Vitamin D and Calcium notes
Calcium
Sources and function:
Mineral critical for various bodily functions including bone health, muscle function, nerve transmission, and hormone secretion.
Strict blood levels are maintained through interplay between bone reservoir, kidney and thyroid gland.
→ 1% circulating in blood, 99% in bone reservoir
Sources include dairy products like milk, cheese, and yogurt which are rich sources of calcium.
Other sources include leafy green veg (e.g. kale, broccoli), fortified foods (e.g. plant based milk, fortified cereals), and certain fish (e.g. sardines, salmon with bones).
Most adults need 700mg per day
The role of calcium in the body:
Ca forms crystalline structure to form bone.
Regulates muscle contraction including cardiac contractions.
Transmission of neuronal signals → Helps to transmit electrical signals between nerve cells.
Supports blood clotting.
The skeleton acts as a reservoir for calcium helping to maintain its levels in the blood within a narrow range.
Inadequate calcium intake can lead to osteoporosis, a condition characterised by bones prone to fractures.
Calcium physiology:
Kidney - reabsorb filtered calcium and is involved in processing vitamin D.
Bone - reservoir for calcium, can be reabsorbed and deposited depending on bodies needs.
Thyroid - releases parathyroid hormone and calcitonin to regulate blood Ca levels.
Calcium homeostasis:
Parathyroid hormone (PTH):
Bones: PTH stimulates the release of calcium from the bones where it is stored in the form of hydroxyapatite crystals.
Kidneys: PTH enhances the reabsorption of calcium in the kidneys preventing its loss in urine. It also circulates the production of active vitamin D (calcitriol), which enhances intestinal absorption of calcium.
Intestines: Through the action of calcitriol, PTH promotes the absorption of dietary calcium in the intestines.
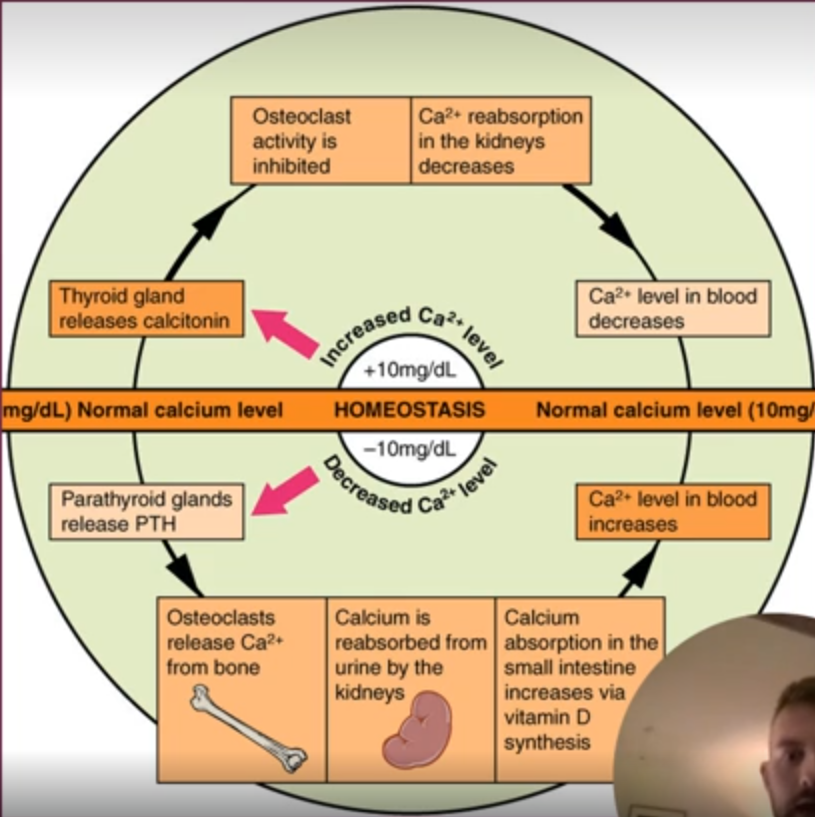
When blood Ca level elevated:
Calcitonin is released which inhibits bone resorption by osteoclasts, promoting Ca deposition in bones.
Kidneys increase calcium excretion, helping lower blood Ca levels.
When blood Ca levels low:
kidneys reduce Ca excretion to conserve Ca.
Factors affecting Ca absorption:
Vit D plays crucial role in Ca absorption. Without sufficient Vit D, Ca absorption is impaired.
Optimal Vit D levels are necessary to increase the efficiency of Ca absorption. Without adequate Vit D, body absorbs no more than 10-15% of dietary Ca.
Other factors influencing absorption include age (tends to decrease with age), dietary components (e.g. oxalates and phytates can bind to Ca and inhibit absorption), and certain medications (e.g. corticosteroids).
Vitamin D
Fat soluble vitamin used by body for normal bone development and maintenance by increasing the absorption of Ca, Mg, and PO4.
Unique as our bodies can synthesise it when exposed to sunlight. Besides role in Ca absorption, it is also essential for immune function, cell growth, reducing inflammation.
Many individuals have inadequate Vit D levels especially those living in regions with limited sunlight exposure or spending most of time inside.
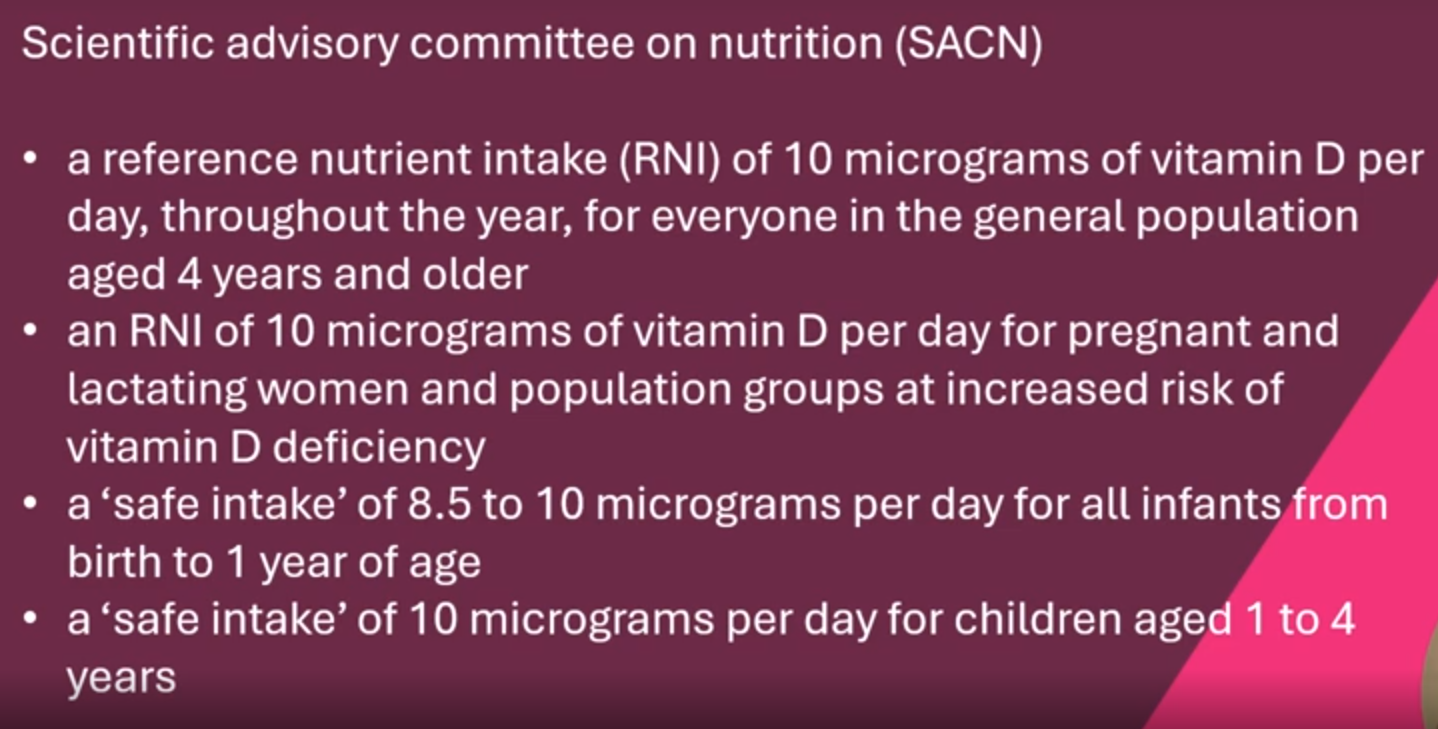
The Scientific Advisory Committee recommends 10ug per day for adults.
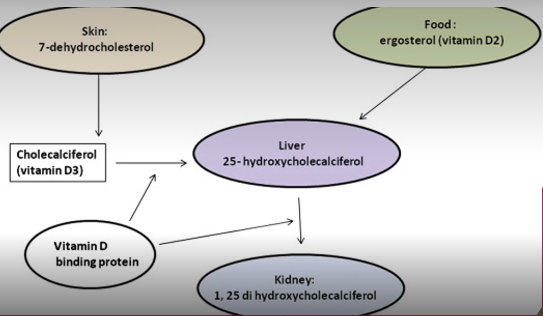
Vitamin D processed in body through liver and kidney to produce active form of Vit D within our small intestine where it can support ingestion of Ca through diet.
Sources of Vitamin D
Dietary sources:
Fatty fish (e.g. salmon, tuna, mackerel) ad fish liver oils are among the best dietary sources of Vit D.
Some foods are fortified with Vit D, such as fortified dairy products, orange juice, and cereals.
However, it is challenging to obtain enough through diet alone, especially within certain pops.
Calcium deficiency
Osteoporosis is a state of reduced bone mineral density that weakens bones and makes them susceptible to breaking.
Bone loss before the stage of osteoporosis is called osteopenia.
Additionally, Ca deficiency can result in muscle weakness/cramps, fatigue, paraesthesia, poor appetite.
Those at risk include post menopausal women, malabsorptive conditions (IBD, coeliac), breastfeeding women, vegans.
Hypocalcaemia - bone pain, osteoporosis, fatigue, confusion, memory problems, depression, nausea, vomiting, weight loss, thirst, polyuria, abdominal pain, renal colic and more.
Vitamin D Deficiency
Rickets in children (soft and weakened bones, fractures, bone and muscle pain, bony deformities) and osteomalacia in adults.
Causes:
Decreased dietary intake and/or absorption
Decreased sun exposure
Decreased endogenous synthesis
Increased hepatic catabolism
End organ resistance
→ At risk populations: elderly, obese patients, nursing home residents, hospital patients, those with darker skin, those who cover skin when outside.
Interactions:
Calcium salts reduce absorption of bisphosphonates, tetracycline antibiotics, levothyroxine, quinolone antibiotics, zinc ann iron.
Cardiac glycosides - Ca supplements can induce hypercalcaemia, which may enhance the effects of digoxin and other cardiac glycosides.
Systemic corticosteroids - absorption of Ca salts may be reduced by corticosteroids.
Thiazide diuretics - may increase urinary excretion of calcium
Fortification
Unlike other nutrients, there is no mandate in UK to fortify with Ca and Vit D however foods are commonly fortified with these nutrients.
Calcium fortification has been shown to be an effective strategy in improving the calcium intake of individuals, especially in non-dairy consumers.
Vit D fortification is particularly effective in raising Vit D levels among individuals with limited sun exposure.
Calcium homeostasis
Calcium absorbed in intestine and excreted via kidneys. Majority of Ca stored in body as calcium phosphate in bones and teeth.
Vitamin D elevates the amount of Ca and phosphate in the blood while PTH also increases Ca levels but decreases phosphate levels.
Calcium-sensitive receptors measure whether the right amount of extracellular Ca is in blood → Located primarily in renal tubular cells and the parathyroid gland.
Increase in serum Ca:
PTH secretion is inhibited but stimulates the release of calcitonin which ensures that less Ca absorbed from food and inhibits osteoclast activity and therefore the release of Ca and phosphate from bones and facilitates their excretion via kidneys.
Calcitonin can lower calcium and phosphate blood levels.
→ Used as therapeutic agent in hypercalcaemia.
Decrease in serum Ca:
Stimulates PTH secretion
Vitamin D facilitates osteoclast activity, which increases release of Ca and phosphate from bones
Blood Ca levels increase again
Calcium and Vitamin D Research and Guidelines
Research
Calcium and bone health:
Research has consistently shown that adequate Ca intake reduces risk of fractures, particularly in postmenopausal women and older adults (Reid et al. 2014). A study by the Cochrane Collaboration (2015) found that Ca supplementation reduces risk of fracture risk in individuals with low baseline Ca intake.
Vitamin D and immune function:
Vit D plays key role in modulating immune system. Recent studies suggest that adequate Vit D levels may lower risk of respiratory infections (Martineau et al. 2017). It is thought to be protective against autoimmune diseases like multiple sclerosis.
Ca and Vit D in Osteoporosis:
Combined supplementation of Ca and Vit D has been shown to reduce bone loss and fractures risk in postmenopausal women (Boonen et al. 2015)
Clinical Guidelines
UK NHS and Public Health England recommend that everyone should consider taking a Vit D supplement during winter months, particularly those with limited sun exposure.
Dietetic implications: Dietitians should asses Ca and Vit D exposure through diet history, clinical signs, biochemical tests (e.g. serum Ca and Vit D levels). Adequate intake should be encouraged, particularly in vulnerable groups such as elderly, vegans etc.
SACN recommendations
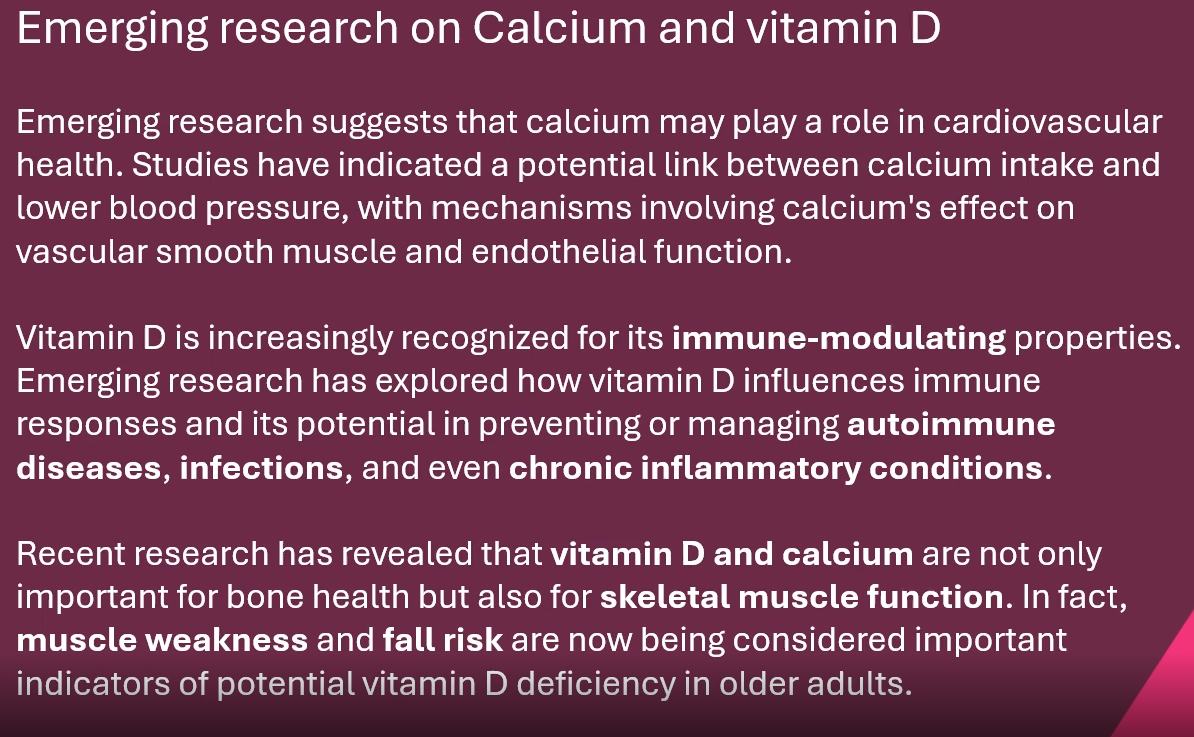
Emerging Research on Ca and Vit D
Considerations for dietetics:
Case Studies
Case Study 1: Elderly Woman with Osteoporosis
Background: An 80-year-old woman with a history of multiple fractures. She follows a pescatarian diet, has limited sun exposure, and is diagnosed with osteoporosis.
Intervention: Consider what dietary sources are rich in calcium that this client may be advised to consume. Consider what supplementation may be appropriate.
Ca Sources:
Oily fish - salmon, tuna, mackerel, sardines etc
Dairy products - yogurt, milk
Fortified products - cereals, tofu, dairy products
Vitamin D supplementation may be appropriate to maximise dietary Ca absorption.
Case Study 2: Vegan Patient with Deficient Vitamin D
Background: A 30-year-old vegan patient with symptoms of fatigue and low mood. Serum vitamin D levels are suboptimal.
Intervention: Consider what vitamin D-rich vegan foods (fortified plant milks, mushrooms) you may recommend and consider whether supplementation would be suitable for optimal vitamin D status.
Vegan Vitamin D sources:
Leafy greens - kale, brocolli etc
Orange juice
Fortified foods - cereals, plant milks
Supplementation would be appropriate.