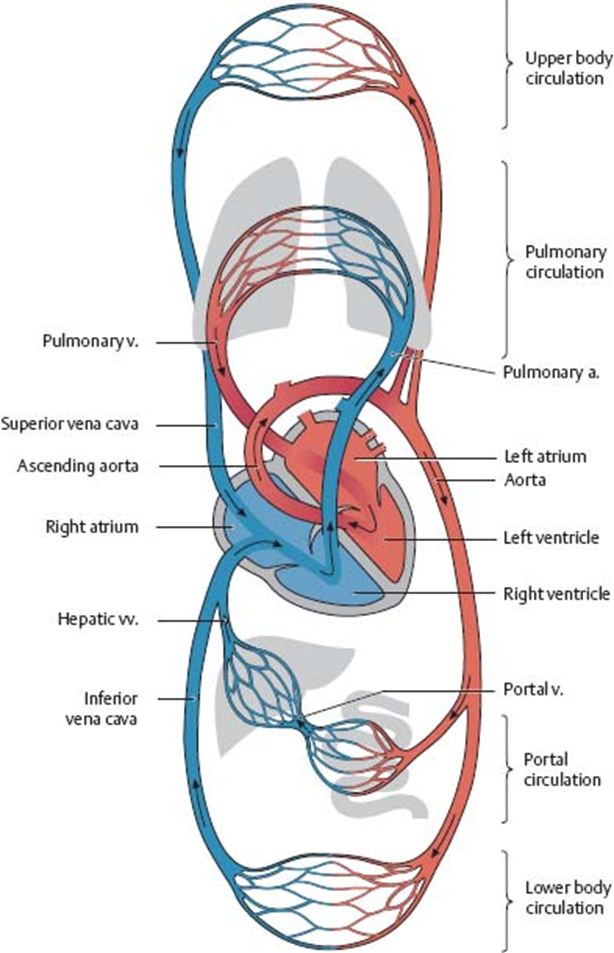
Know the pulmonary circulation pathway
deoxygenated blood from the right ventricle of the heart goes into the pulmonary trunk and pulmonary arteries and to the right and left lungs; blood is oxygenated and comes back to the heart (the left atrium), usually by means of 2 pulmonary veins.
Know the layers of pericardium and heart wall
pericardium- double wall of serous membrane covering the heart; 1-fibrous 2-serous
serous membrane- two layers A-parietal, B-visceral
pericardial cavity- space between the two layers of serous membrane, contains pericardial fluid
visceral pericardium (epicardium)- closely attached to the heart
3 layers:
epicardium
myocardium (main mass)
endocardium
What is the Clinical significance of the following: pericarditis and cardiac tamponade?
pericarditis: inflammation of the pericardium, usually from infection. swells and rubs against the heart that caused severe pain, friction rub
cardiac tamponade: occurs when you have a heart attack and is quite severe bc it was built up, coming up for awhile bc there is blocked coronary arteries, death of cardiac cells, so when it happens the heart wall splits, so blood is coming from inside one of the chambers and out. Then blood fills the pericardial cavity sac and impedes the heart beating. Can remove the fluid with a pericardiocentesis: 5th or 6th left intercostal space near sternum
Know all the branches of the left and right coronary arteries.
coronary arteries: functional end arteries
right coronary artery: supplies right atrium
right marginal artery: supplies both ventricles
posterior interventricular artery: supplies both ventricles and posterior part of interventricular septum
left coronary artery:
anterior interventricular artery: supplies both ventricles and interventricular septum
circumflex branch: supplies the left atrium, left surface of the heart, and let ventricle
left marginal artery: a branch of circumflex artery, supplies left ventricle
in 40% cases, the SA node and eve AV node and bundle of HIS are supplied by left coronary artery
Know the venous drainage of the heart.
the main cardiac veins drain into coronary sinus:
great cardiac vein: lies in the anterior interventricular groove
middle cardiac vein: lies in the posterior interventricular groove
small cardiac vein: lies in right coronary groove (2 and 3 drain most of the right coronary artery blood)
posterior vein of the left ventricle: on inferior and posterior surface
left marginal vein
anterior cardiac veins: (several on the right ventricle) usually enter the right atrium
smallest cardiac veins (thesbesian veins): begin in the myocardium and open directly into heart chambers, mainly atria; also carry blood to the myocardium
Know the blood flow pathway through the heart. Be able to identify each structure that blood would pass as it travels through the heart.
superior/inferior vena cava or coronary sinus → right atrium → right ventricle through tricuspid valve → go through pulmonary valves into pulmonary trunk → pulmonary arteries that branch into the left and right lungs → red blood cells go to alveoli, release carbon dioxide and pick up oxygen → pulmonary veins bring blood back to heart from the lungs → coming into left atrium into bicuspid/mitral valve into left ventricle → goes into aortic semilunar valve → enters systemic circulation into aortic valve
What is the Clinical significance of rheumatic fever?
acute inflammation as a result of complication of chronic tonsillitis or pharyngitis by streptococcus infection
characterized by arthritis, chorea, skin involvement (erythema), subcutaneous nodules, and carditis
nodules on the valve cause irregular blood flow, valvular incompetence (blood regurgitation causing murmur
may cause stenosis (mitral stenosis)
Know the conduction system pathway of the heart.
1. intrinsic impulse- conducting system of the heart: heart contains a specialized muscle tissue (the impulse conducting system) which spontaneously generates rhythmic impulses
2. sinus (sinoatrial) node (keith flack node): pacemaker (impulse frequency:70)
network of muscle cells
lies anterior margin of orifice of SVC, from which the impulse reaches the AV node
3. atrioventricular (aschoff tawara) node: situated in right atrium (interatrial septum) on the ventricular side of orifice of coronary sinus (impulse frequency: 50-60/min)
4. bundle of his (atrioventricular bundle): runs through the interventricular septum beneath the endocardium to the base of pupillary muscles (impulse frequency: 25-45/min)
5. purkinje fibers:terminal fibers of the bundle of His, merge with the cardiac muscles
What are the disorders of the conduction system
arrythimas: variation from normal heart rhythm
ventricular fibrillataion: rapid, random firing of electrical impulses in the ventricles
atrial fibrillation: impluslses circle within atrial myocardium, stimulating AV node
What are the innervations of the heart?
Sympathic: from 5-6 upper thoracic segments; postsynaptic fibers end on SA and AV nodes
Action: increases heart rate and contraction force, coronary dilatation
Parasympathic: Vagus nerve terminates on many small ganglia on the heart
Action: decreases heart rate and force and vasoconstrictor coronary arteries
What structures would be found in the supracardiac mediastinum?
mediastinum- the space between the right and left lungs
5 layers of structures:
thymus
great veins related to heart, the phrenic nerves, the thoracic duct and lymphatic trunks
arch of aorta including its branches and the vagus nerves,
sympathetic and parasympathetic nerves to the heart (cardiac plexus)
trachea and its bifurcation
esophagus, the recurrent laryngeal nerves
Know the Congenital Heart Defects
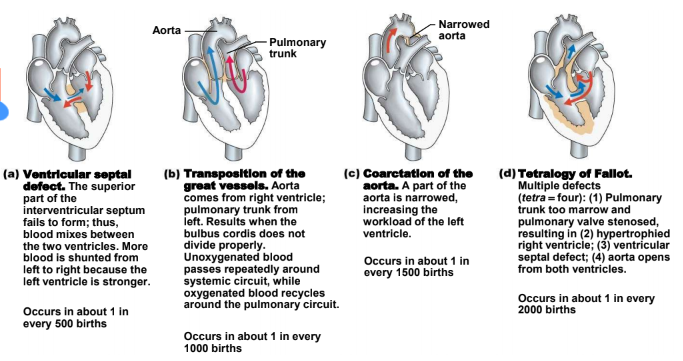
Ventricular septal defect.:
The superior part of the interventricular septum fails to form; thus, blood mixes between the two ventricles. More blood is shunted from left to right because the left ventricle is stronger. 1/500
Transposition of the great vessels;
Aorta comes from right ventricle; pulmonary trunk from left. Results when the bulbus cordis does not divide properly. Unoxygenated blood passes repeatedly around systemic circuit, while oxygenated blood recycles around the pulmonary circuit. 1/1000
Coarctation of the aorta:
A part of the aorta is narrowed, increasing the workload of the left ventricle. 1/1500
Tetralogy of Fallot.:
Multiple defects (tetra = four): (1) Pulmonary trunk too marrow and pulmonary valve stenosed, resulting in (2) hypertrophied right ventricle; (3) ventricular septal defect; (4) aorta opens from both ventricles. 1/2000