Oral Biology OSPE Final Exam
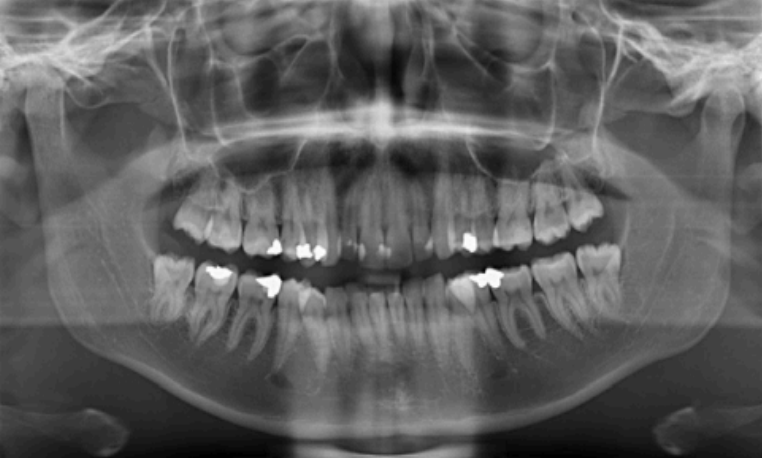
Age estimation using Panoramic Radiographs
Human dentition is divided into primary and permanent dentition
Primary dentition: your first set of teeth, also known as milk teeth or baby teeth, typically consisting of 20 teeth that emerge between 6 months and 3 years of age.
Permanent dentition: the second set of teeth that gradually replace primary teeth, usually consisting of 32 teeth, and typically begins to emerge around age 6 and continues into early adulthood.
4 teeth emerge for each 6 month of age:
By 5 months in utero, all crowns started calcification
By 6 months in utero: 4 teeth (lower centrals & upper central) begin eruption
By 12 months: 8 teeth (+upper laterals & lower laterals)
By 1 year old: all crowns completed formation
18 months: 12 teeth (+ upper 1st molars & lower 1st molars)
24 months: 16 teeth (+ upper canines & lower canines)
30 months: 20 teeth (+ lower 2nd molars & upper 2nd molars)
By 2.5 years, all primary teeth erupted
By 4 years old, all primary teeth completed root formation.
Age estimation chronologies are used for assessing unknown ages of patients and for forensic and archaeological applications.
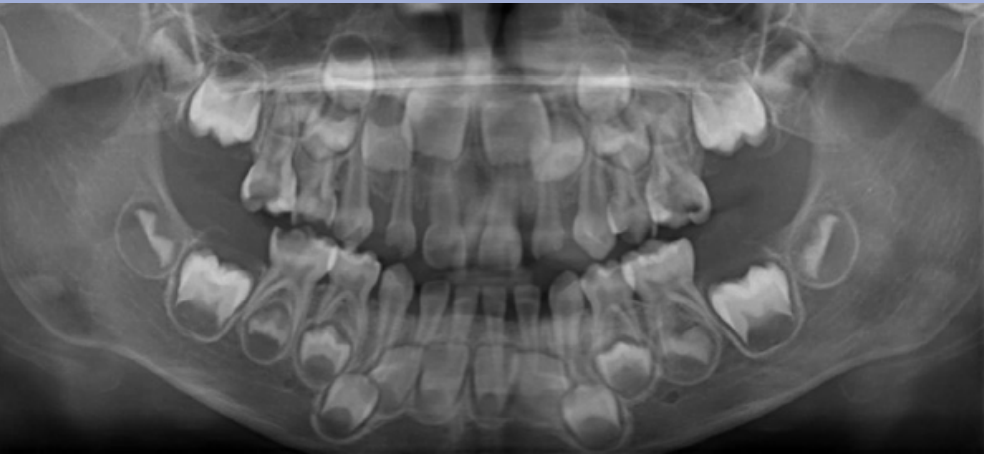
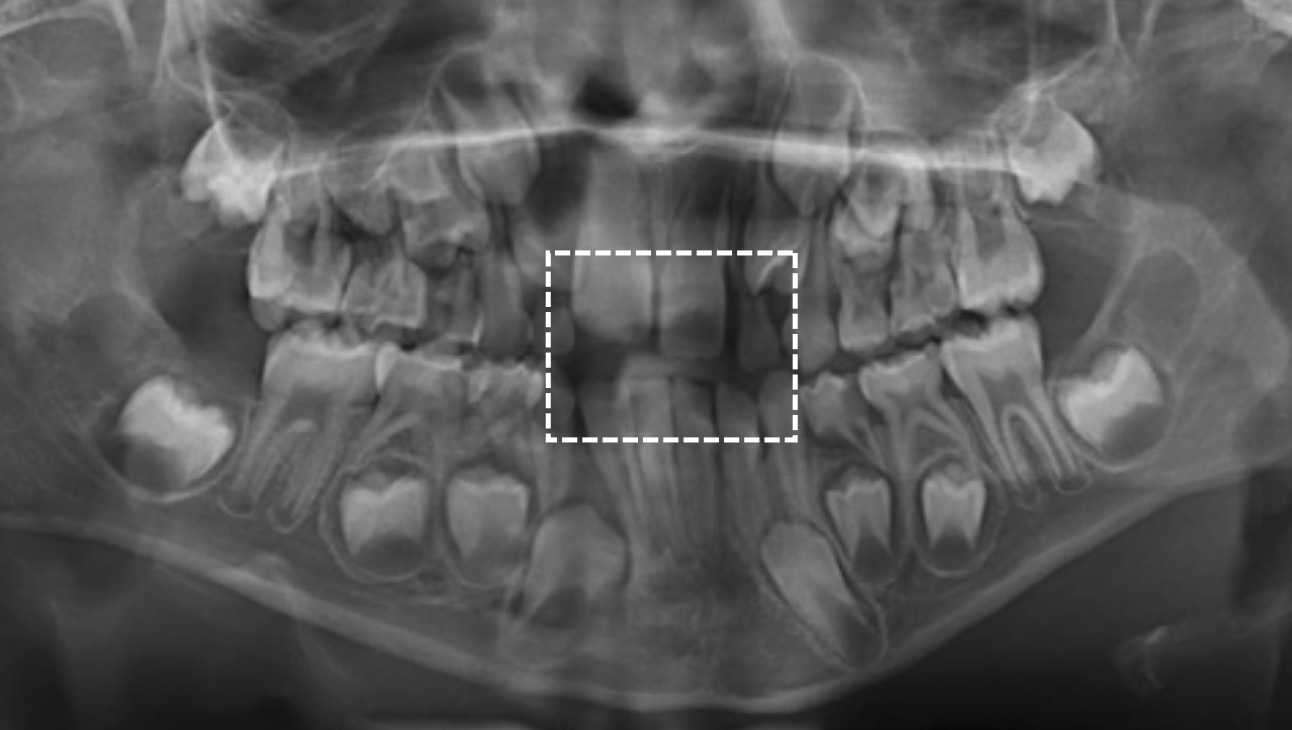
The age in this picture is characterized by the teeth erupted which are: Maxilla ABCDE and Mandible ABCDE. The teeth unerupted are the Maxilla 1234567 and the Second molar in the Maxilla- 1/3 Crown completed, Mandible- 1/3 crown completed
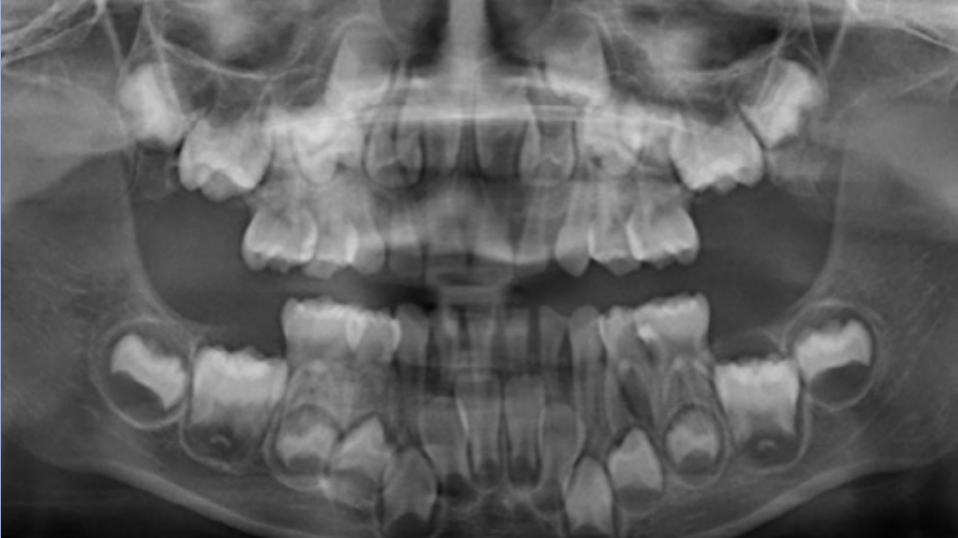
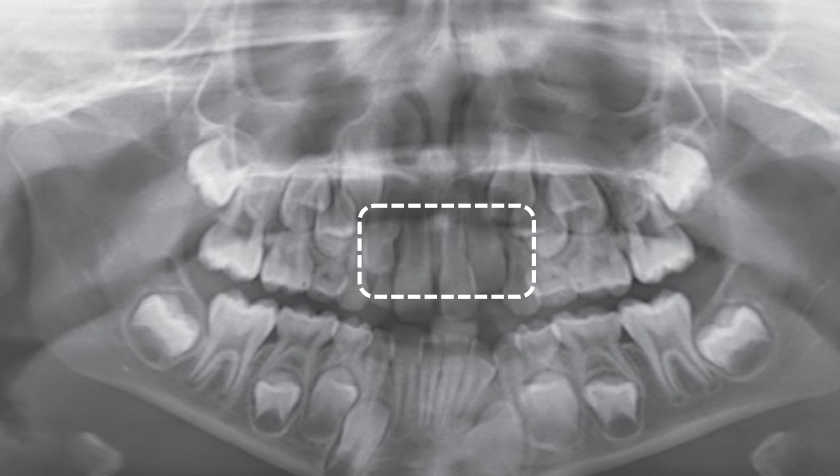
The age in this picture can be estimated by the erupted teeth which are: Maxilla ABCDE, Mandible ABCDE. The unerupted teeth are the Maxilla 1234567 and, Mandible 1234567 and the main identifying feature is the Second molar – Maxilla- 2/3 Crown completed, Mandible- 2/3 crown completed
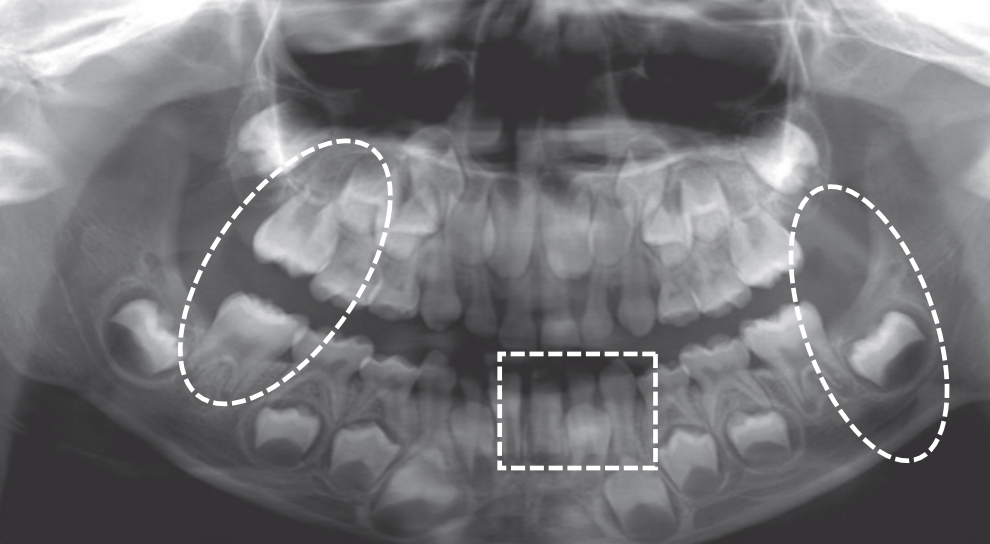
At age 6 is characterized by the erupted first molar in the maxilla, and the erupted central incisor and first molar in the mandible. Teeth erupted – Maxilla ABCDE6, Mandible 1BCDE6 - Teeth unerupted – Maxilla 123457, Mandible 23457
Dental age 7 is characterized eruption of permanent teeth Mandibular Lateral Incisor, Maxillary Central Incisor
Dental age 8 is characterized by eruption of the maxillary lateral incisors
Teeth erupted – Maxilla 12CDE6, Mandible 12CDE6
Teeth unerupted – Maxilla 3457, Mandible 3457
Dental age 9 the maxillary lateral incisors have been in place for 1 year, and
root formation on other incisors and first molars is nearly complete.
Teeth erupted Maxilla 12CDE6, Mandible 12CDE6
Teeth unerupted – Maxilla 3457, Mandible 3457
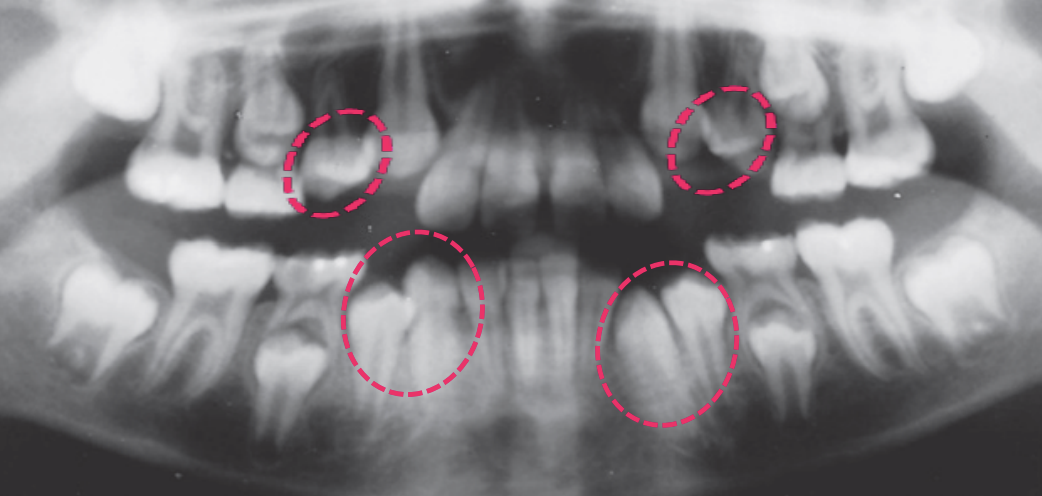
Dental age 11 is characterized by the eruption of the mandibular canines,
mandibular first premolars, and maxillary first premolars
Teeth erupted Maxilla 12C4E6, Mandible 1234E6
Teeth unerupted – Maxilla 3457, Mandible 57

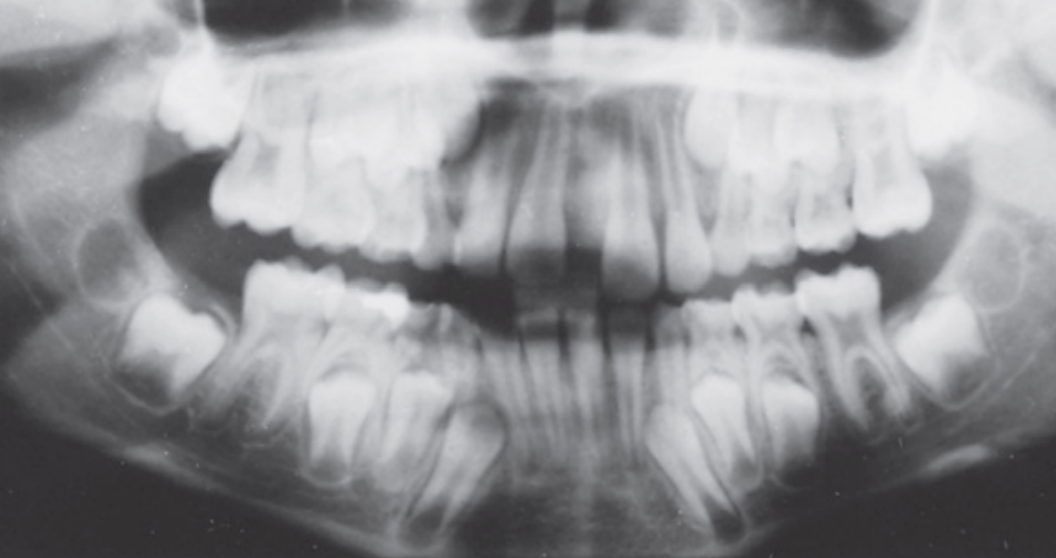
Dental age 12 is characterized by eruption of maxillary canine and the maxillary and mandibular second premolars.
Teeth erupted– Maxilla 1234567, Mandible 1234567
Teeth unerupted – all 2nd and 3rd molars

Dental age 15, the roots of all permanent teeth except the third molars are
complete, and crown formation of third molars
Dental age 21, all of the roots and molars are fully erupted
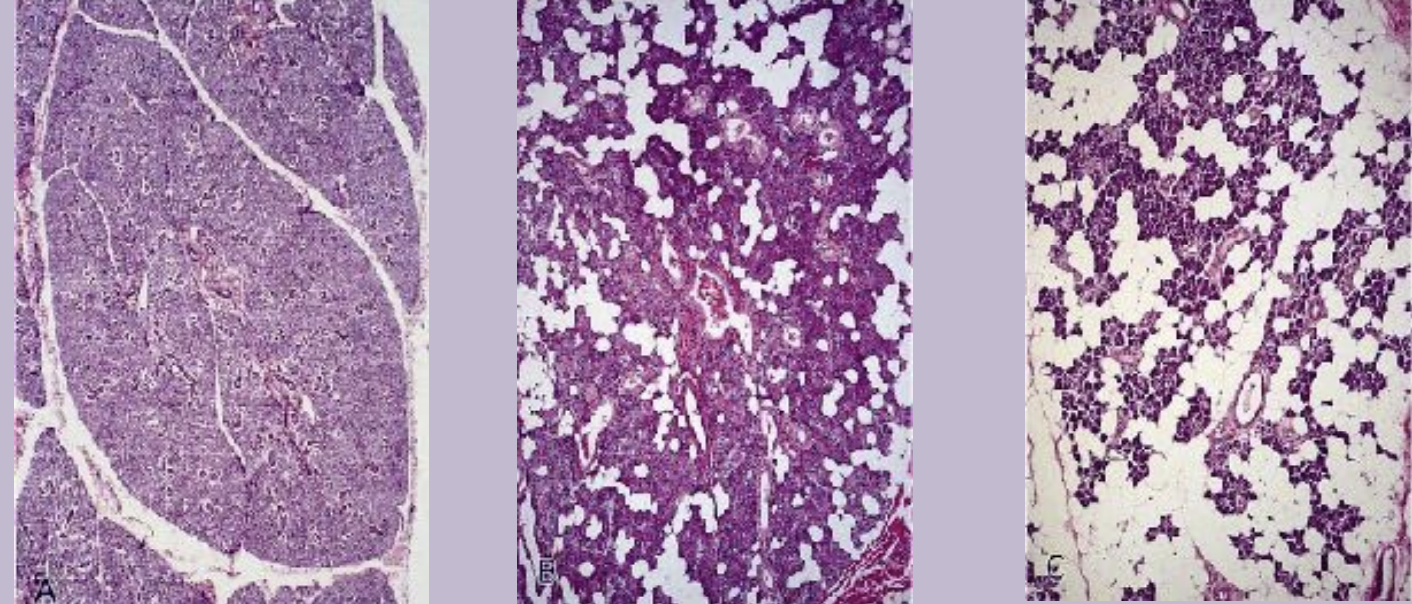
Salivary glands
Salivary glands are essental organs of the oral cavity that produce saliva fluid. They are merocrine and exocrine glands producing saliva. They contain specialized epithelial cells called glandular epithelial cells.
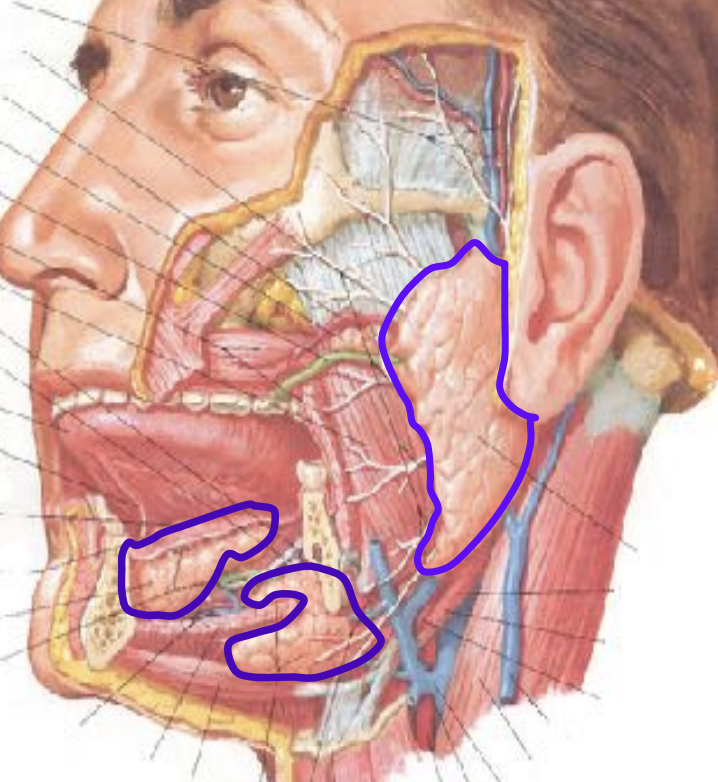
Major salivary glands:
Parotid gland
Submandibular gland
Sublingual gland
Minor salivary gland:
Minor salivary glands are way smaller than the major salivary glands and are located in the submucosa. They are not found within gingiva and anterior part of the hard palate.
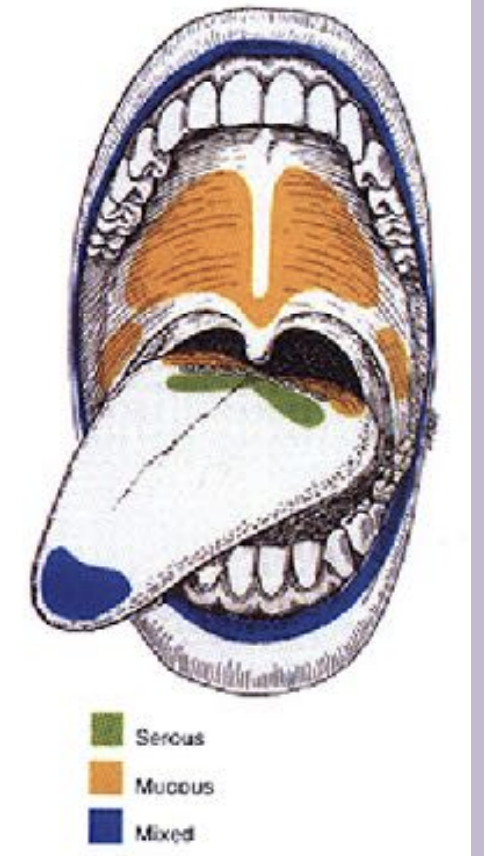
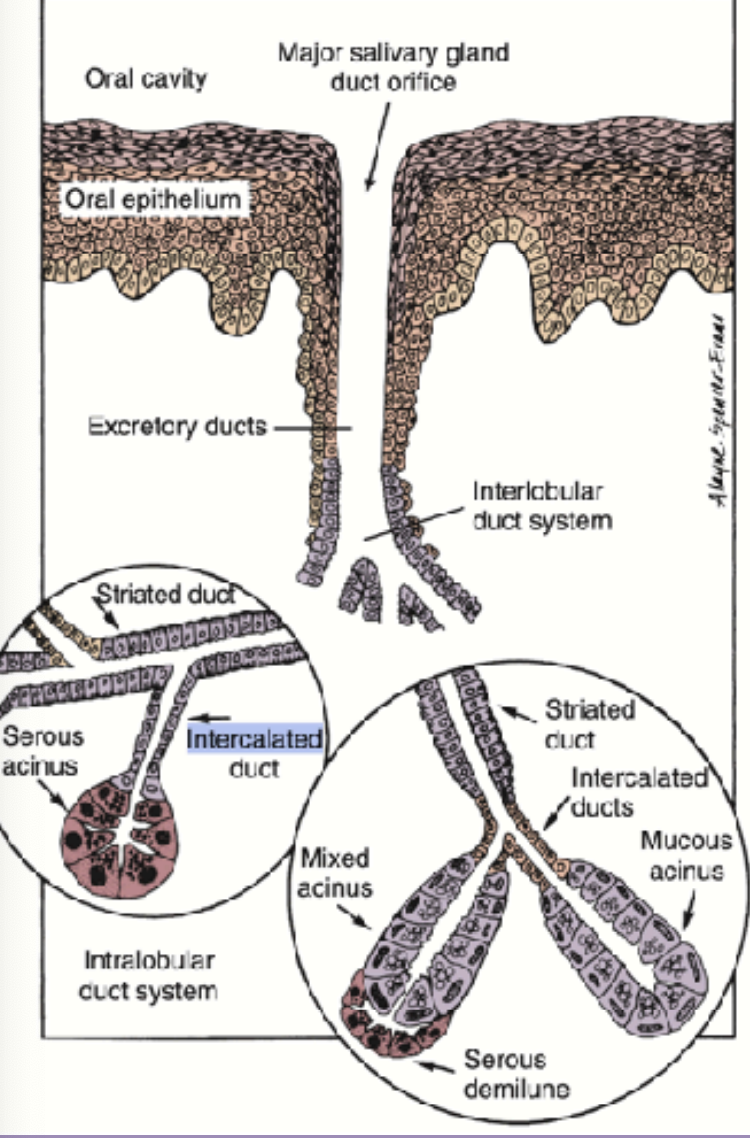
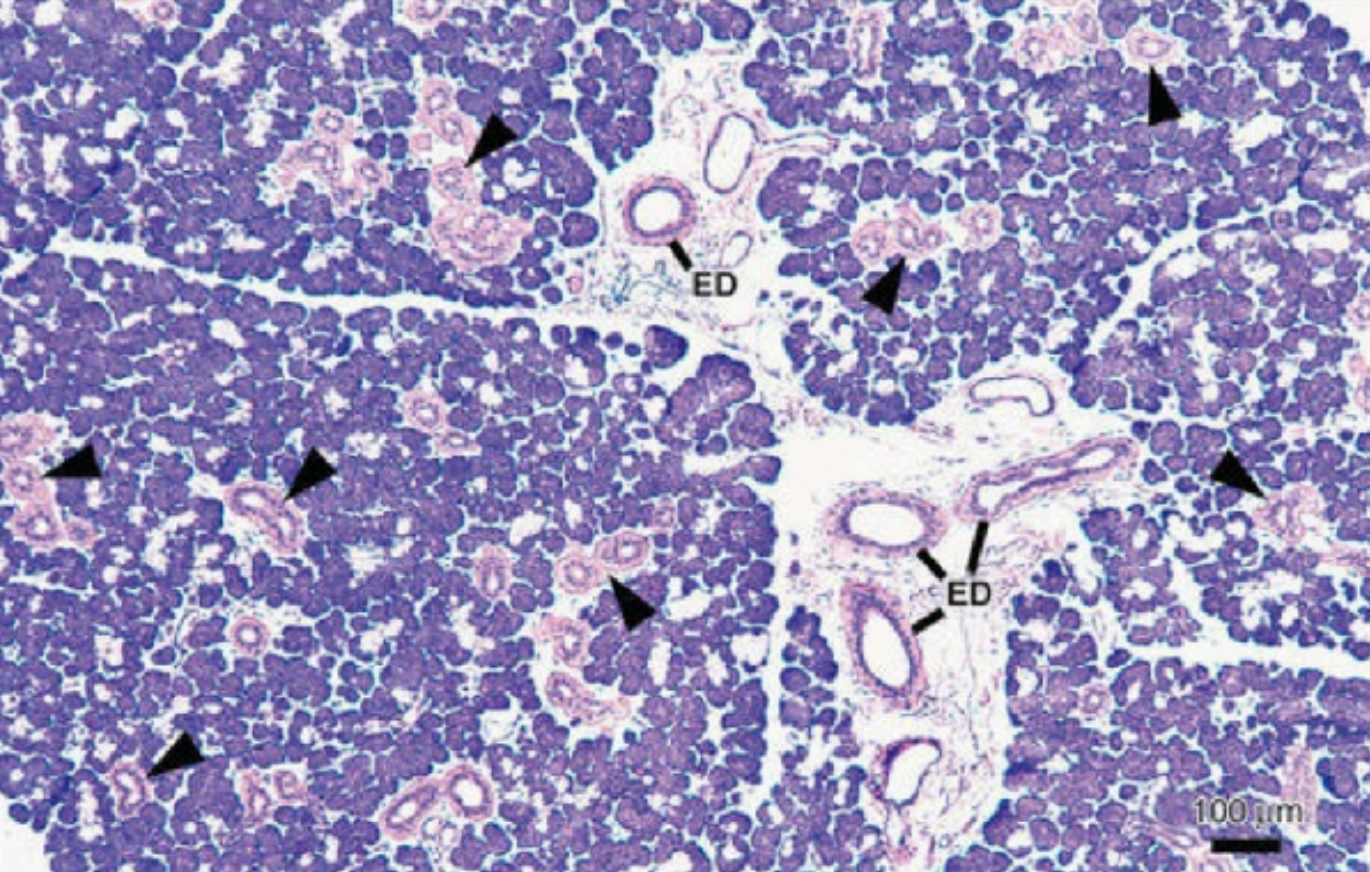
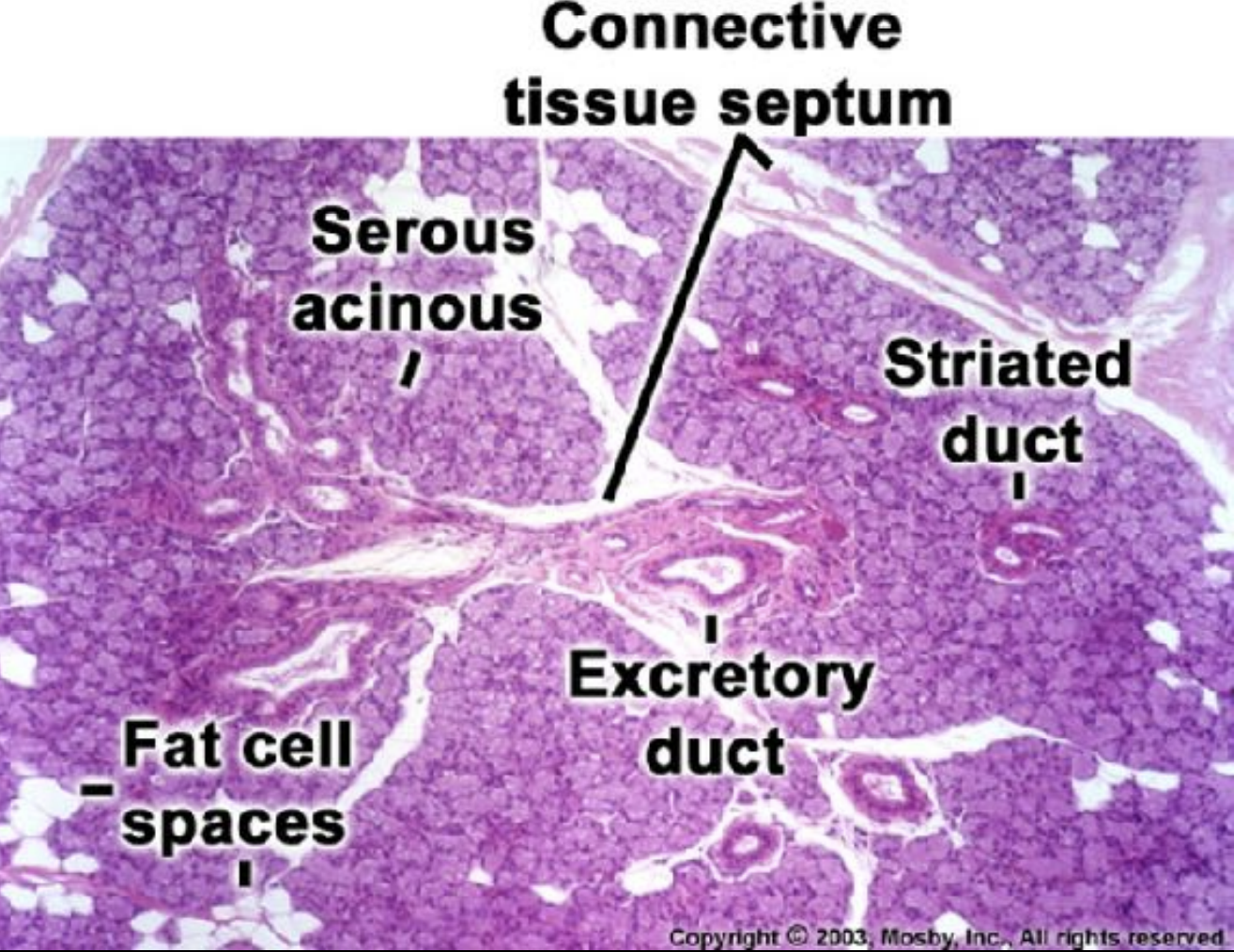
Structure of the salivary glands:
The functional unit of the salivary glands is acini (saliva).
Three types of salivary glands are: Serous, mucous, and seromucous (mixed)
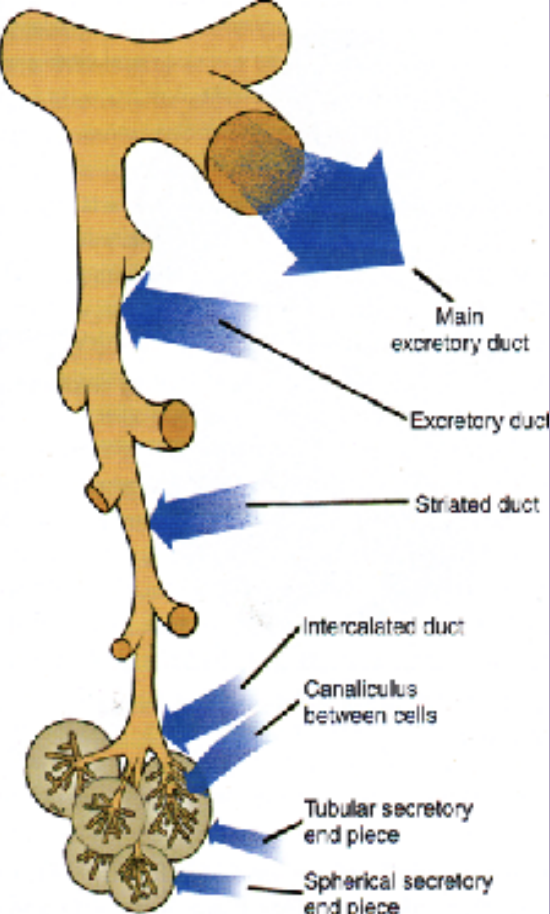
The secretion from the acini (saliva) first reaches the intercalated ducts and then into the striated ducts. these ducts are between the acini and so inside the lobular arrangment.
Finally the contents reach the collecting or exceratoey duct which are present in between the lobules called interlobular ducts
Ducts:
Execratory ducts
striated ducts
intercalated ducts
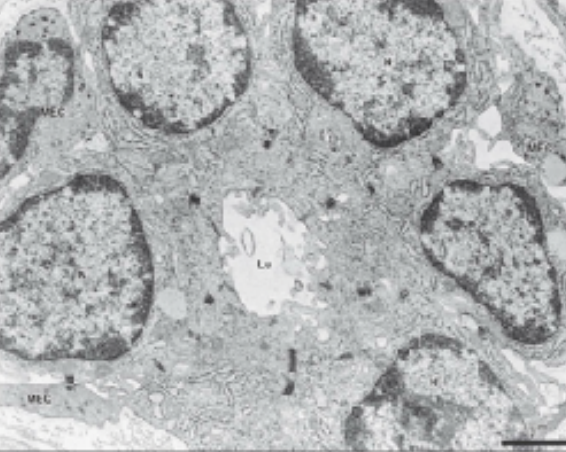
Secretory cells:
There are two main types of secretory cells:
Serous cells
Mucous cells
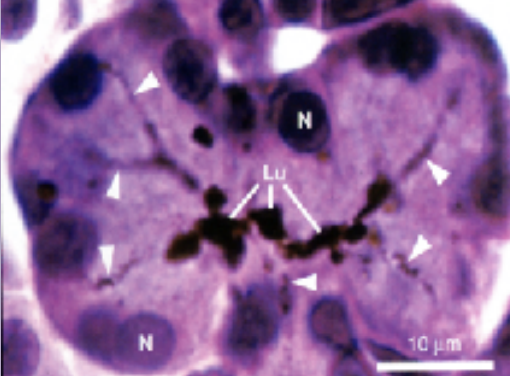
Serous cells:
8-12 cells surrounding central lumen
Pyramidal with broad base
spherical nuclei
Numerous secretory granules calles “zymogen granules”
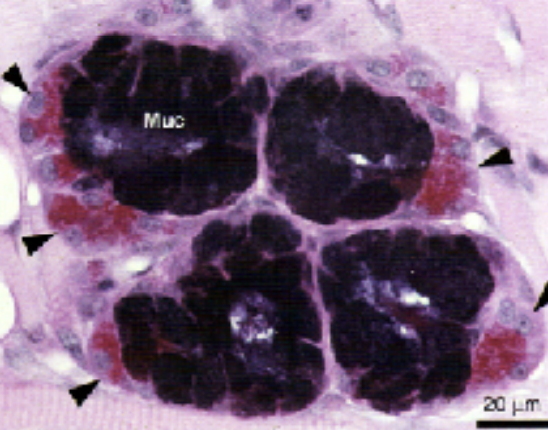
Mucous cells:
Have tubular configuration
mucous cells are larger than the serous
may have associated serous cells (serous deminiules)
Nucleus is flattened and compressed against the basal surface.
More cybrohydrates - mucins = more prominent golgi apparatus
Mucous cells have mucenogen granules
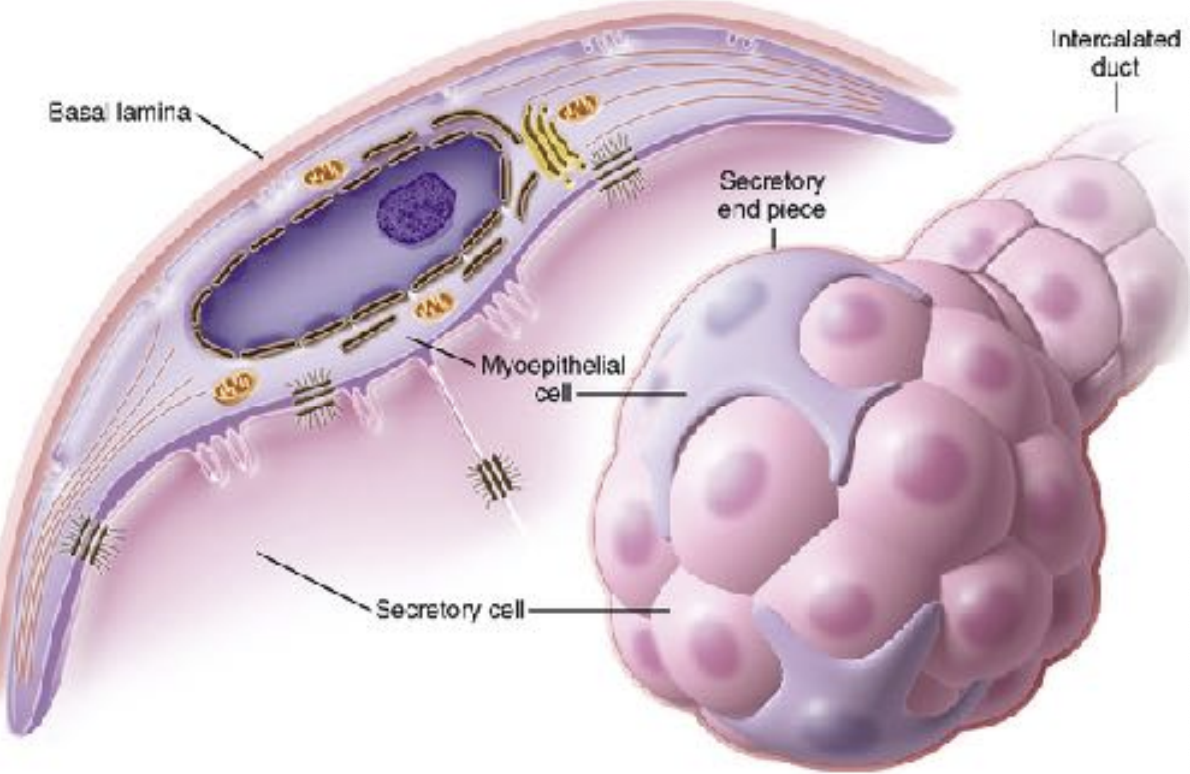
Myoepithelial cells:
These are contractile epithelial cells
forcibly express the content of the glands
Provide signals to the acinar secretory cells
Have 4-8 processes filled with actin & myosin
Support secretory cells
Ducts of the salivary gland:
Striated ducts:
Columnar cells
Centrally located nucleus
Eosinophilic cytoplasm
Prominenty striations
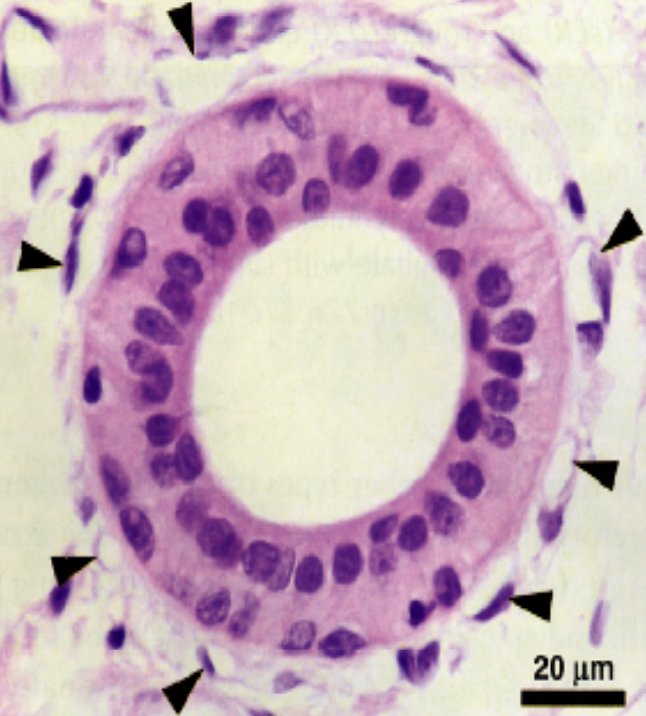
Intercalated Ducts:
Smaller in diameter
lined by small cuboidal cells
Nucleus located ar the center
Myoepithelial cells are also present
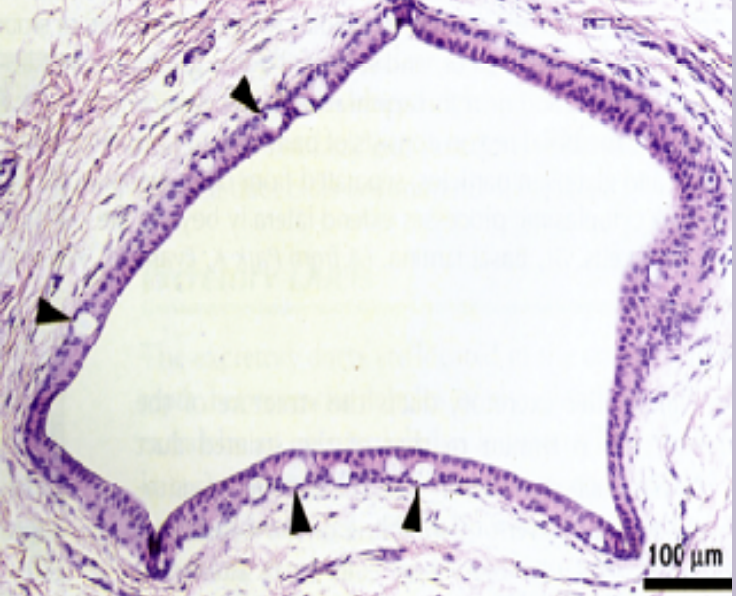
Excretory ducts:
Located in the connective tissue septa between lobules of the gland
Ducts are larger than striated ducts
In large excretory ducts goblet cells may be present between basal cells
As the duct reaches the oral mucosa the lining becomes stratified
Connective tissue:
Outer layer of connective tissue is Capsule , which serves to protect the underlying structures and provide support to the gland.
Septa are extentions of the capsule that extend inward, dividing the gland into smaller sections knows as lobes and lobules. this organization helps to compartmentalise the gland, providing a structured layout
Functionality: The septa carry essential components such as blood vessels, excretory ducts, and nerves, which are vital for the proper functioning of the gland. They ensure that the gland receives nutrients, can secrete saliva, and is able to communicate with the nervous system.

The connective tissue composed of:
Cells- fibroblasts, dendritic cells, mast cells, macrophages, plasma cells, lymphocytes and adipose tissue
Matrix- proteoglycans, glycoproteins, collagen fibers and elastic fibers
Plasma cells are located adjacent to secretory end pieces and intralobular ducts producing immunoglobulins that are secreted in saliva (secretory IgA), (sIgA)
Age changes in salivary glands include :
fibrosis and fatty degenerative changes
presence of oncocytes (eosinophilic cells containing many mitochondria)
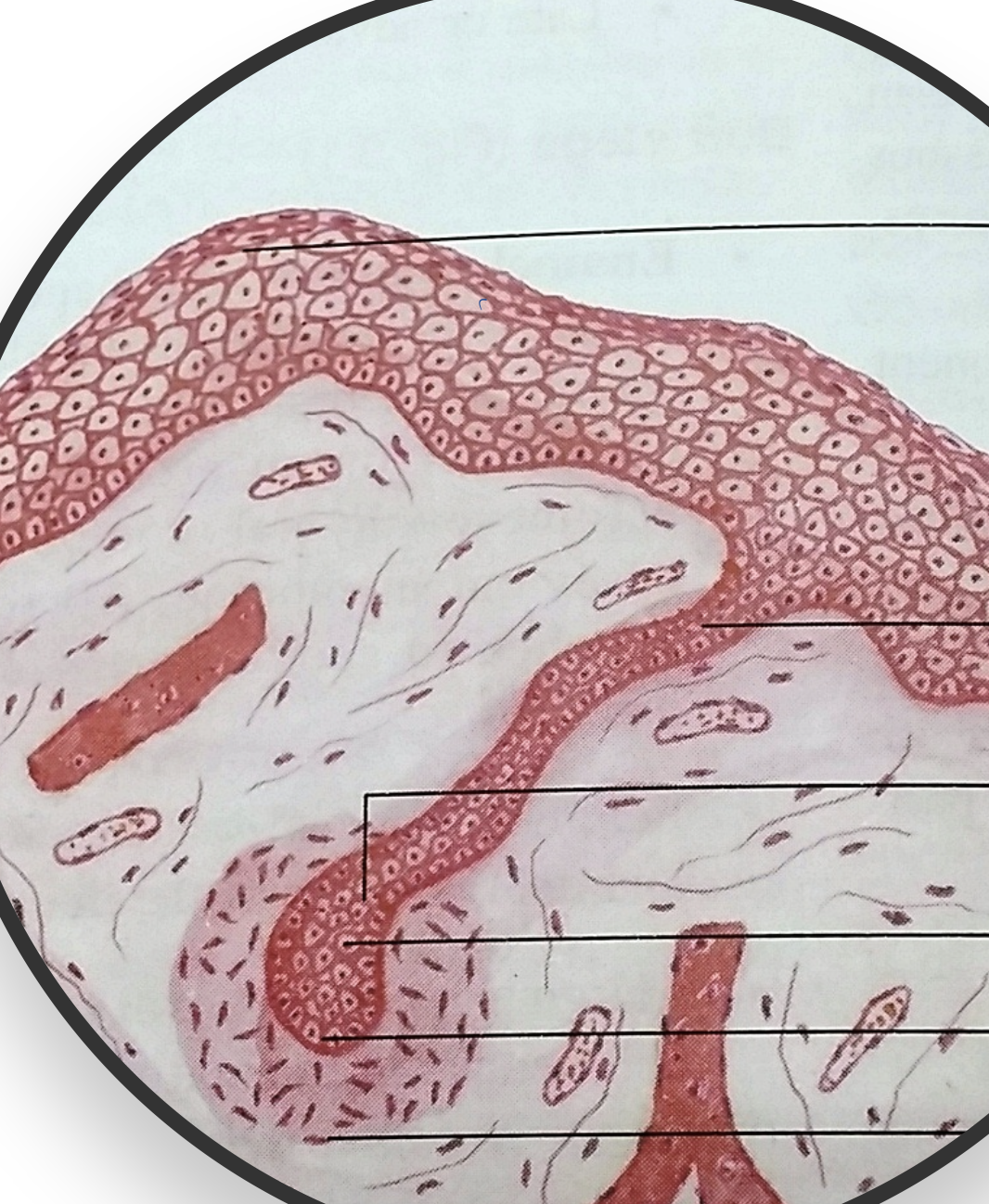
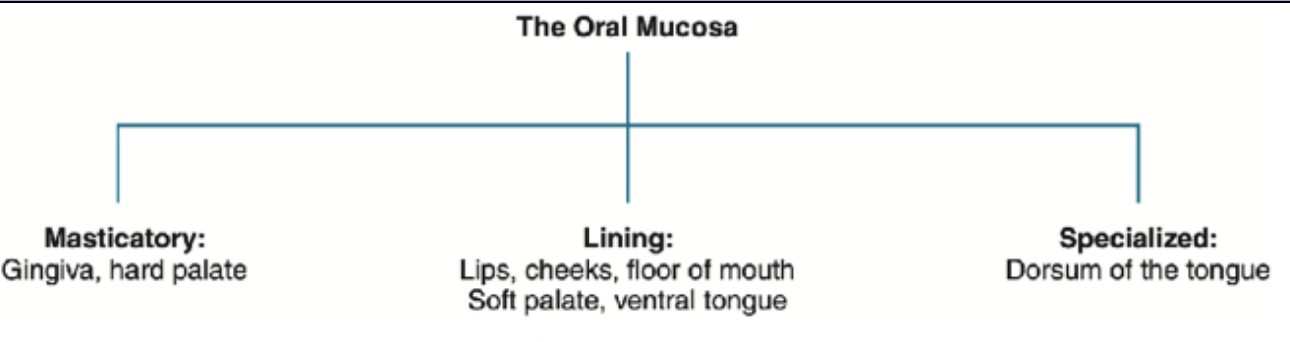
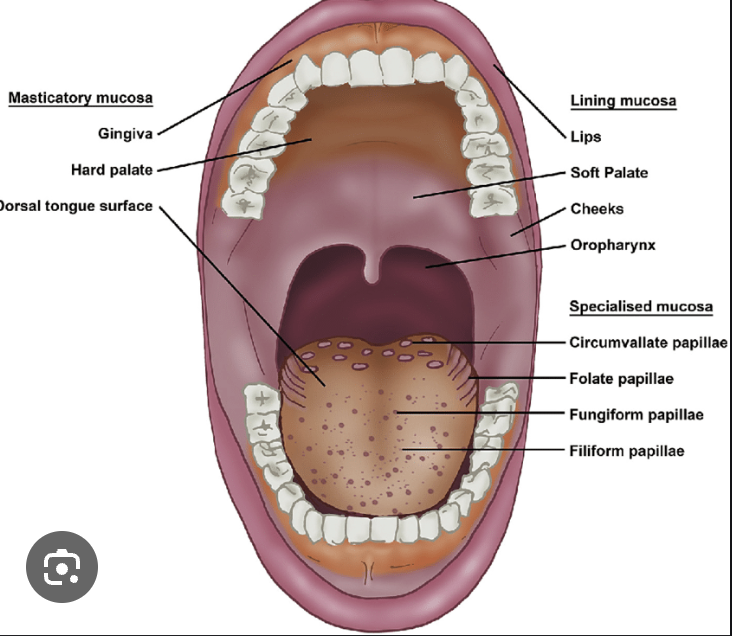
Oral mucosa
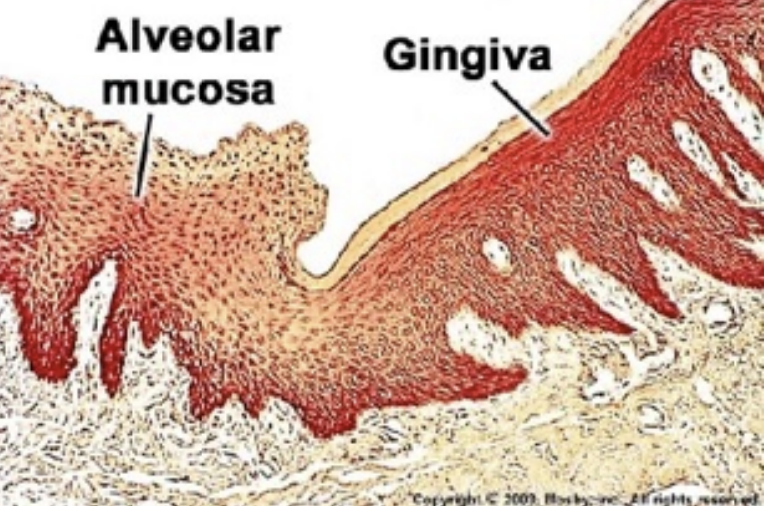
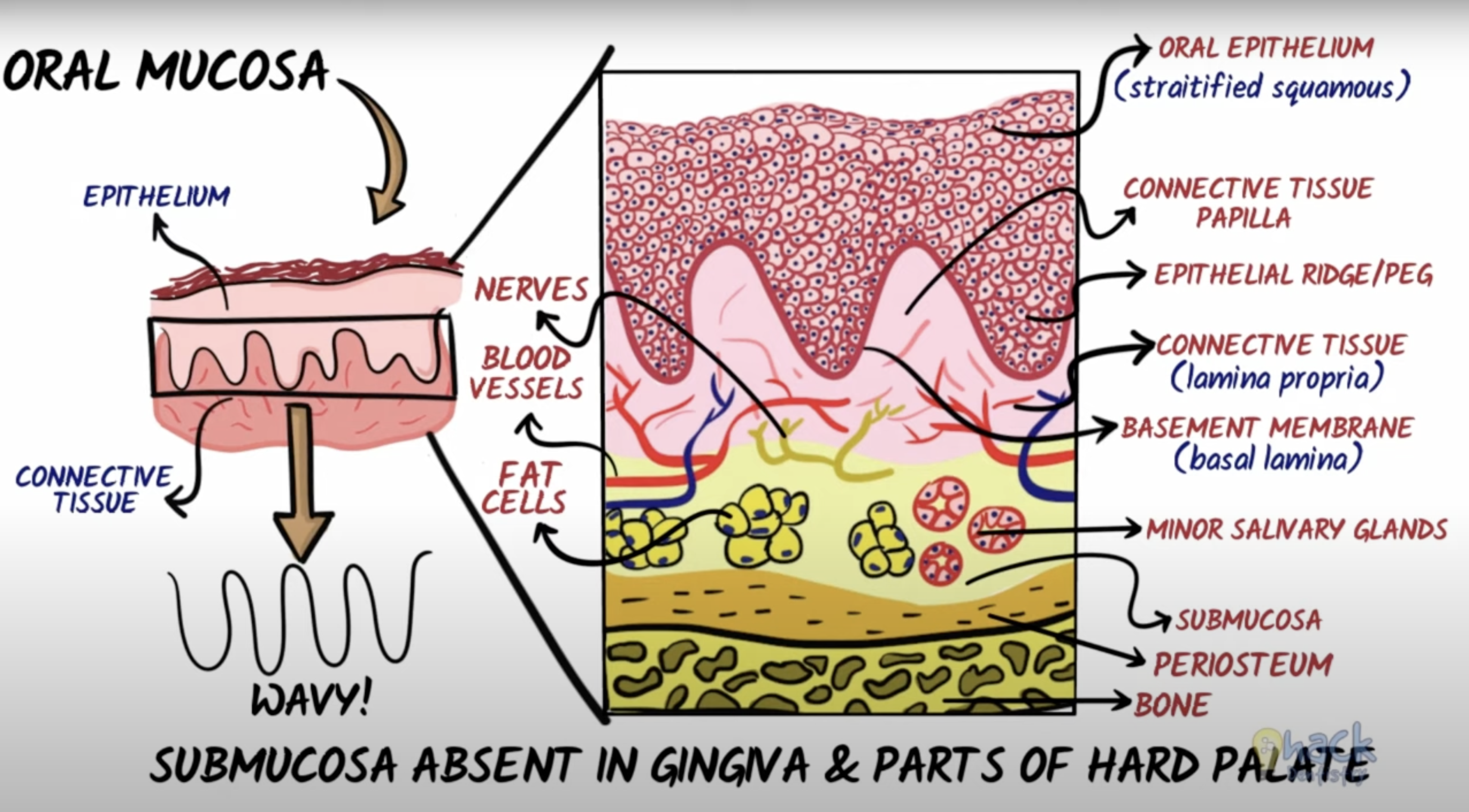
The oral mucosa is used to describe the moist lining of the oral cavity, it is made of an epithelium and connective tissue. It can be classified into: lining mucosa, masticatory mucosa, and specialized mucosa, with distinctive histological, clinical, and functional features.
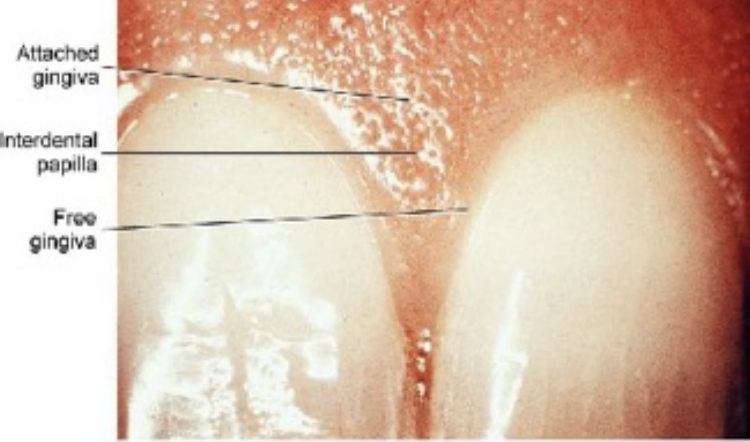
The gingiva and hard palate are a part of masticatory mucosa, masticatory mucosa also bears the forces of mastication and is usually keratinized and 25% of the total mucosa
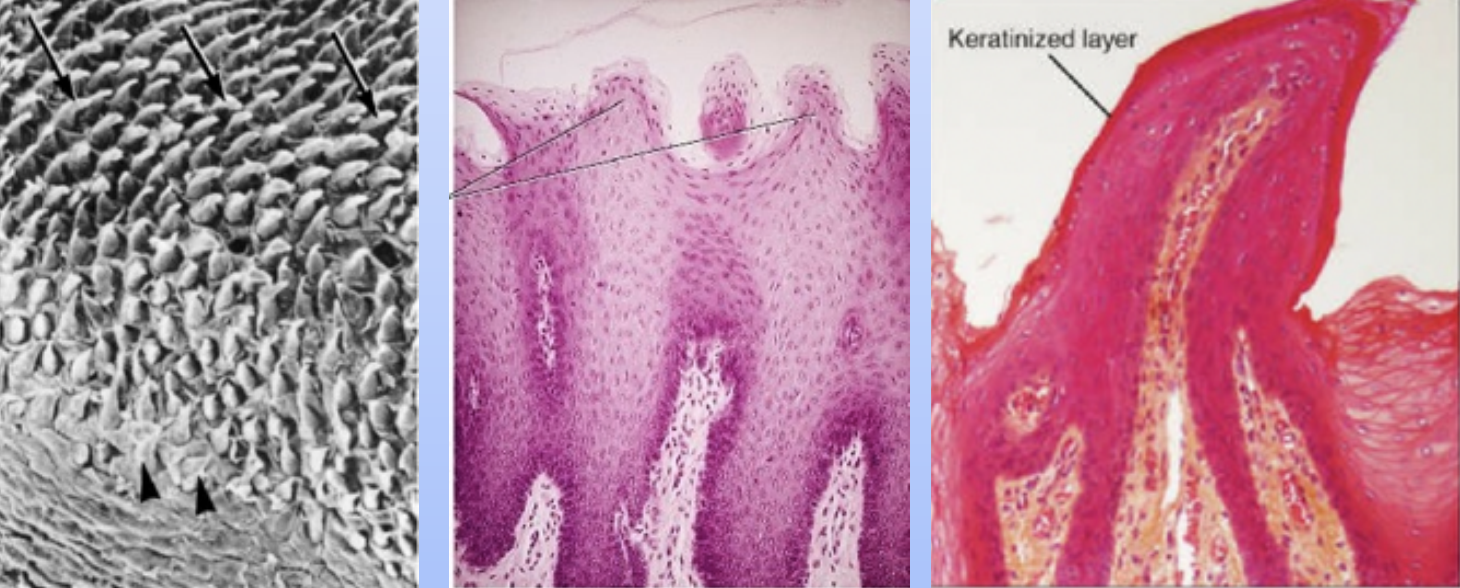
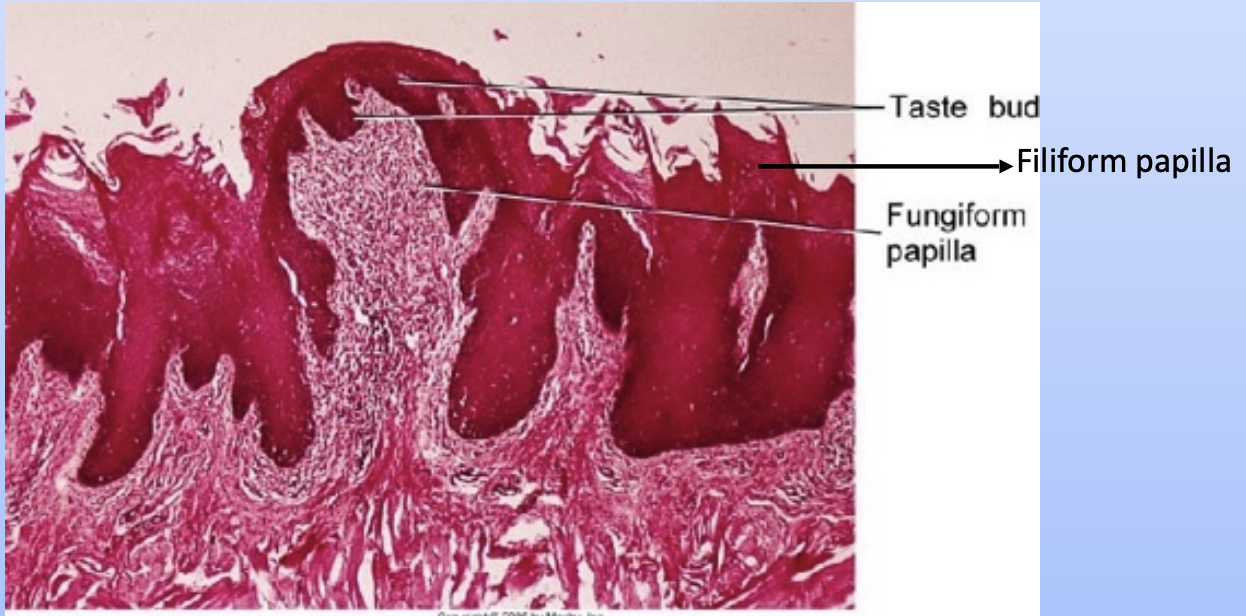
The dorsum of the tongue forms the specialized mucosa because of the presence of taste buds which have a sensory function which is 15% of the total mucosa and is composed of cornified epithelial papillae.
The rest of the oral cavity is lined by the lining mucosa which is 60 % of the total mucosa and it covers the floor of the mouth, ventral tongue, alveolar mucosa, buccal mucosa, lips, and soft palate, it is non - keratinized
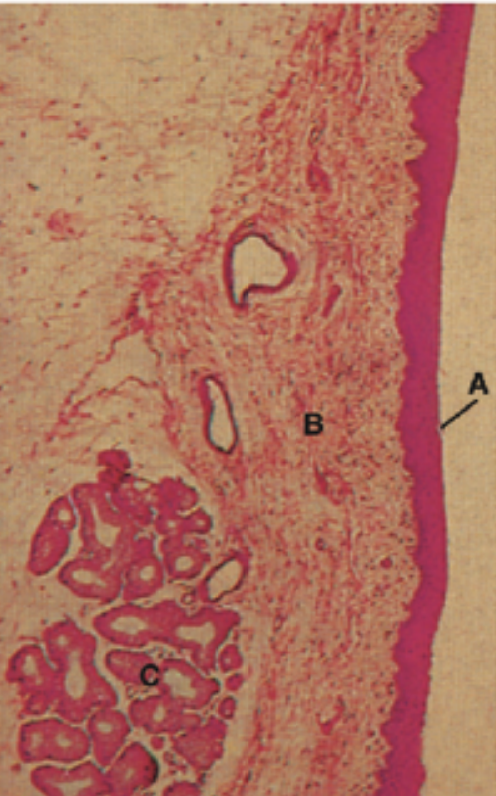
The 2 main components of the oral mucosa is the stratified squamous epithelium and the underlying connective tissue (lamina propria)
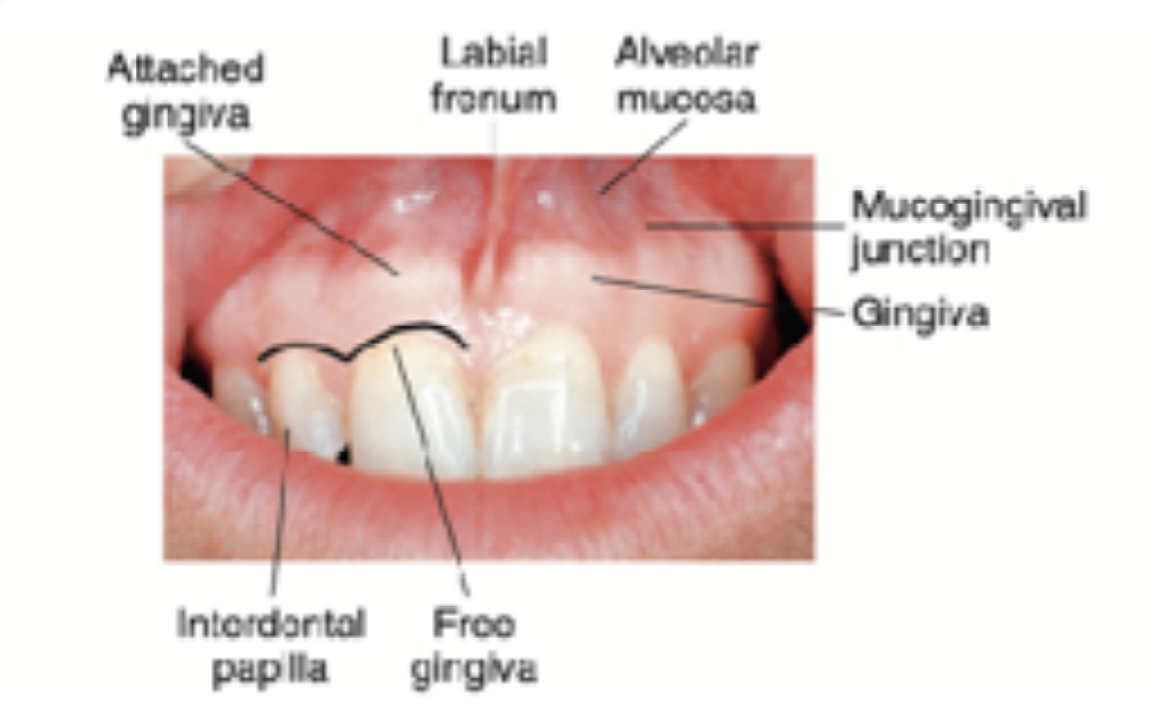
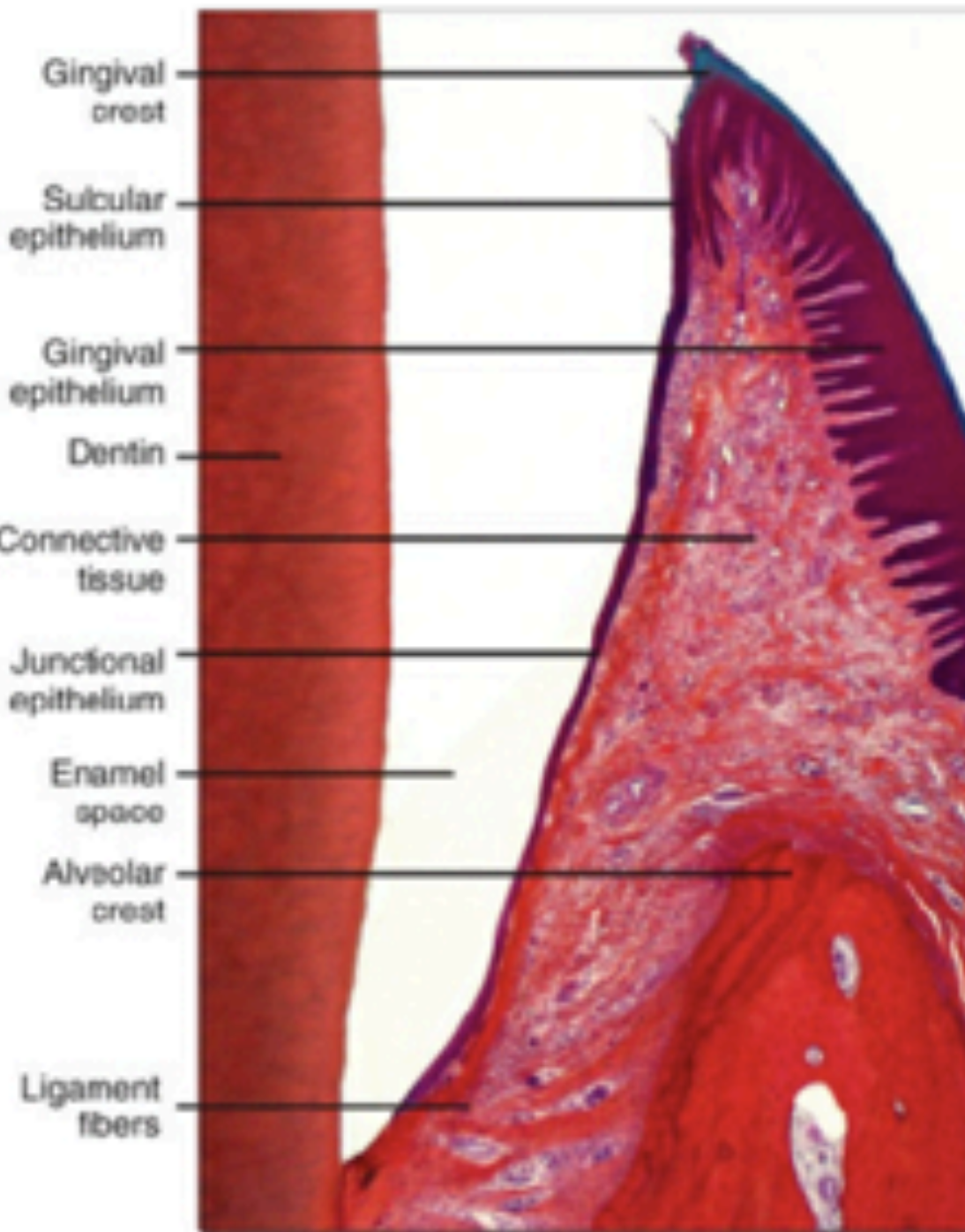
Dentogingival junction is the region where the oral mucosa meets the surface of the tooth. Very important because it is a weak area in the oral mucosa.
There are 4 types of papilla in the specialized mucosa that is located on the dorsal surface of the tongue: fungiform, filiform, foliate, and circumvallate papillae, each serving specific functions in taste perception and texture sensation.
The 4 taste sensations are sweet, salty, sour, and bitter.
Sweet and salty: Anterior tongue
Sour: Lateral tongue
Bitter: region of circumvallate papilla
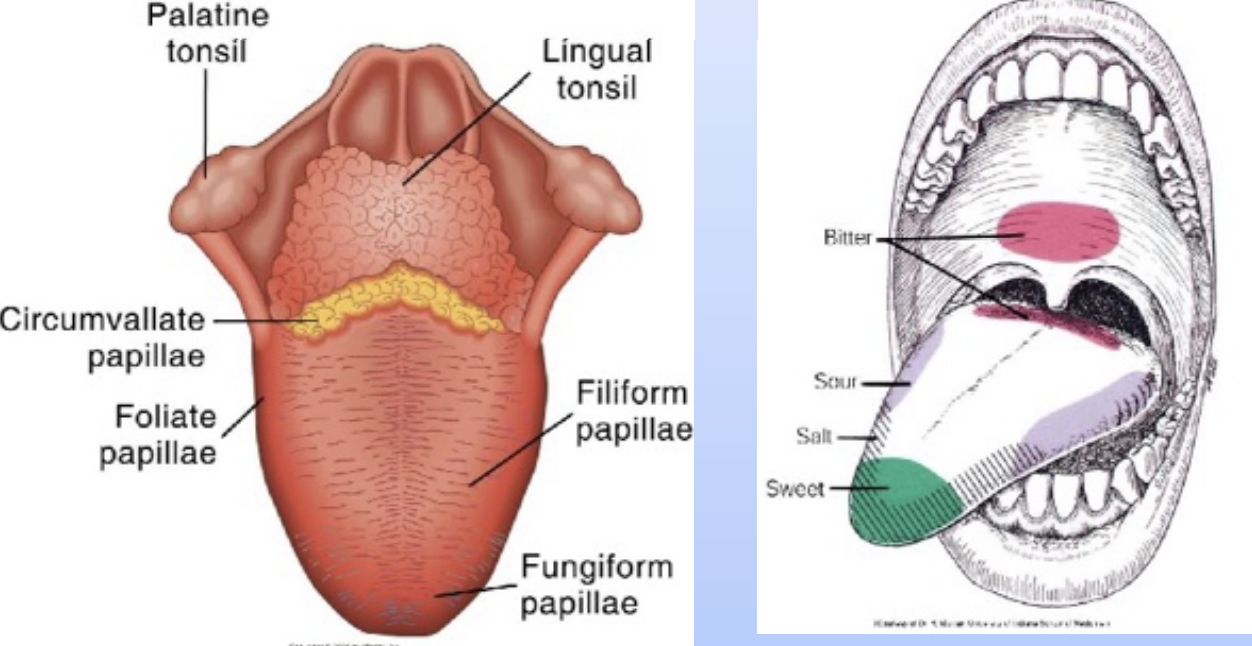
Filiform papilla: Makes up the majority of the papillae and covers the anterior part of the tongue. They appear as slender, threadlike keratinized projections on the surface epithelial cells. They facillitate mastication and movement of food on the surface of the tongue and have no taste buds.
Fungiform papilla: (Fungus-like) These are interspersed between the filiform papilla. they are smooth, round structures that appear red. Seen through a thin, non-keratinized stratified squamous epithelium. Taste buds are usually seen within the epithelium.
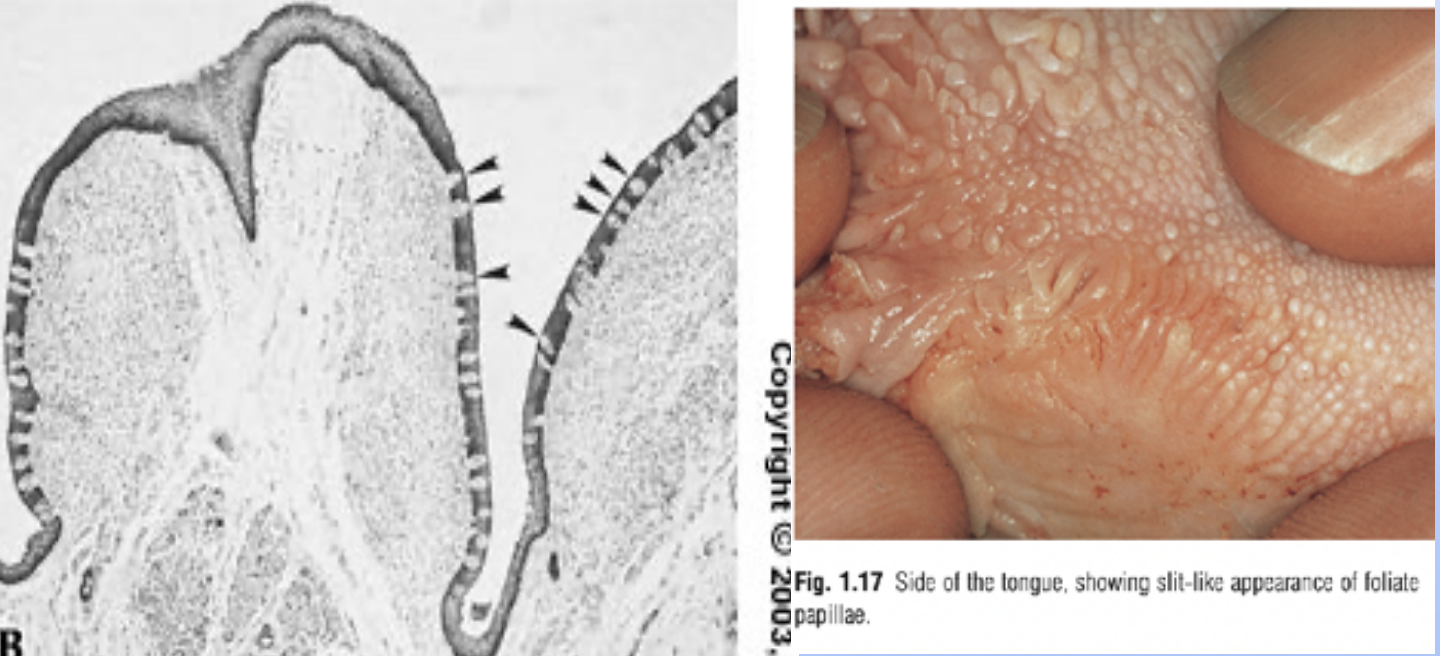
Foliate papilla: (leaf like) These are located on the sides of the tongue and are characterized by folds of tissue that contain a few taste buds in the epithelium. Foliate papillae are more prominent in infants and become less pronounced with age, serving primarily for taste sensation.
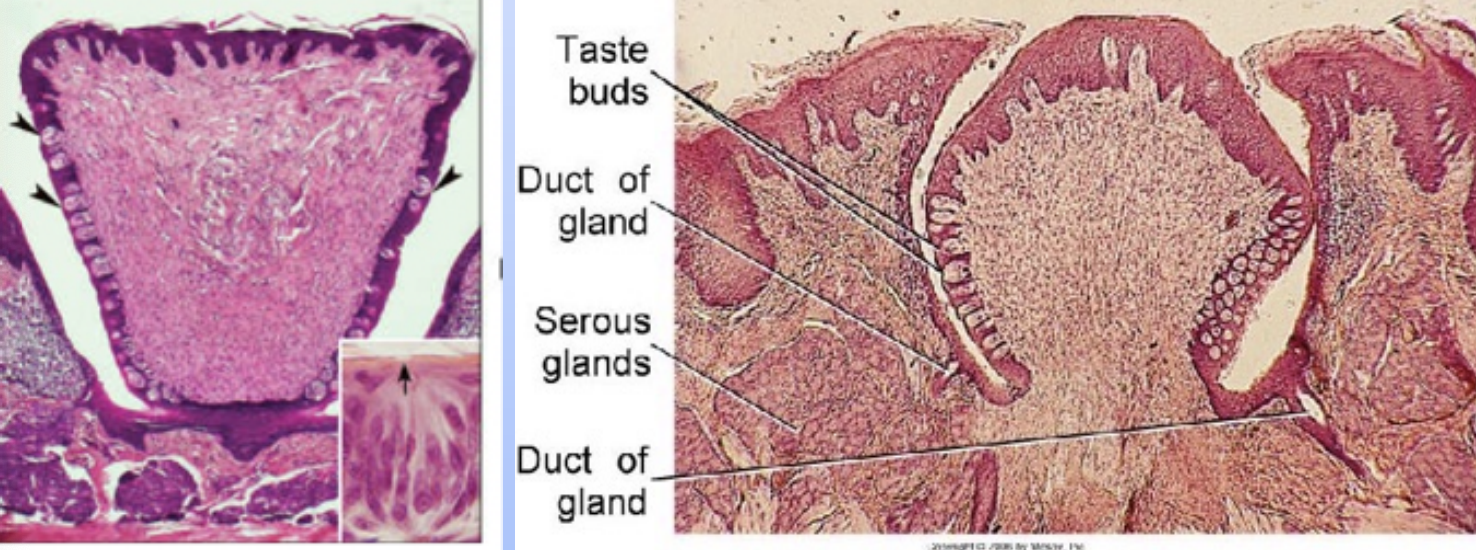
Circumvallate papilla; (walled papilla) These are large, dome-shaped structures located at the back of the tongue, surrounded by a trench. They contain numerous taste buds within their walls and are involved in the perception of bitter tastes. Circumvallate papillae are also associated with von Ebner's glands, which secrete saliva to help dissolve food substances and facilitate taste.
Orofacial development:
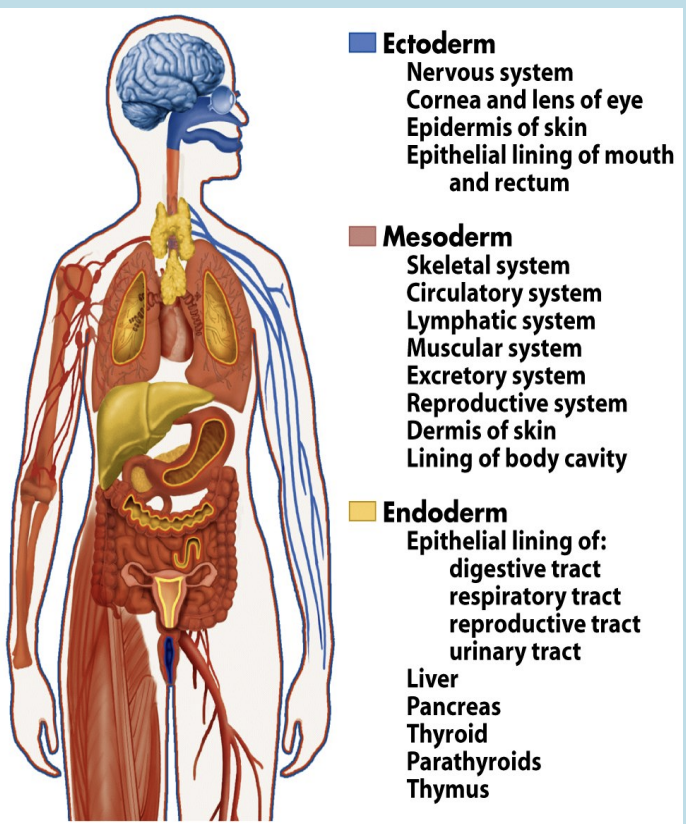
first thing that happens during the Orofacial development is the embryo develops into three types of tissues, called the germ layers:
1- Ectoderm: forms the outer covering and the nervous system
2- Mesoderm: gives rise to muscle, internal organs, and connective tissues such as blood and cartilage.
3- Endoderm: produces the lining of the digestive tract or gut, along with some of the associated organs.
Embryonic period: first 8 weeks after conceptionduring which all major organs and structures are formed, laying the groundwork for the subsequent stages of development.
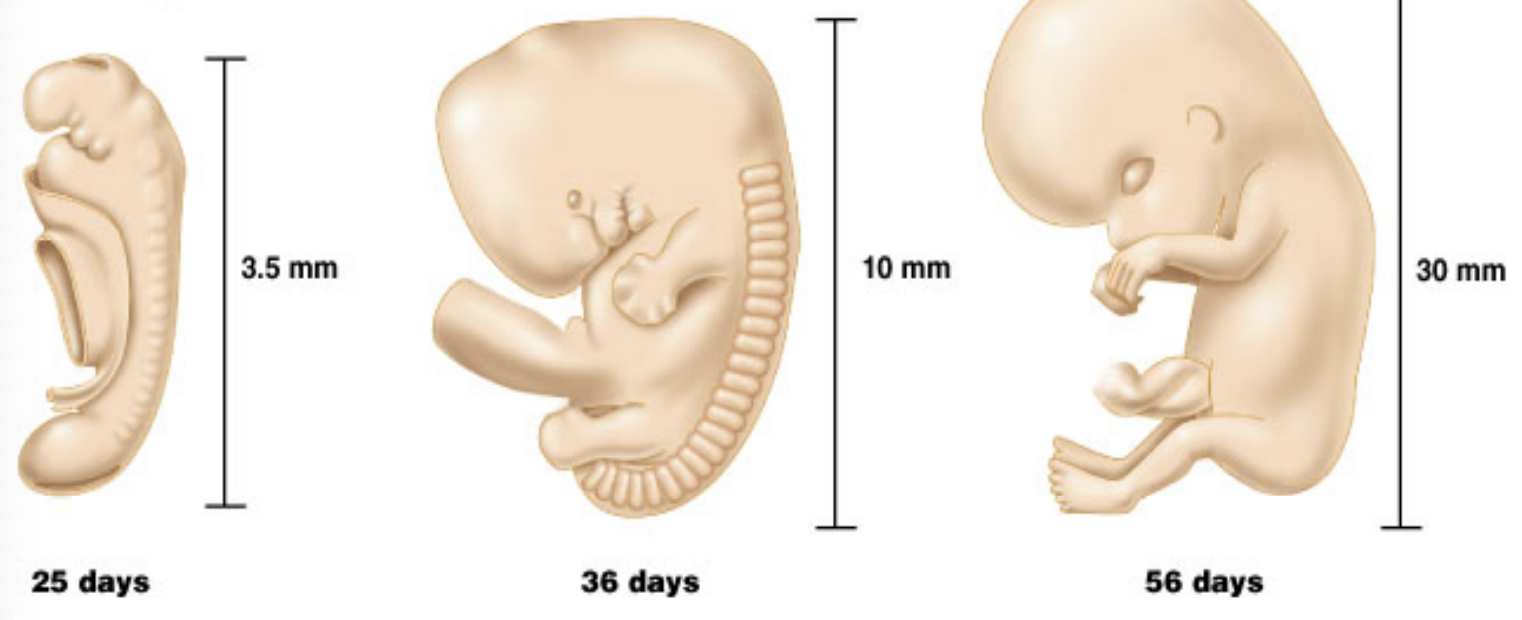
29 day embryo or about 4 weeks or 1 month: Heart starts pumping, size is ½ cm
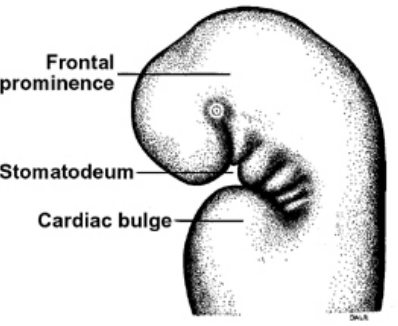
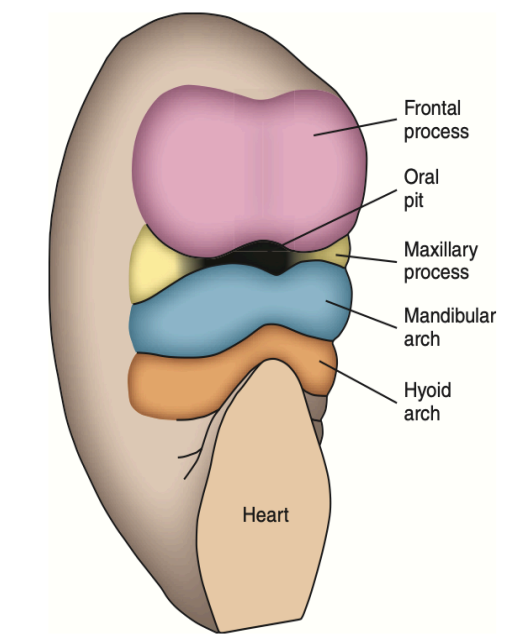
Development of primitive oral cavity and head fold: the head folding results in the formation of the primitive oral cavity = stomatodeum.
Initially, the stomatodeum is separated from the developing gut by the buccopharyngeal membrane. In the fifth week of development, this membrane ruptures, connecting the oral cavity to the foregut and forming the oropharynx. This connection is essential for the subsequent development of the digestive and respiratory systems.
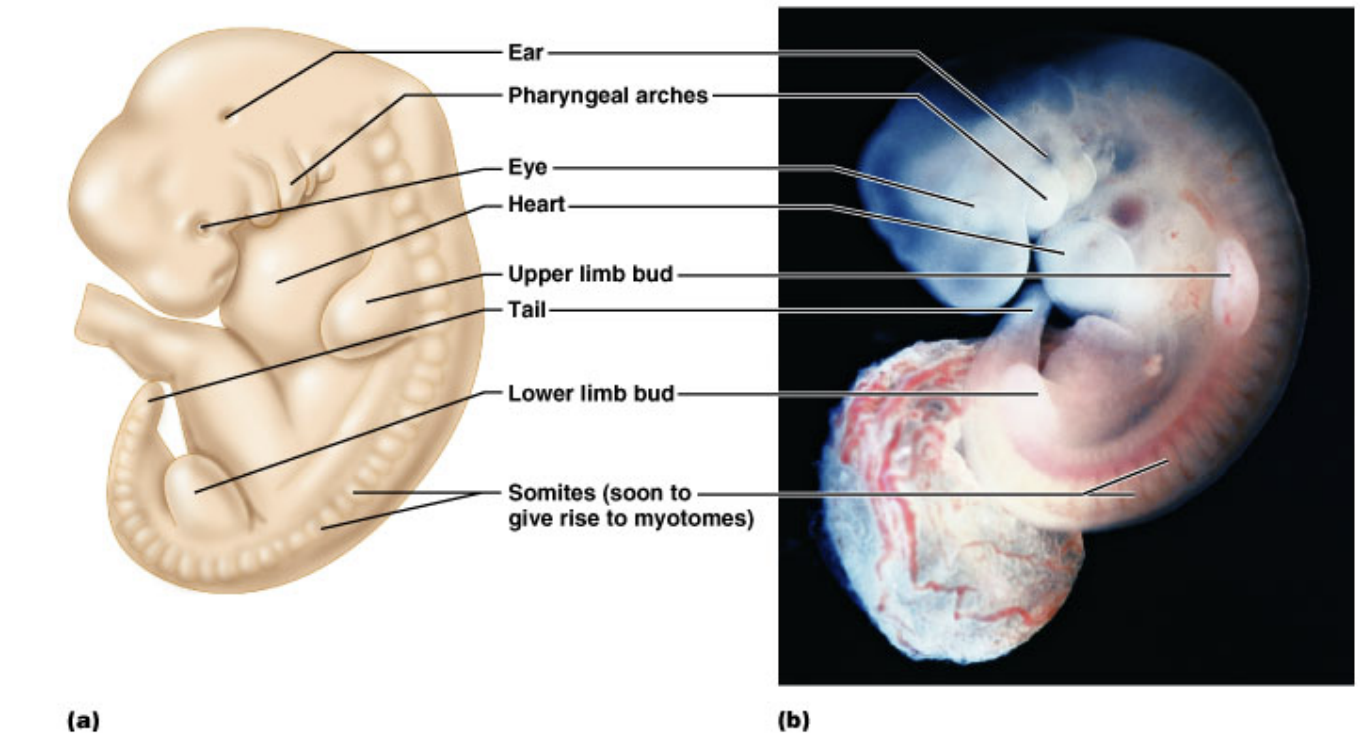
Branchial arches/ pharyngeal arches/ branchial apparatus
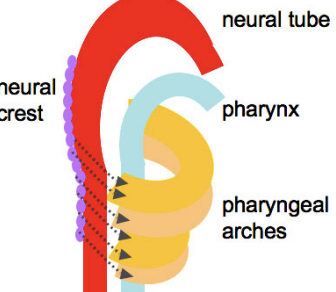
The pharyngeal arches are named like this because they bend around the sides of the pharynx as bars of tissue, each arch is separated by vertical grooves on the lateral sides of the neck at the fifth week
Medially they are seperated by pharyngeal pouches.
They are 6 pairs - U Shaped
Core of the mesenchymal tissue is formed from neural crest cells that migrate in to form the arches
They are covered externally by ectoderm and lined internally by endoderm
Each have their own developing cartilage, nerve, vascular and muscular components
These arches separate the stomatodeum from the developing heart.
The first arch (mandibular arch) - forms the mandibular and maxillary processes, associated muscles of mastication, nerves, and blood supply.
The second arch (hyoid arch) - forms the hyoid bone, and part of the temporal bone (VII)
Cartilage = Reichert’s cartilage- form the muscles of facial expression, the middle ear muscles
Third arch - forms the tongue (ix nerve)
Fourth arch - forms the tongue, most of the laryngeal cartilages (IX and X nerves)
Fifth arch - Incorporates into the fourth
Sixth arch - Forms most of the laryngeal cartilages (IX and X nerves)
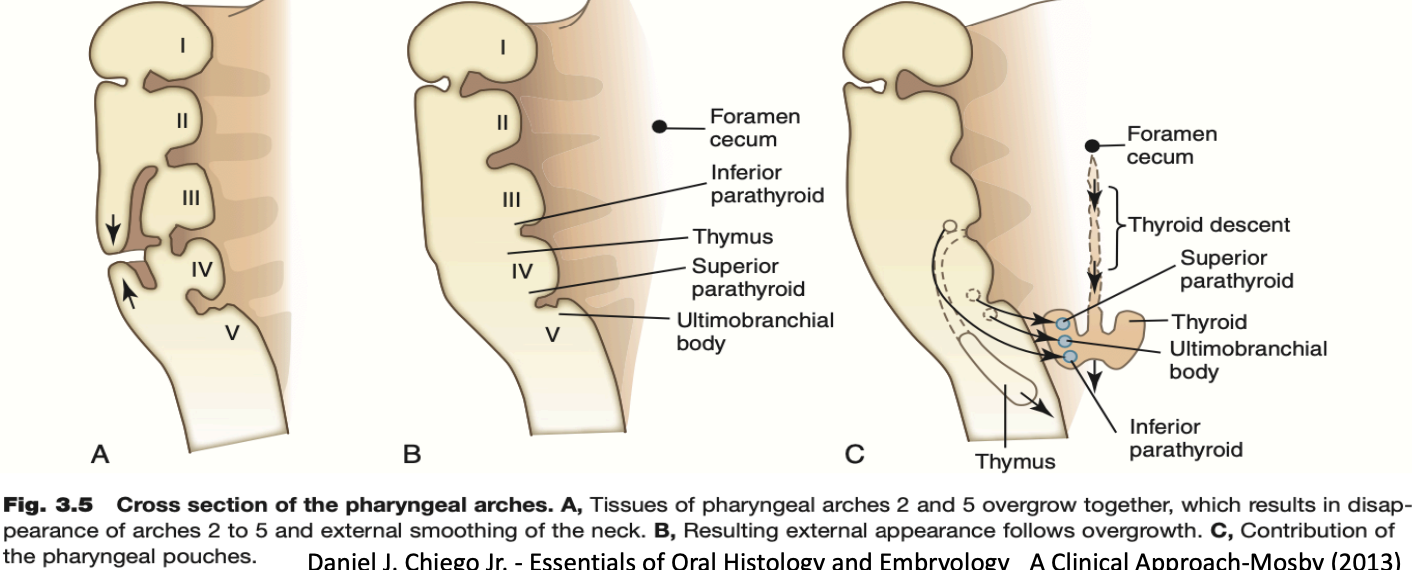
Pharyngeal pouches:
They are four well-defined pairs of pharyngeal pouches that develop from the lateral walls of the pharynx.
The first pouch (between the 1st and 2nd arches) gives rise to the external acoustic meatus, tympanic membrane, and eustachian tube
The second pouch forms the palatine tonsils.
The third pouch forms the thyroid and parathyroid glands
The fourth pouch forms the parathyroid gland
The fifth pouch becomes incorporated with the fourth
Development of the face starts from the fusion of five face-primordia (or bulges or processes) that were formed during 4th week of IUL
• One Frontonasal prominence from frontal lobe
• Two Maxillary prominences from first branchial arch
• Two Mandibular prominences from first branchial arch
• The fusion occurs during the 5th to 8th week of IUL.
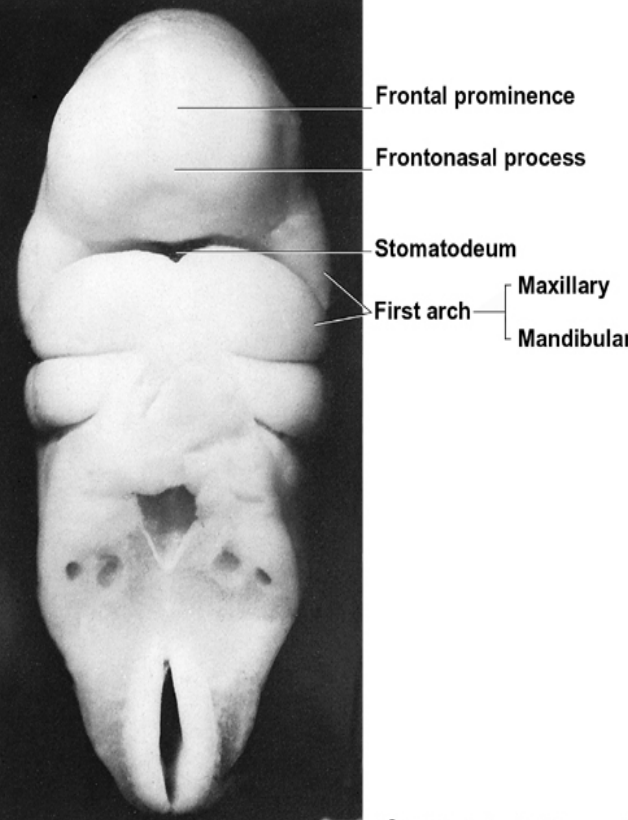
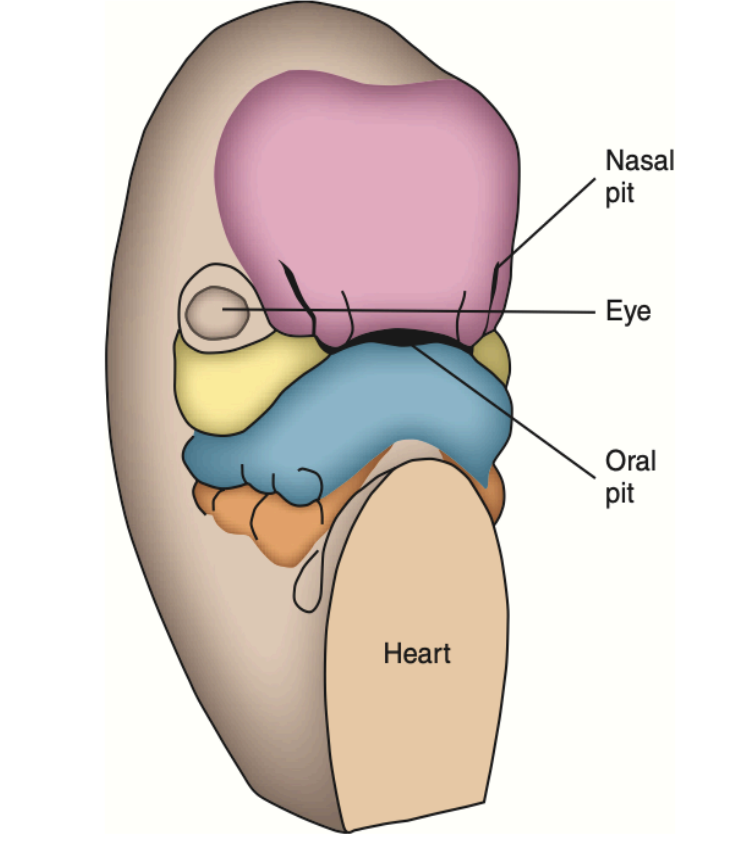
During the 4th week of IUL, the centrally located oral pits are grouped at the frontal and maxillary processes and the mandibular arch. Although it appears unrelated at this time, during this period these processes and the first arch form the human face.
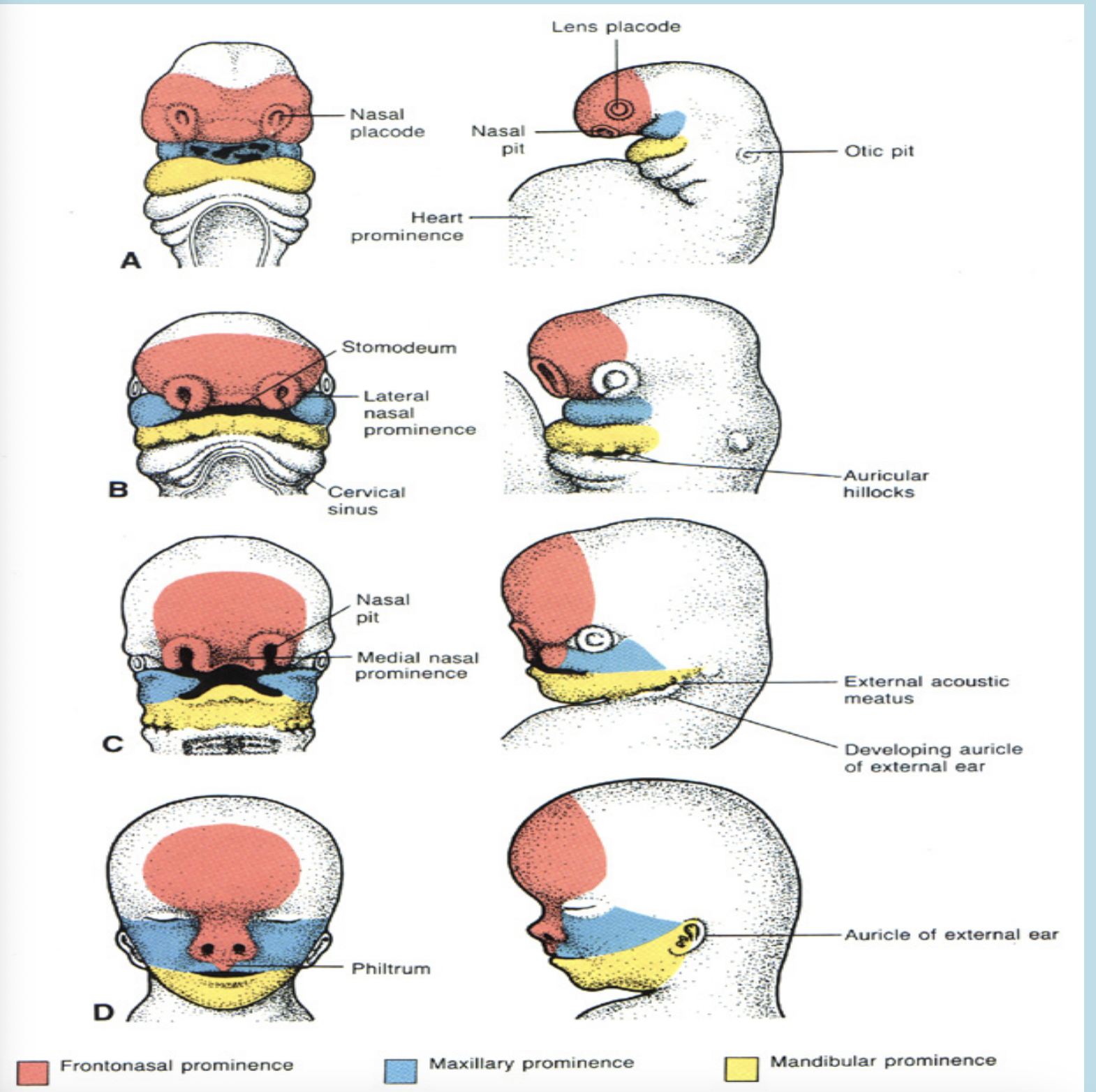
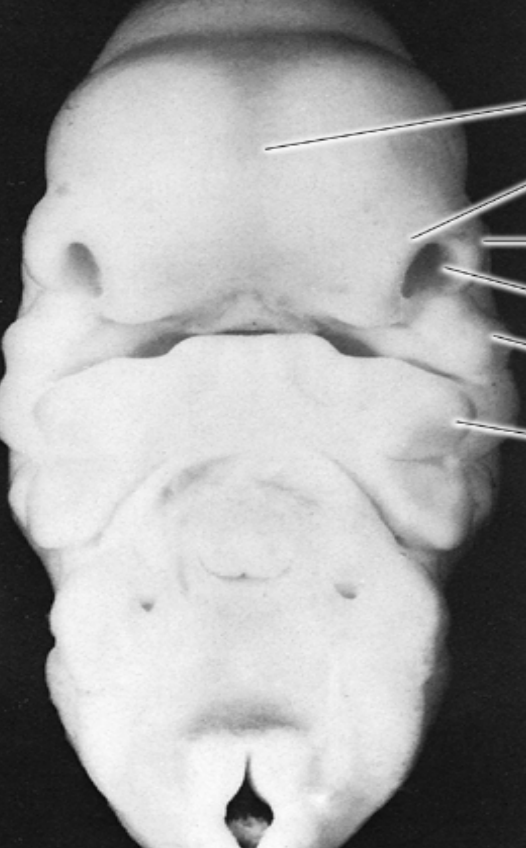
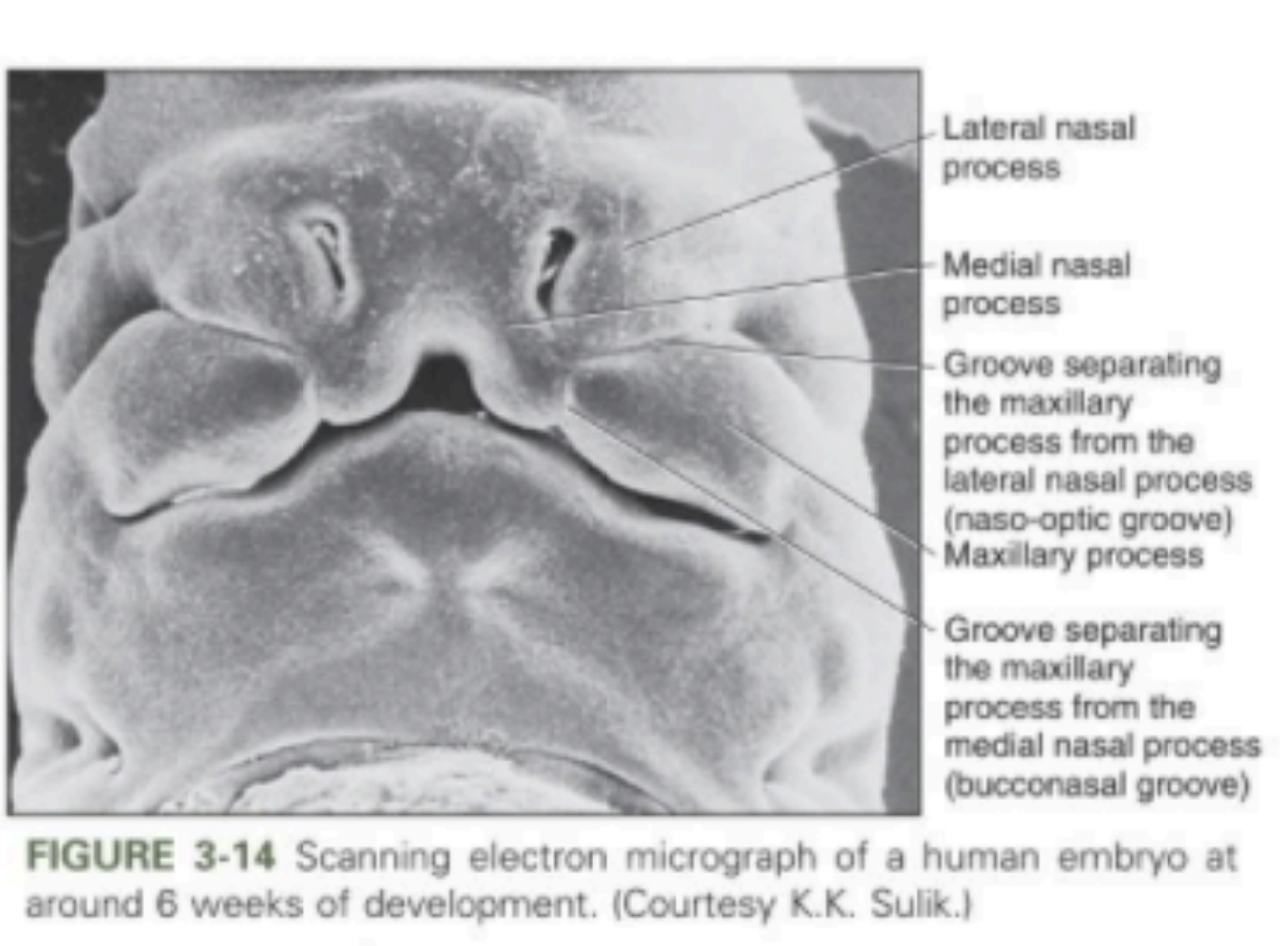
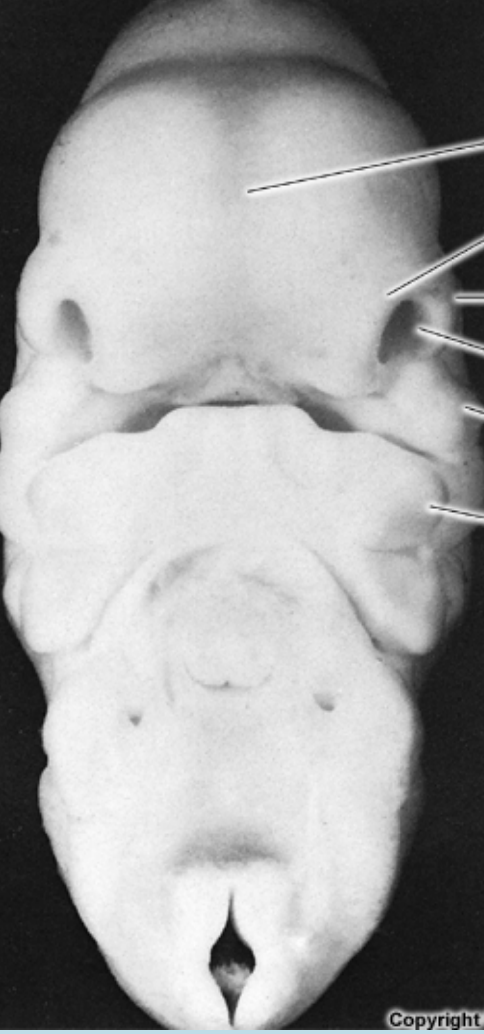
During the 5th week of IUL the nasal pits develop and now appear on the sides of the face. The frontal processes now become the frontonasal process.
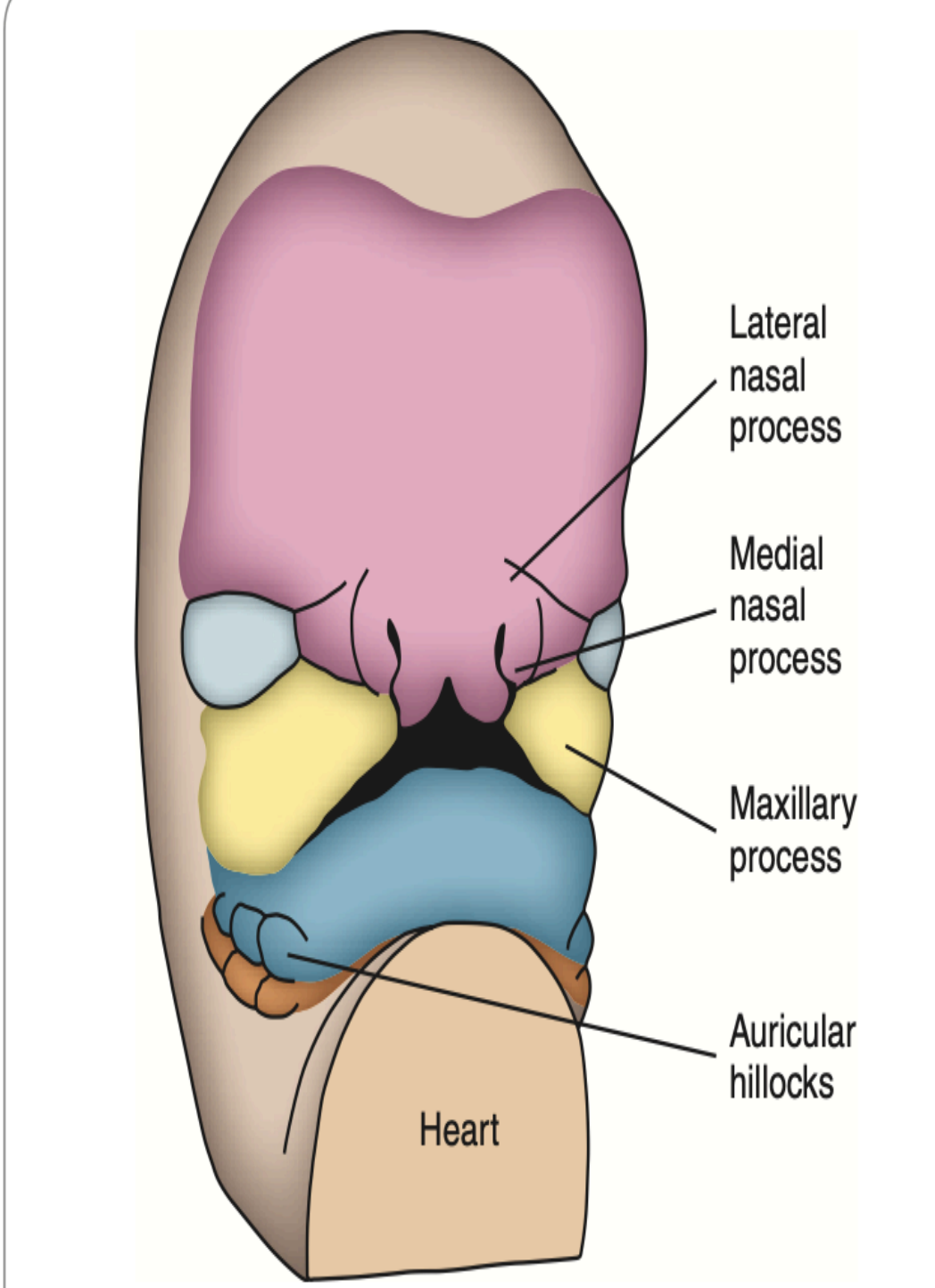
During the 6th week of IUL, the lateral parts of the face begin to expand which broadens the face. the nasal processes are limited to the middle of the upper lip, which make the face appear more human like
The upper lip is composed of a medial process and two lateral maxillary segments
The medual nasal process is called the philtrum
A ridge of tissue surrounds each nasal pit
The tissue lateral to the pits is the lateral nasal process
The tissue medial to the pits is the medial nasal process
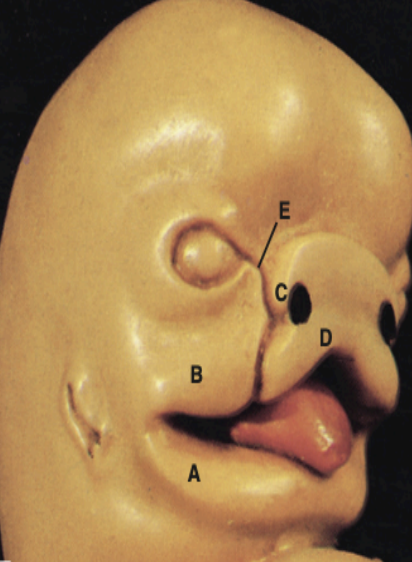
A- Mandibular process
B- Maxillary process
C- Lateral nasal process
D- Medial nasal process
E- Naso-optic furrow
The development of the upper face is from the tissues surrounding the oral pit.
Day 24: The frontal process develops (it covers the forebrain) Which result in the start of the maxillary and mandibular processes from the 1st branchial arch, and a well-defined boundaries of the stomatodeum.
Day 26: The maxillary and mandibular processes become well-formed
Day 27: The nasal placode and the odontogenic epithelium appear
Day 28: Localized thickenings develop within the frontal prominence which are the olfactory placodes.
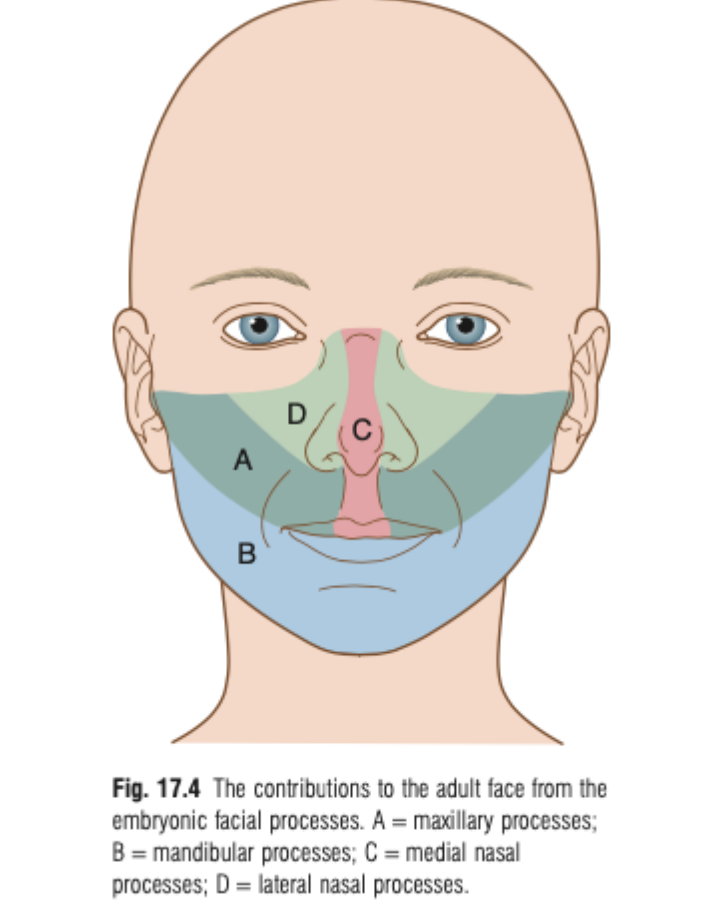
The contributions to the adult face from the embryonic facial process:
Maxillary processes: Contribute to the upper lip, cheeks, and part of the palate.
Mandibular processes: Form the lower lip and mandible.
Medial nasal processes: Forms the bridge of the nose, the tip of the nose, and the nasal septum, as well as the midline of the upper lip.
Lateral nasal process: Forms the lateral aspects of the nose and contributes to the alae of the nostrils.
Development of naso-maxillary complex:
By the 4th to 5th week of development, nasal placodes (thickened areas of epithelium) form, which become the olfactory epithelium.
Ectomesenchyme cells proliferate and migrate around these placodes, forming medial and lateral nasal processes surrounding the nasal pits.
The medial nasal processes fuse at the midline, forming the intermaxillary (premaxillary) process, which contributes to the premaxillary segment.
Development of naso-maxillary complex:
The frontal lobe proliferates between the medial nasal processes to form the frontonasal prominence, which contributes to the forehead and parts of the nose.
The medial nasal processes (from both sides) and the frontonasal prominence together form the middle portion of the nose, upper lip, anterior maxilla, and the primary palate.
The upper face develops faster than the lower face during this period.
Early facial development is driven by tissue proliferation and migration forming the primitive nasal cavities.
Around day 28, olfactory placodes (ectodermal thickenings) appear.
Rapid proliferation of underlying mesenchyme pushes the frontal eminence forward, forming the nasal pits.
The lateral arm of each pit forms the lateral nasal process.
The medial arm of each pit forms the medial nasal process.
The area between the pits becomes the frontonasal process, where the nose develops.
The medial nasal processes and the frontonasal process together give rise to:
The middle portion of the nose
The upper lip
The anterior part of the maxilla
The primary palate
Paranasal Sinuses & Nasal Cavity Development
Some paranasal sinuses begin developing in late fetal life.
Frontal and sphenoid sinuses are not present at birth.
By age 2, the anterior ethmoid sinuses grow into the frontal bone (visible on X-rays by age 7).
Posterior ethmoid sinuses grow into the sphenoid bone.
Sinuses influence facial size/shape in infancy and voice resonance.
Remaining sinuses develop after birth.
They form as outgrowths from the nasal cavity wall.
These outgrowths become air-filled extensions in adjacent bones.
The original openings remain as the adult sinus orifices.
Maxilla Development
The maxillary process arises from the first branchial arch.
Ossification centers form in the maxillary processes and extend into the palatine process to form the hard palate.
The maxillary process gives rise to the cheek, maxilla, and zygomatic bone.
It fuses with the lateral nasal process (LNP), creating the naso-optic furrow.
Fusion of facial processes at the center creates a bulge from the medial nasal process (MNP) called the premaxillary/globular process.
This forms the primary palate and four incisor teeth.
Maxillary tooth development begins as epithelial thickenings in the arch at their future positions.
Development of palate invlolves the formation of:
Primary palate
Forms from the premaxillary process (fusion of medial nasal processes)
Secondary palate
Forms from the two lateral palatine shelves or processes
Develop as internal projections of the maxillary prominences
Fusion of their processes
Fusion of the median nasal processes gives rise to the median palatine process and form the primary palate.
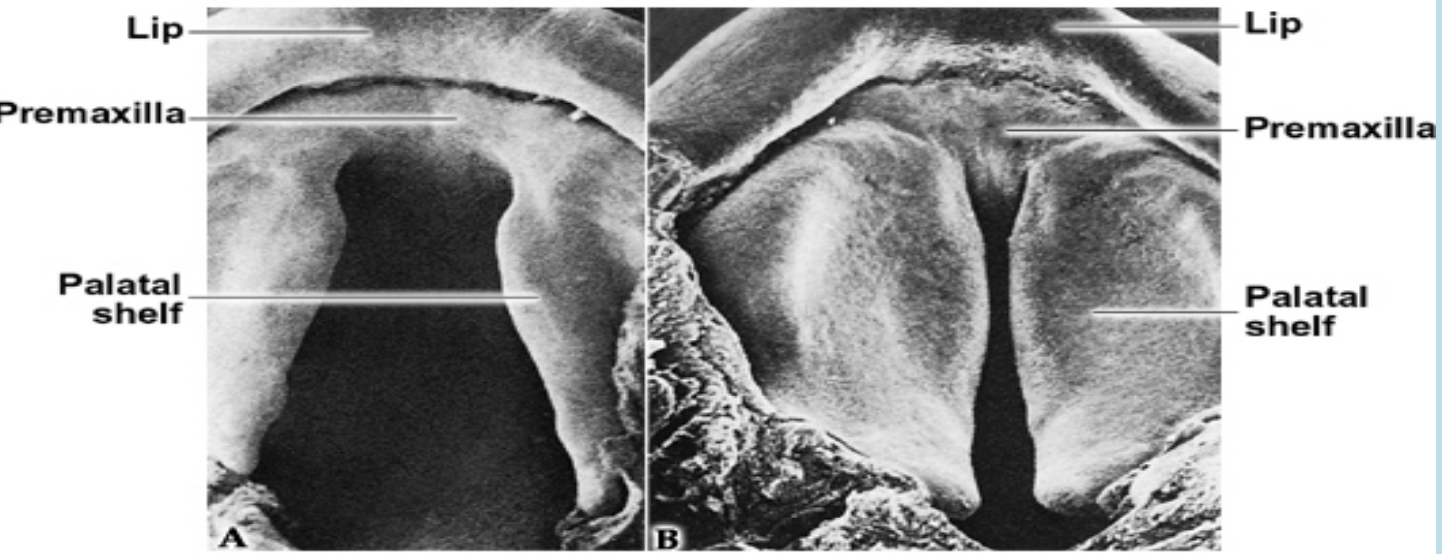
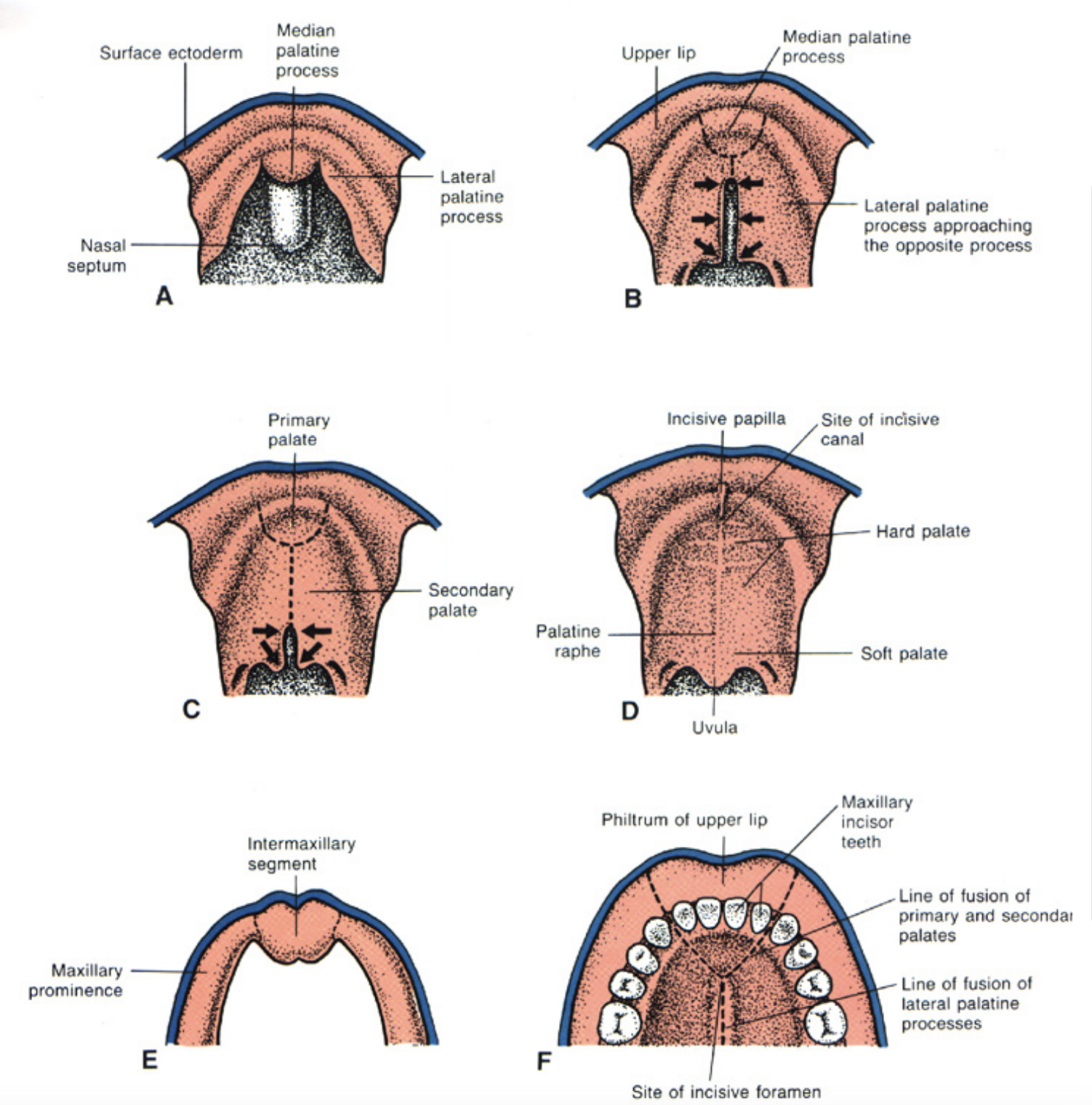
Primary and secondary palate:
The common oronasal cavity is bounded anteriorly by the primary palate and occupied by the developing tongue
Only after the development of the secondary palate, the oral and nasal caities can be distinguished.
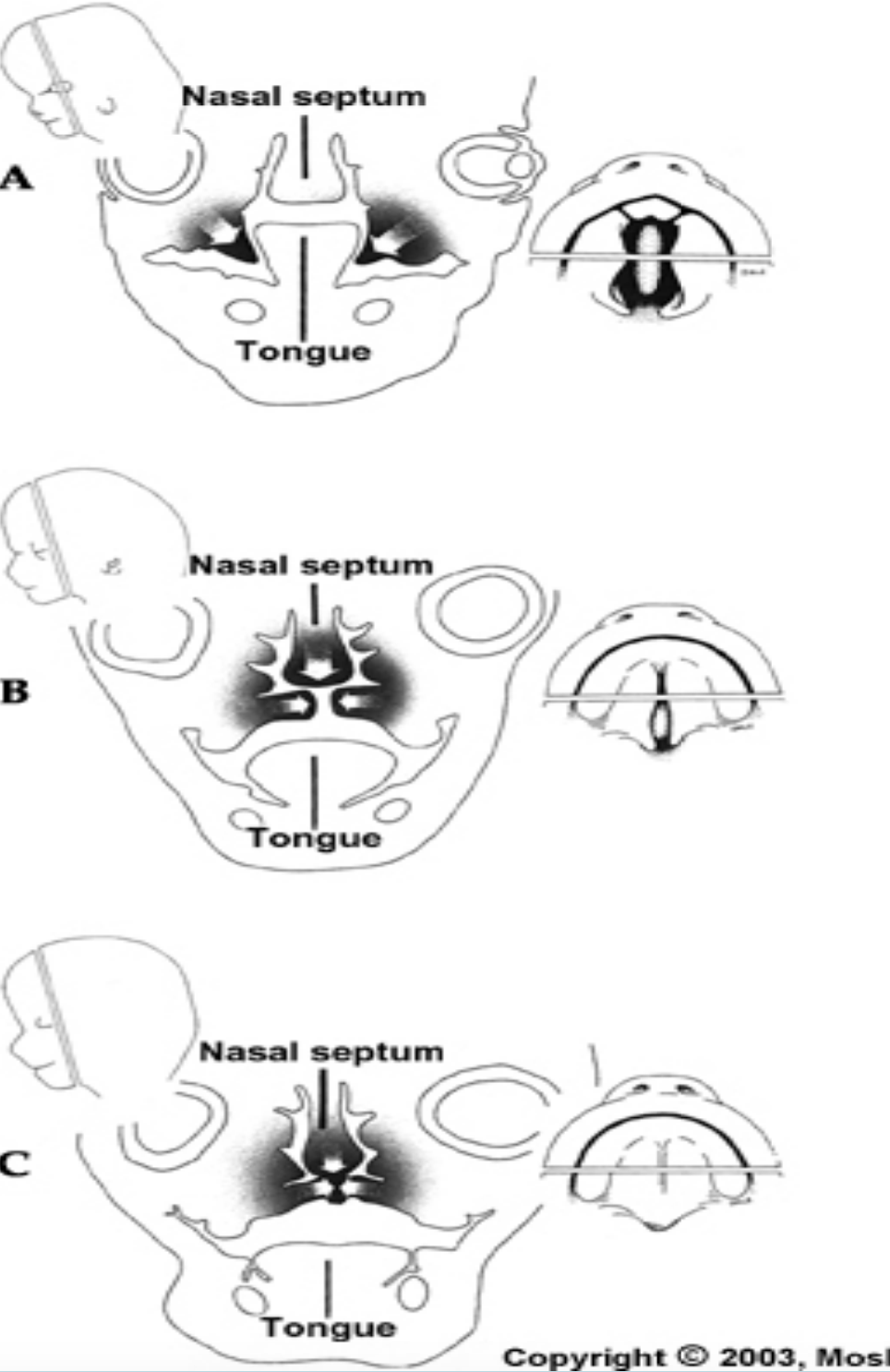
Three outgrowths appear in the oral cavity:
Nasal septum: Grows downwards through the oral cavity and it encounters the primary and secondary palates
2 palatine shelves
The closure of the secondary palate involve the hardening of the palatine shelves along with the downward movement of the tongue.
During the fourth week of development:
The maxillary processes fuse with the medial nasal processes, forming the lateral parts of the upper lip, while the medial nasal processes form the central part of the upper lip.
The maxillary processes also fuse with the lateral nasal processes, creating the nasolacrimal groove (from the inner eye corner to the nasal cavity).
The entire lower lip develops from the mandibular process.
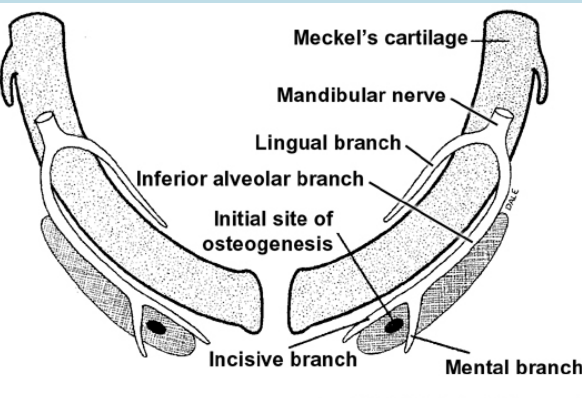
Mandible development begins with Meckel’s cartilage (from the first branchial arch) around 6 weeks, forming a rod surrounded by a fibrocellular capsule. The two cartilages are separated at the midline by the mandibular symphysis.
Mesenchymal condensation occurs near the symphysis.
At 7 weeks, intramembranous ossification begins in this mesenchyme, spreading forward and backward to form the mandible.
The mandible bones grow toward the midline but do not fuse immediately—the mandibular symphysis, derived from Meckel’s cartilage, fuses shortly after birth.
The ramus forms through rapid posterior ossification into the first arch mesenchyme.
Growth of the mandible until birth is influences by the appearance of three secondary (growth) cartilages
condylar – 12th week, developing ramus by endochondral ossification, a thick layer persists at birth at the condylar head (mechanism for post-natal growth of the ramus = endochondral)
coronoid – 4 months, disappears before birth
symphyseal – appears in the connective tissue at the ends of the Meckel’s cartilage, but disappear after 1 year after birth
Development of the tongue begins in about 4 weeks of embryonic development.
The oral part (anterior two-thirds) of the tongue develops from the fusion of two lateral lingual swellings and a median tuberculum impar.
The pharyngeal part or root of the tongue (posterior one-third) develops from the copula and the hypobranchial eminence (forms from the 2nd, 3rd and 4th branchial
arches)
Muscles of the tongue arise from occipital somites which migrate into the tongue area
The tongue develops from the endoderm of the first four bronchial arches.
During the fourth week of IUL, pairs of swellings called lingual swellings from the first arch and a single swelling called tuberculum impar originates, with ectoderm covering outside. The lingual swellings give rise to anterior 2/3 of the tongue.
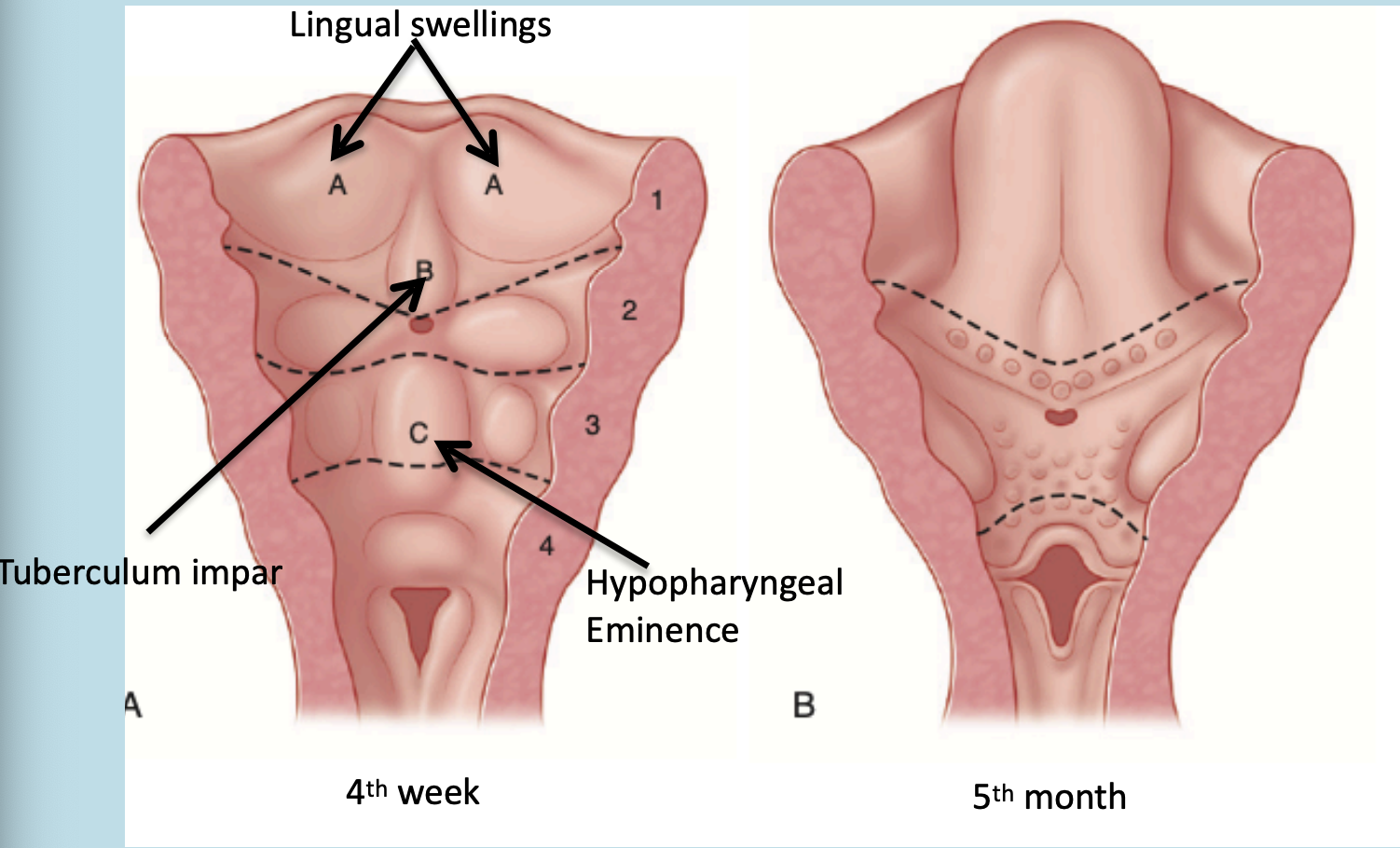
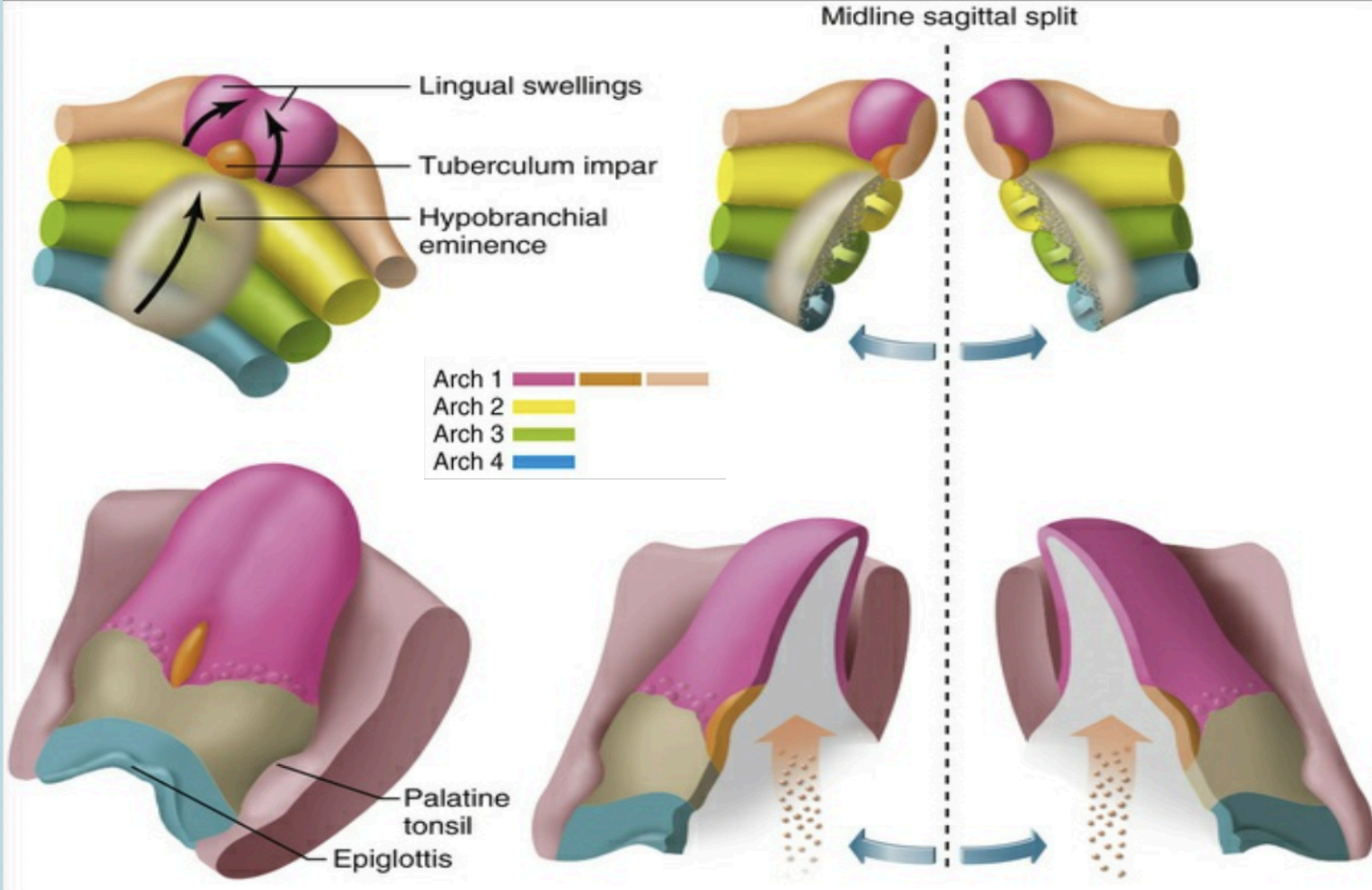
The lingual swellings, together with the tuberculum impar, which arise from the first arch, will form the anterior two thirds of the tongue. The hypobranchial eminence overgrows the second arch. Final disposition of the tongue and the relative contributions of the first to fourth arch. The arrow depicts the route of incoming occipital myotomes that form the tongue muscle.
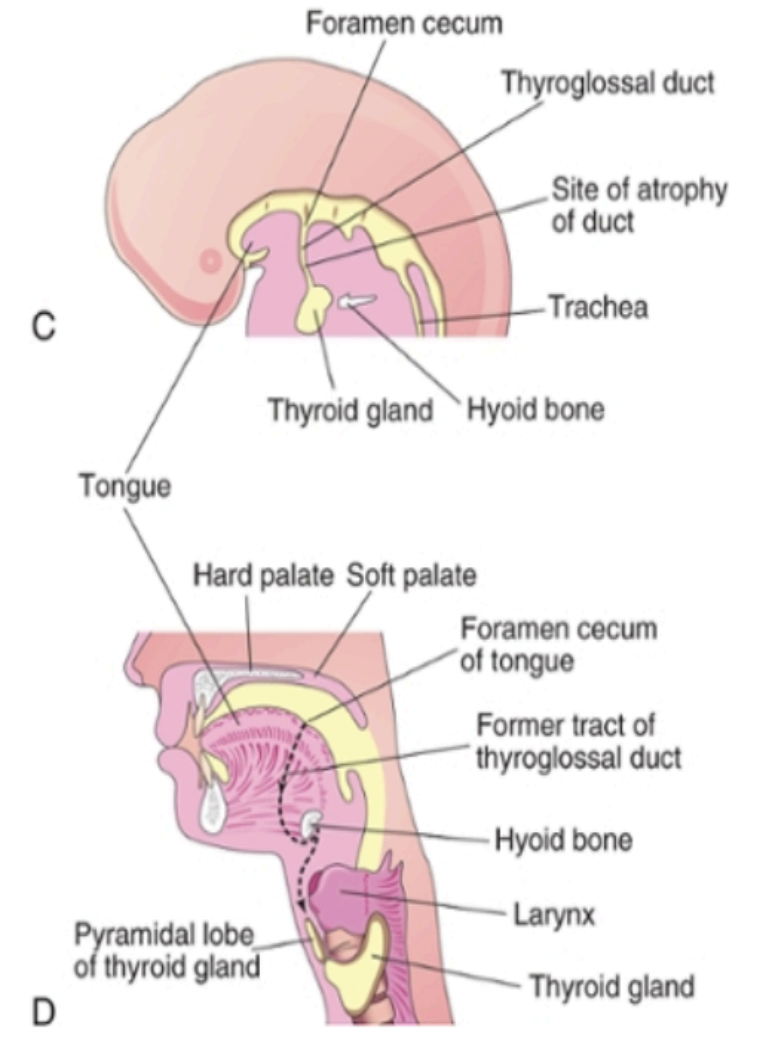
Development of the thyroid: The thyroid gland is the first of the body’s endocrine glands to develop, on approximately the 24th day of gestation from the primative oral cavity.
The thyroid originates from two structures: The primative phaarynx and neural crest
It begins at the foramen cecum, located between the tuberculum impar and copula (tongue-forming structures).
A thyroid diverticulum (tube-like outgrowth) forms from the foramen cecum and elongates downward as the thyroglossal duct, passing in front of the hyoid and thyroid cartilage.
By the 5th week, the duct bifurcates to form the two lateral lobes of the thyroid and the isthmus.
During migration, the thyroid remains temporarily connected to the tongue by the thyroglossal duct.
Neural crest cells are the band of cells at the outer most edges on neural plate. They present on the dorsal aspect of the neural tube. They migrate from the ectoderm to mesoderm to form the connective tissue called the ectomesenchymal cells.
They give rise to:
Connective tissue of the craniofacial structures including bone, cartilage, ligament
Connective tissue of lacrimal and salivary glands
Dental structures (enamel is from the surface ectoderm but the signal for the stimulation is from the ectomesenchyme )
Connective tissue of thyroid, parathyroid and thymus
Tunica media of the outflow tract of the heart and the great vessels
Structure of Enamel, Dentin and Pulp
Enamel is a highly mineralized tissue of ectodermal origin. It is 96% mineral, 4% water.
It is very brittle but the underlying dentin provides some resilience
Physical, chemical and histological pattern on enamel enables it to withstand the masticatory and other insults on the teeth
Enamel: Physical properties -
Color: yellowish white to grayish white
Thickness: Thick at the incisal edge and cusp tip of molar and premolars (2-2.5 mm) and ends cervically as knife edge.
Hardness: it is the hardest calcified tissue in the human body because of its calcification and crystal orientation.
Brittleness: Enamel is brittle especially when looses the underlying elastic healthy dentin
Permeability: Enamel acts as a semi-permeable membrane
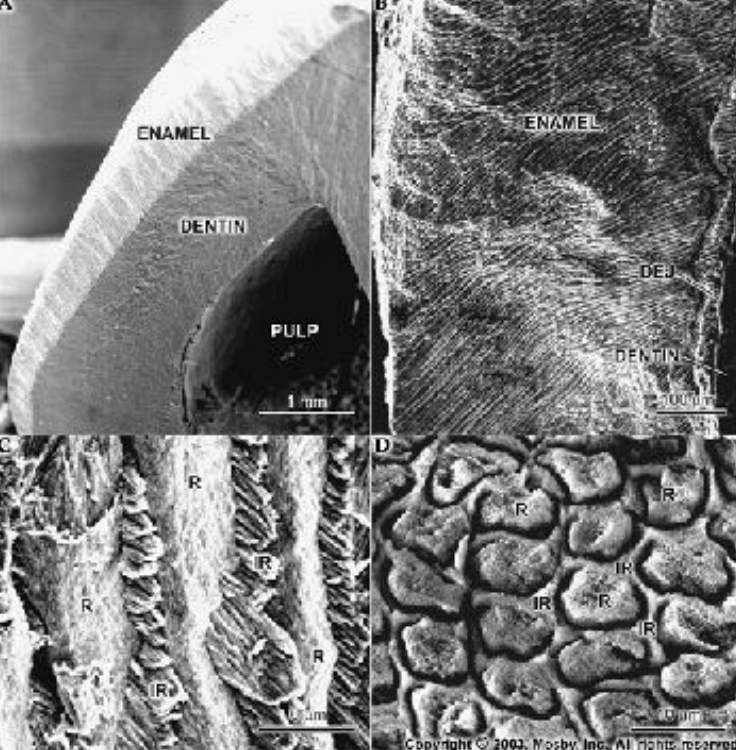
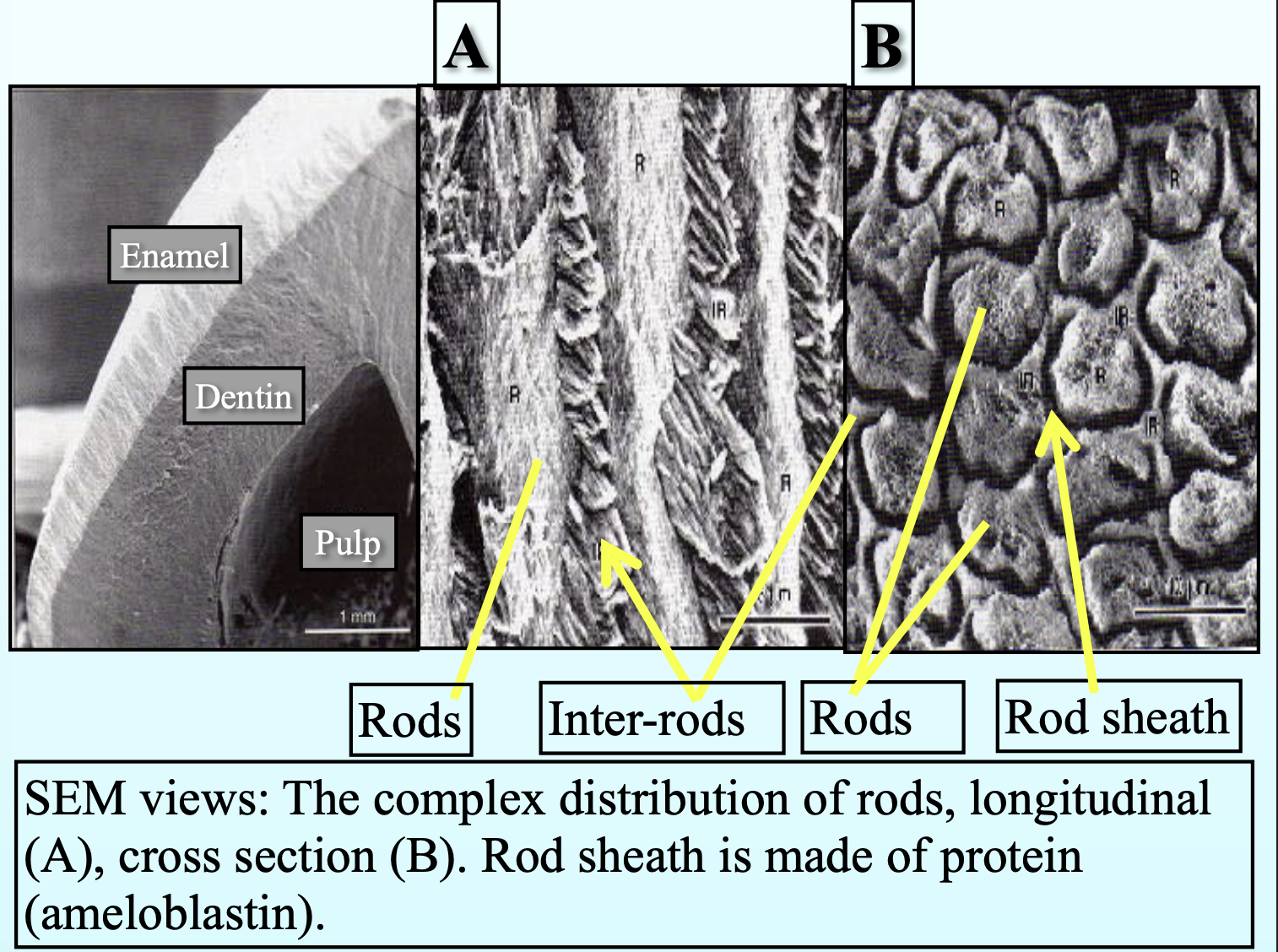
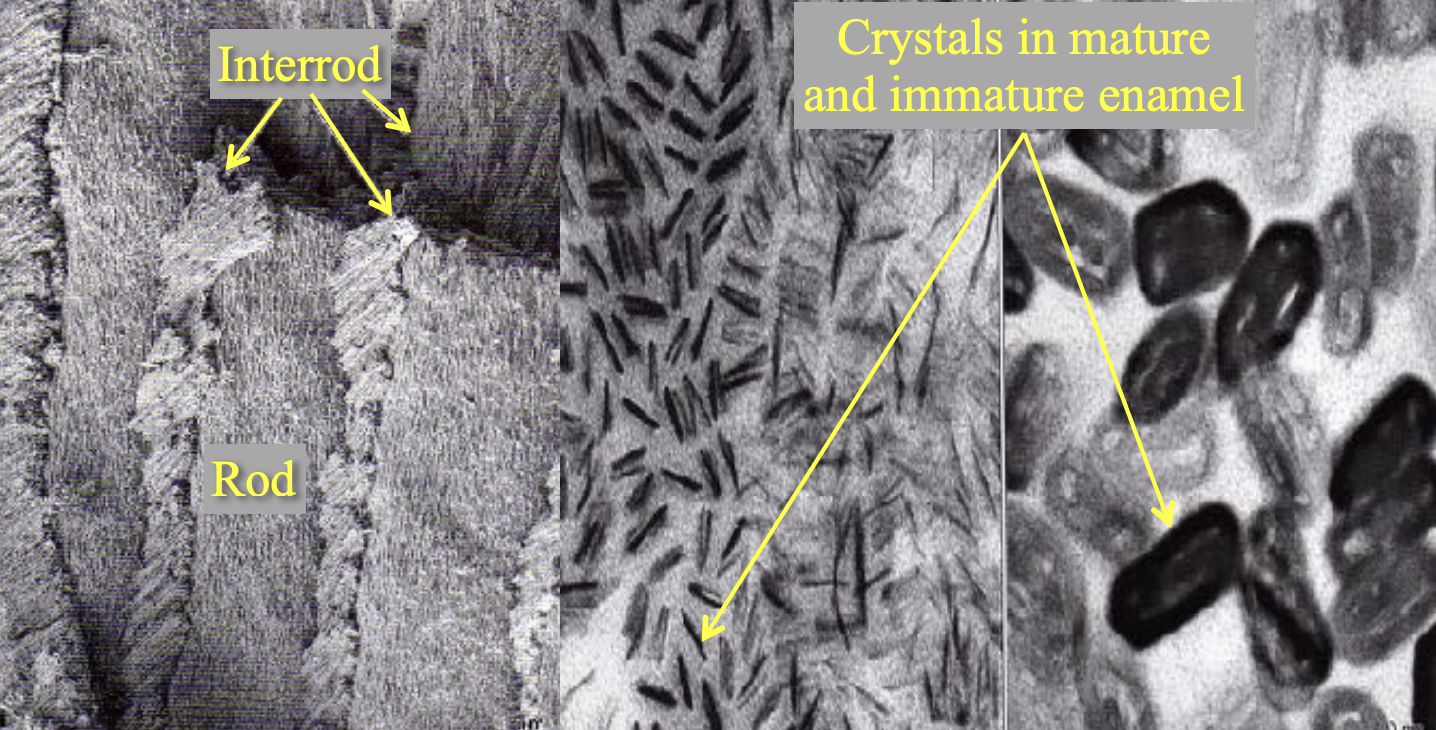
Enamel strucure:
Organized into rods (prisms) and interrods (inter prismatic) substance
The boundary between rod and interrod is delimited by a narrow
space containing organic material – rod sheath
Average diameter of the enamel rod is 4-5 µm
Crystals that make up rod and interrod are long, ribbon like structures. They are similar in structure and composition but diverge in orientation.
Enamel Structure:
Striae of Retzius: Dark lines seen in longitudinal sections, running from the DEJ (dentino-enamel junction) to the tooth surface. They show the weekly pattern of enamel formation.
Cross Striations: Fine lines seen every 4 micrometers across enamel rods, showing daily growth.
Hunter-Schreger Bands: Light and dark bands seen under a microscope, caused by changes in the direction of enamel rods.
Gnarled Enamel: Twisted enamel rods near the DEJ, especially at the cusp tips, giving a swirled appearance.
Neonatal Line: A clear line in enamel that separates enamel made before birth from that made after birth.
Surface Enamel: The outermost layer is harder and has no visible prisms (prism-less).
Enamel Tufts: Small, brush-like structures starting from the DEJ and extending into enamel. They contain more organic material and are areas where rod direction changes.
Enamel Lamellae: Thin cracks or lines from the enamel surface to the DEJ, formed due to disturbances during development.
Perikymata: Fine grooves on the enamel surface that reflect the incremental growth of enamel.
DEJ (Dentino-Enamel Junction): The wavy boundary between dentin and enamel. Its scalloped shape helps resist chewing forces.
Enamel Cuticle (Nasmyth’s Membrane): A thin layer covering the newly erupted tooth, made by ameloblasts.
Enamel Spindles: Extensions of dentin tubules (from odontoblasts) that may extend into enamel during early development.
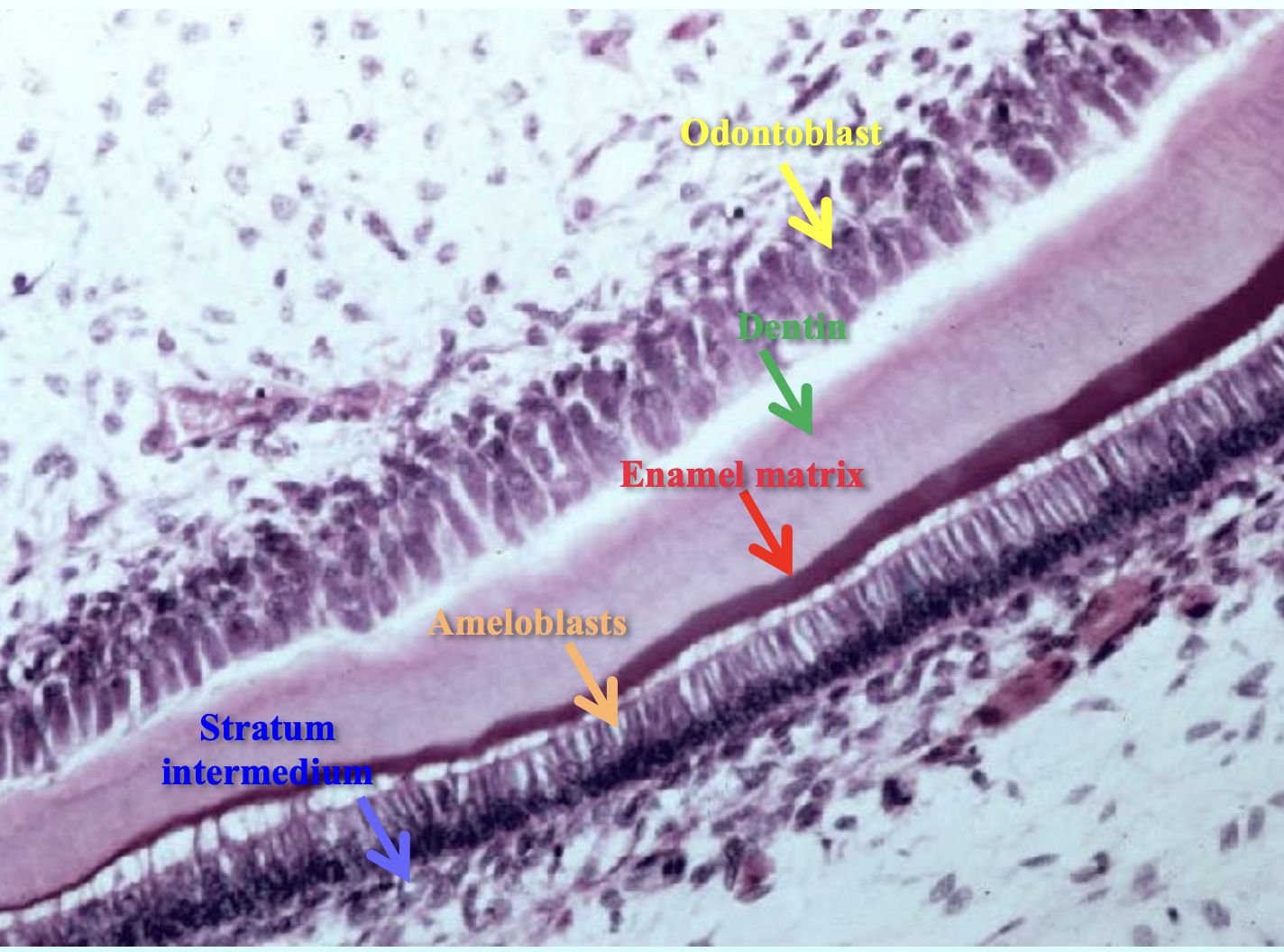
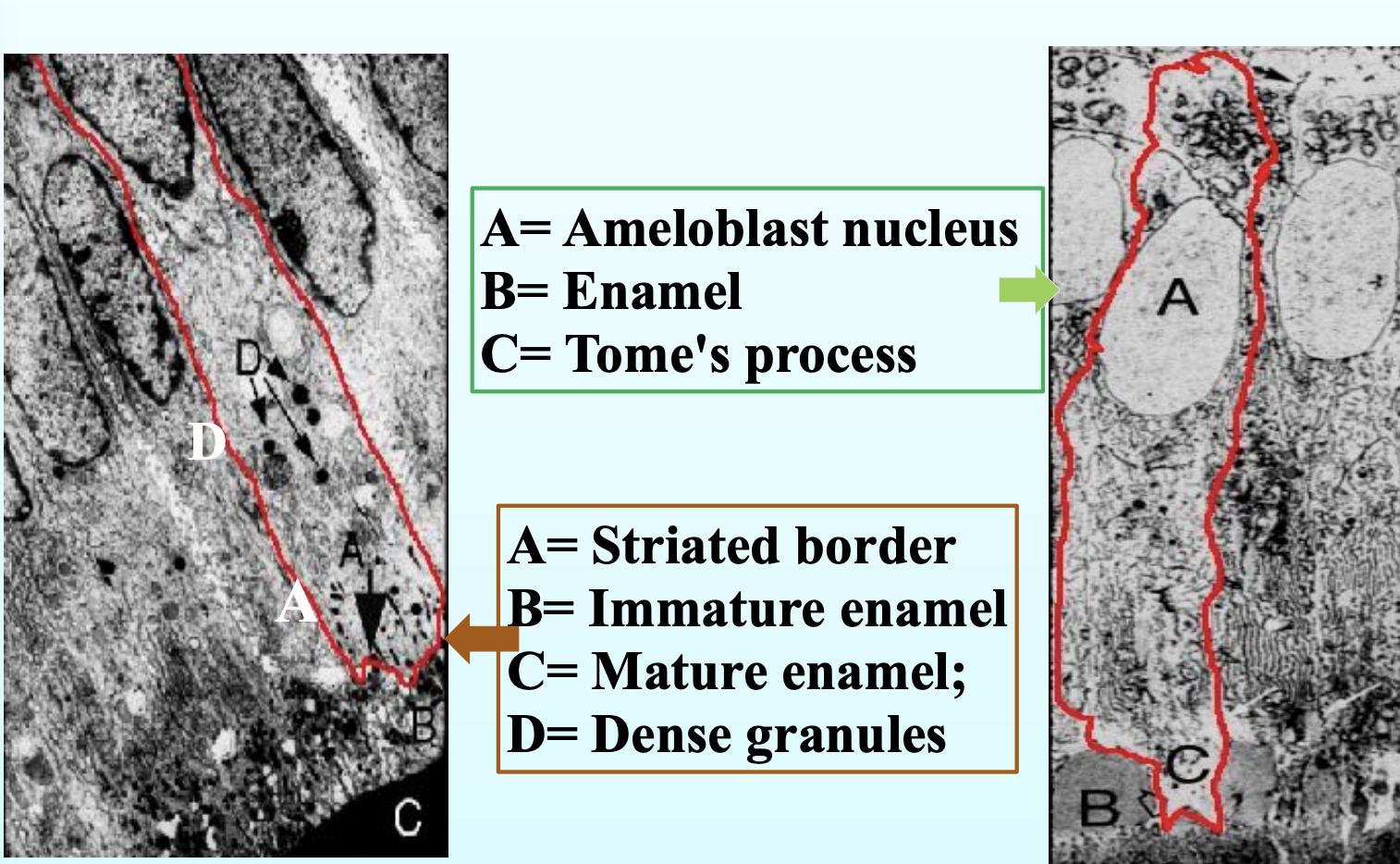
Secretory amerloblasts:
Secretory ameloblasts are enamel-forming cells that are active during the stage when enamel is being laid down.
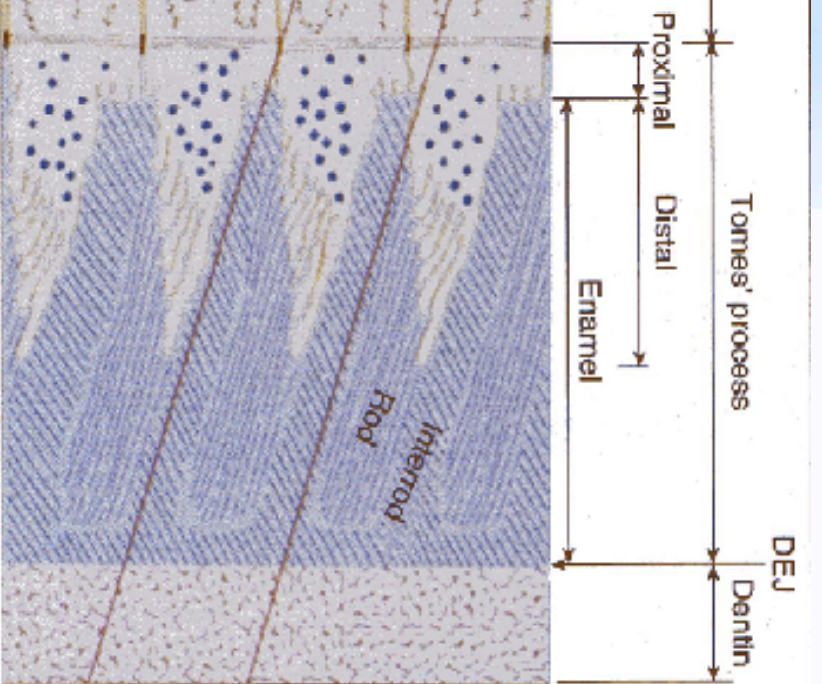
They have a special projection at their tip called the Tomes’ process.
This Tomes’ process helps in forming two parts of the enamel:
Rod enamel: tightly packed, organized enamel that forms the core of each enamel rod.
Interrod enamel: the enamel that lies between the rods, slightly different in direction and structure.
During maturation stage of enamel formation, the enamel hardens and the pre-existing hydroxypatite crystals of the enamel row in width and thickness and NO more new crystals are formed.
Tomes processes are not apparent at this stage.
The maturation stage is made up of transitional phase and the maturation proper phase.
Transitional phase: comes after the full thickness of the enamel is formed.
The Ameloblasts (AB) undergo a lot of morphological changes that prepares them for the maturation of the enamel
Maturational proper phase: during this phase, the ameloblasts become more involved in the removal of water and organic material
They also undergo apoptosis so that approximately 25% of the ameloblasts die during the transitional phase and an additional 25% die during the MP phase
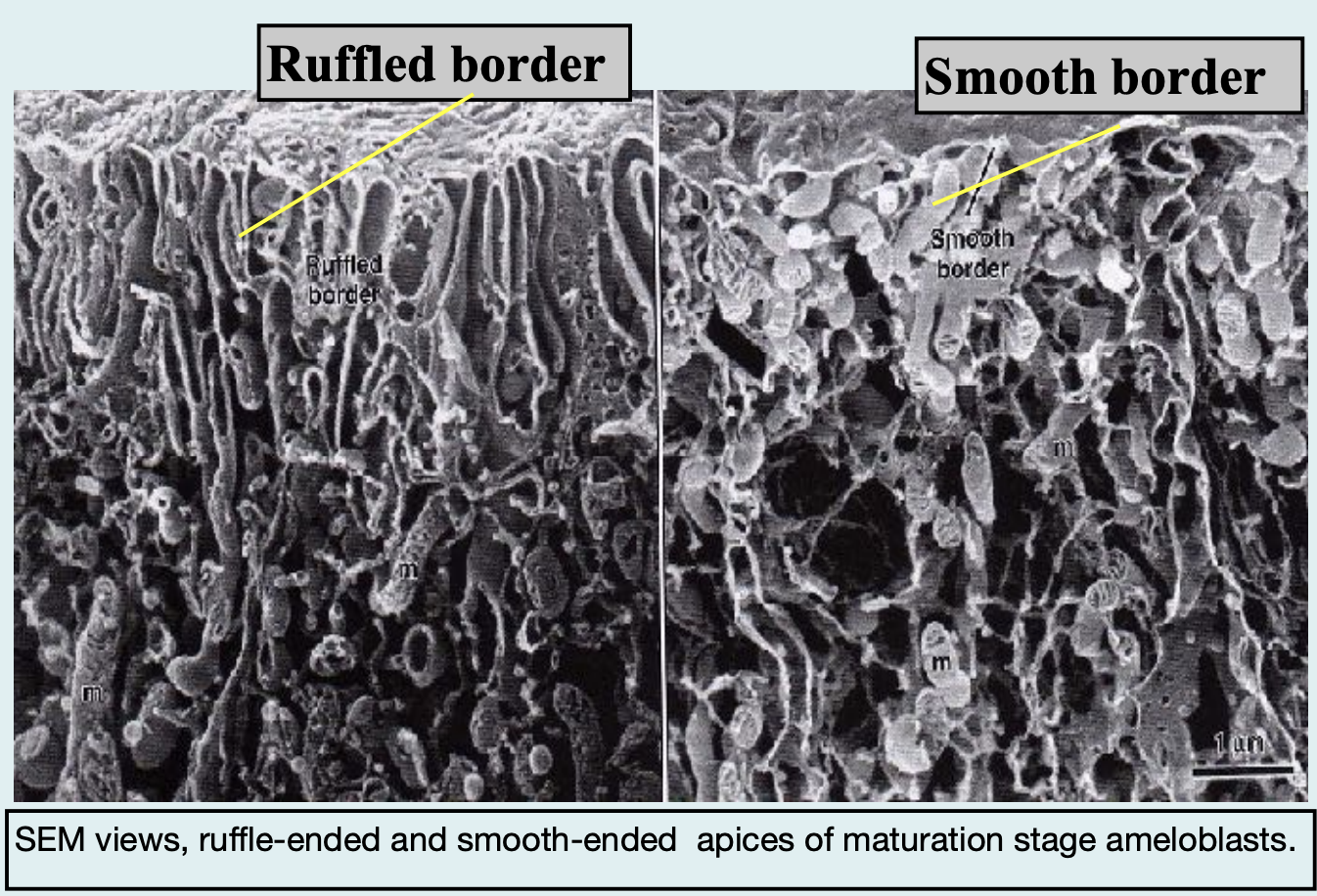
During enamel maturation, ameloblasts change their shape and function to help remove water and proteins and allow minerals (like calcium and phosphate) to enter the enamel, making it harder.
They do this by switching between two surface types:
Ruffle-ended ameloblasts:
Have a folded or ruffled edge (like little waves).
Help pump calcium and phosphate into enamel.
Involved in mineral deposition.
Smooth-ended ameloblasts:
Have a flat or smooth edge.
Help remove water and proteins from enamel.
Involved in cleaning up the enamel.
🔄 Ameloblasts alternate between these two forms during maturation to balance mineral addition and protein removal, which is crucial for making strong, fully developed enamel.
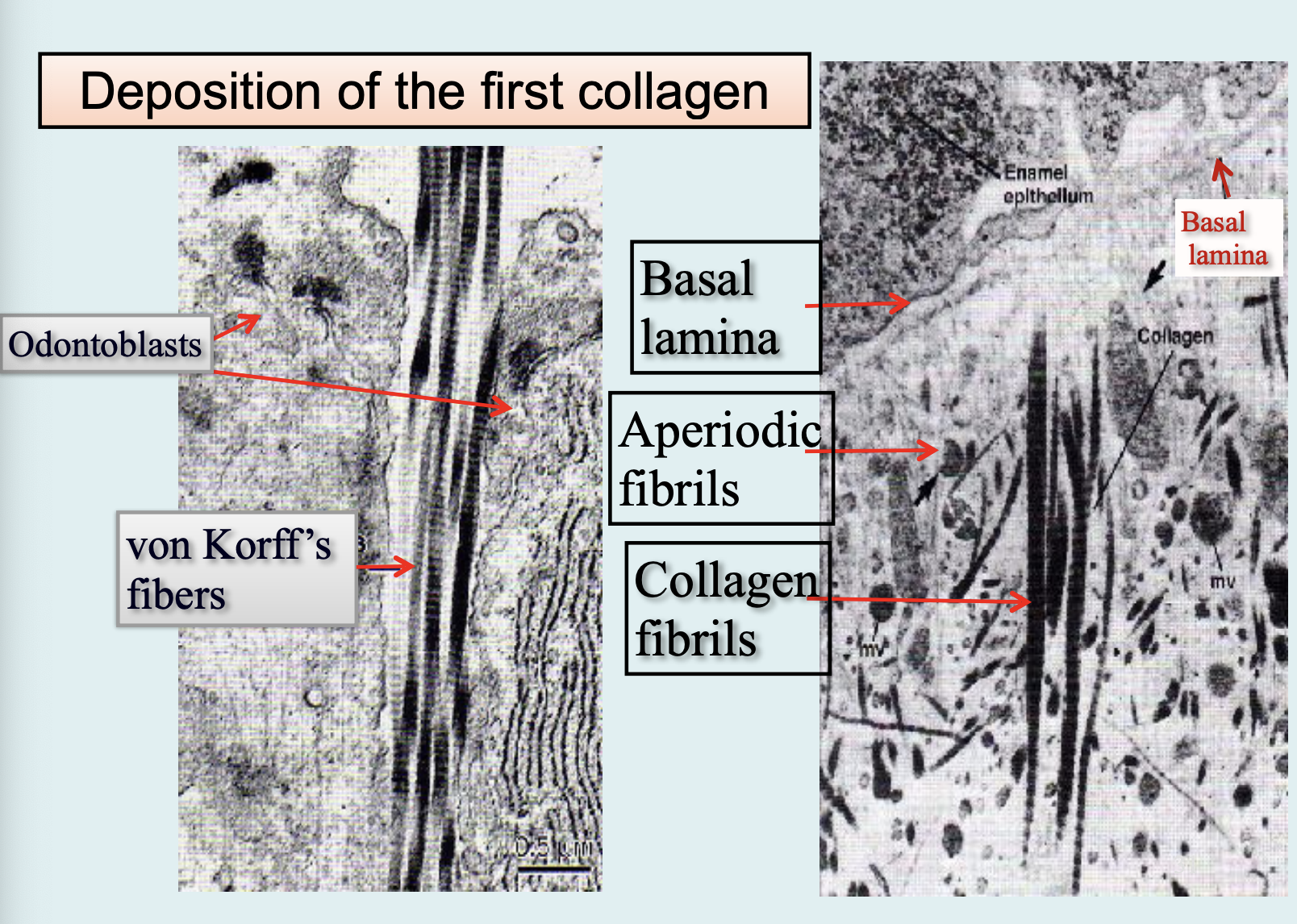
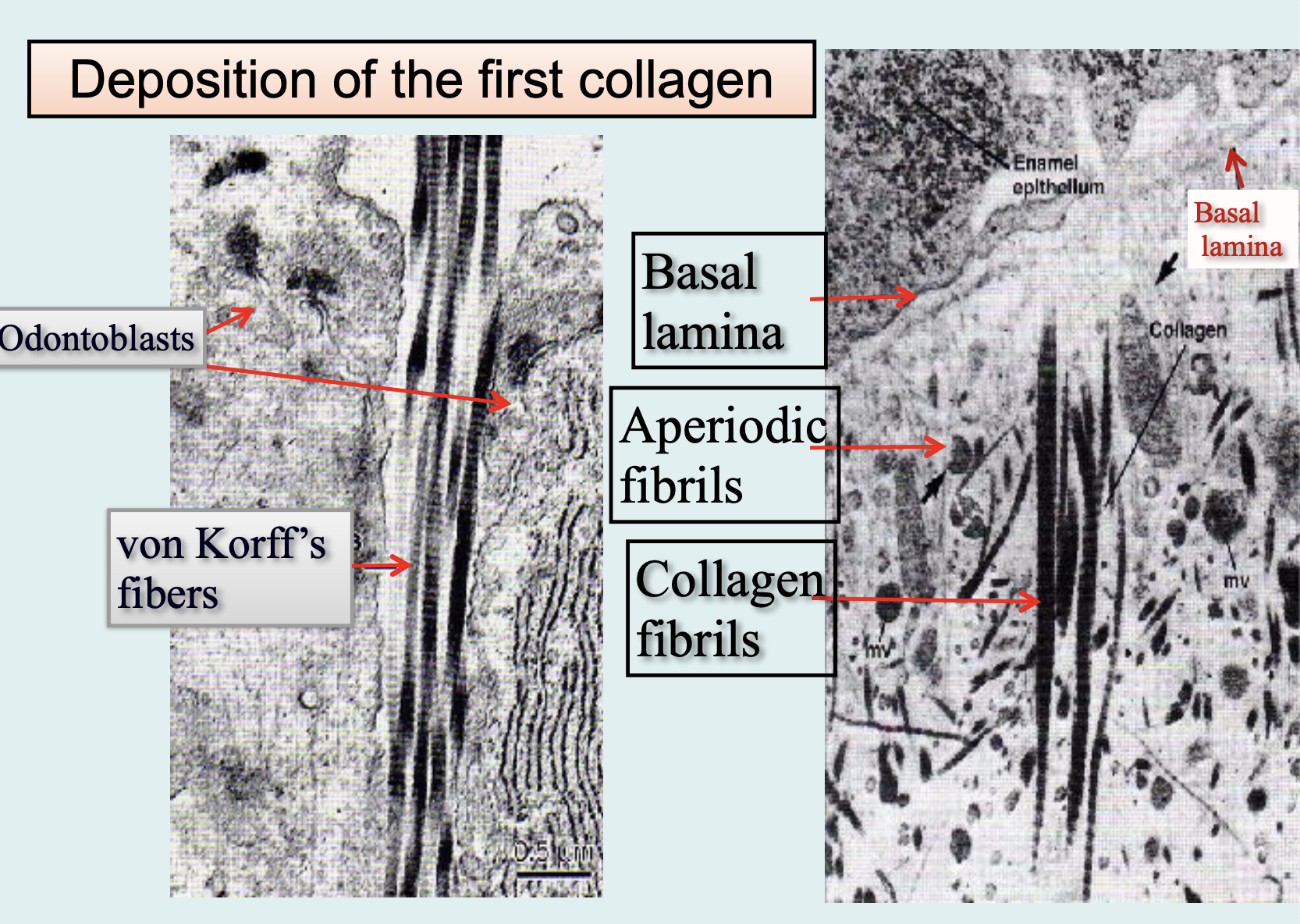
Dentin is first deposited as a layer of pre-dentin - Unmineralized matrix. It contains principally of collagen and non-collagenous components - similar to osteoid.
Physical and chemical properties
It has an elastic quality that is important to the functioning of the tooth
It is yellowish in color
It gradually mineralizes to form dentin
Mature dentin is 70% inorganic, 20% organic, and 10% water by weight
Inorganic – hydroxyapatite in the form of small plates
Organic – collagen types I, III and V with small amounts of lipids and non-collagenous matrix proteins
Harder than bone and cementum but softer than enamle
Type 1 collagen
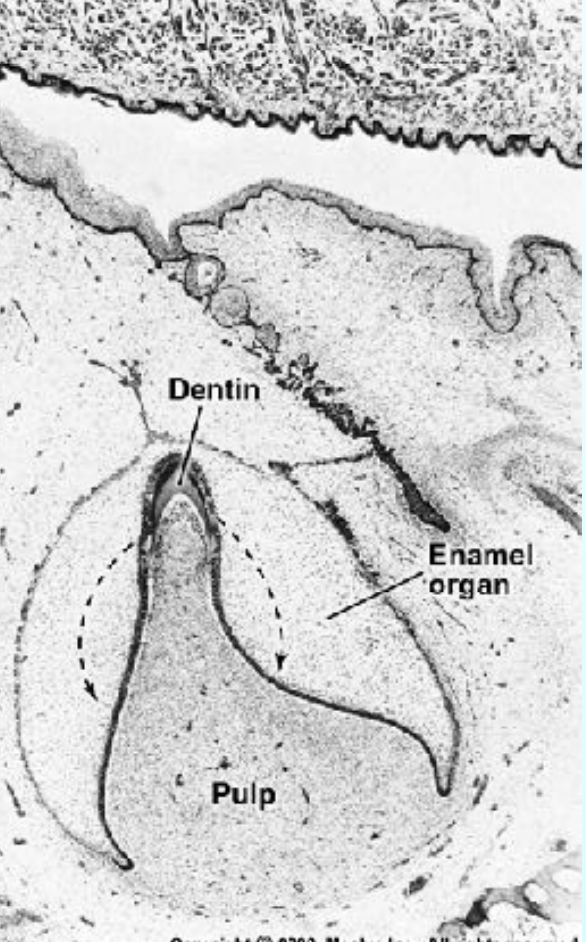
Pattern of dentin formation begins at the bell stage.
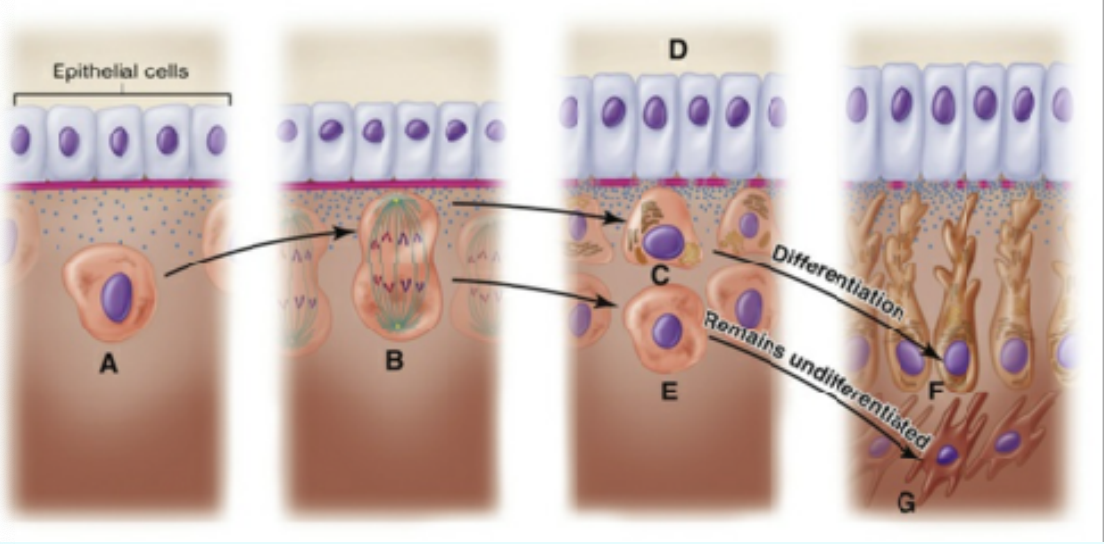
Odontoblast differentiation:
The undifferentiated ectomesenchymal cell (A) of the dental papilla divides (B), with its mitotic spindle perpendicular to the basal lamina (pink line). A daughter cell (C), influenced by the epithelial cells and molecules they produce (D), differentiates into an odontoblast (F). Another daughter cell (E), not exposed to this epithelial influence, persists as a subodontoblast cell (G). This cell has been exposed to all the determinants necessary for odontoblast formation except the last.
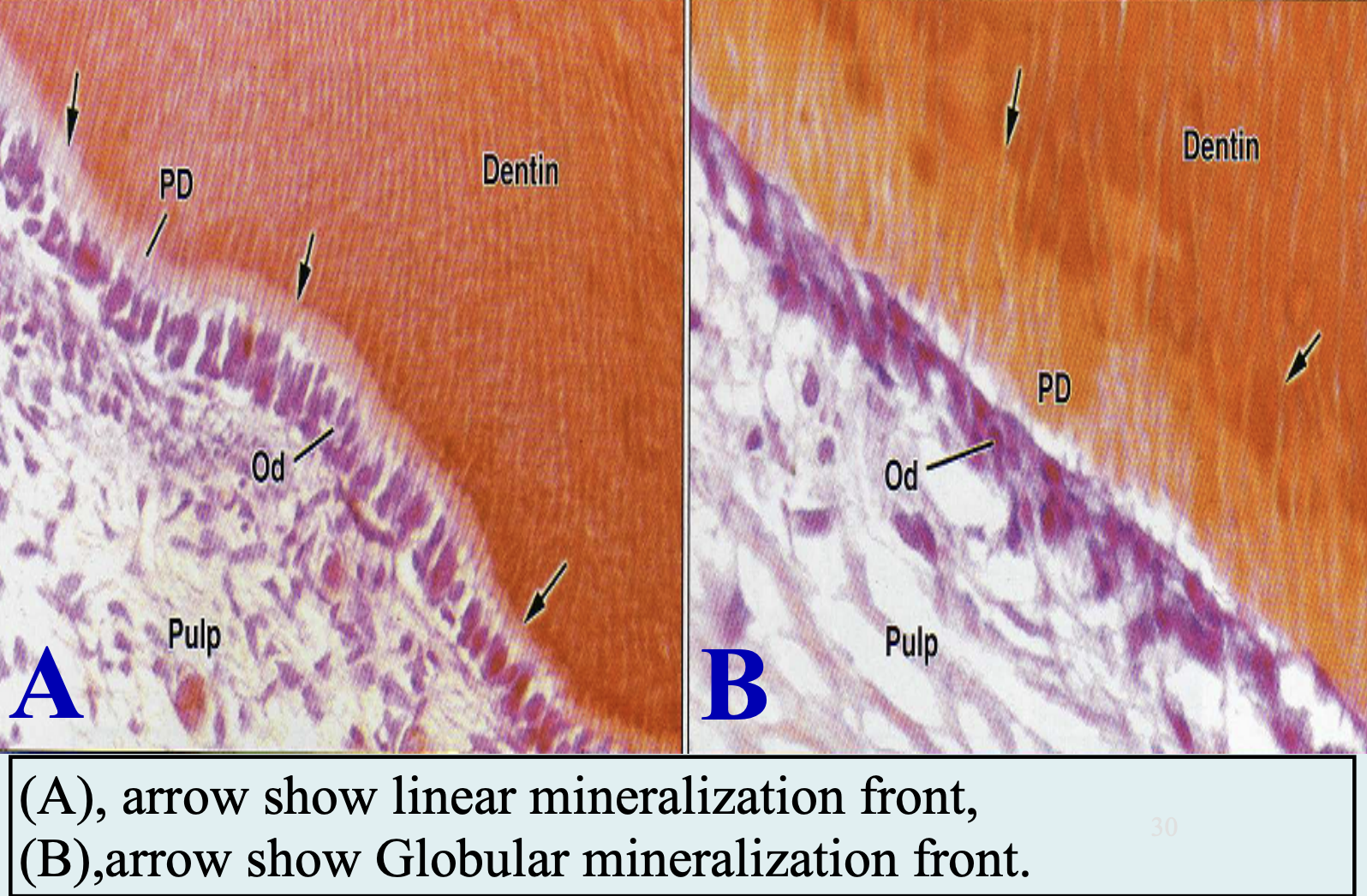
Mineral phase first appears within the matrix vesicles as single crystals - thought to be seeded by the phospholipids of these vesicles or odontoblasts
Crystals grow rapidly and rupture from the confines of the vesicles and spread as clusters of crystallites that fuse with adjacent ones
The organic pre-dentin is always found between the odontoblasts and the mineralization area
Mineralization is controlled through the secretion of matrix proteins- Dentin proteins
Formation of Root Dentin:
Compositionally different that of the coronal dentin
The collagen fibers in the mantle dentin are arranged in a different orientation
The degree of root dentin is also less
Rate of deposition of dentin is slower
Dentin Histology:
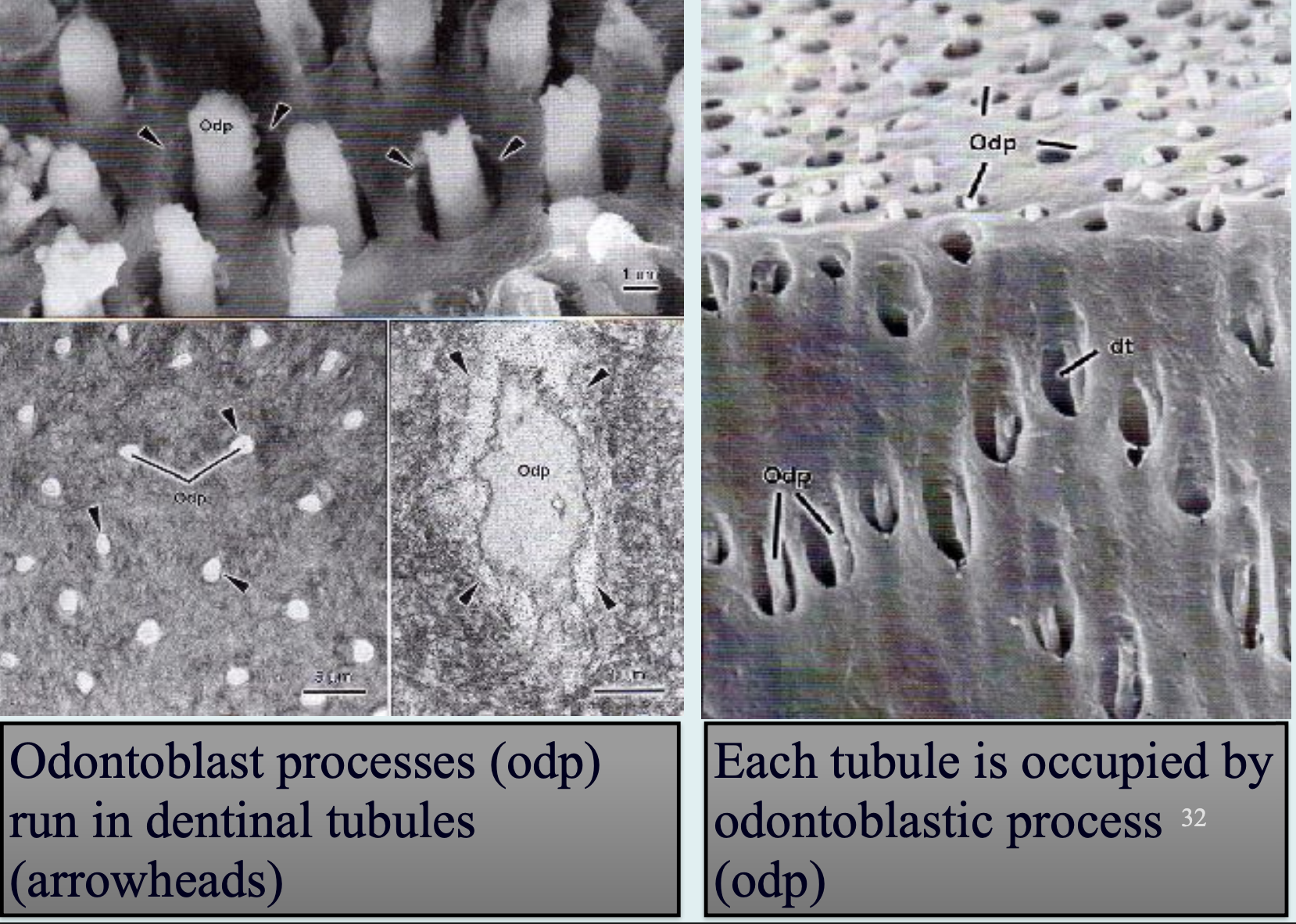
Dentinal Tubules:
Extend from DEJ to pulp.
S-shaped path, denser near pulp.
Help in caries spread.
Reflect path of odontoblasts.
Predentin:
Newly formed, unmineralized dentin.
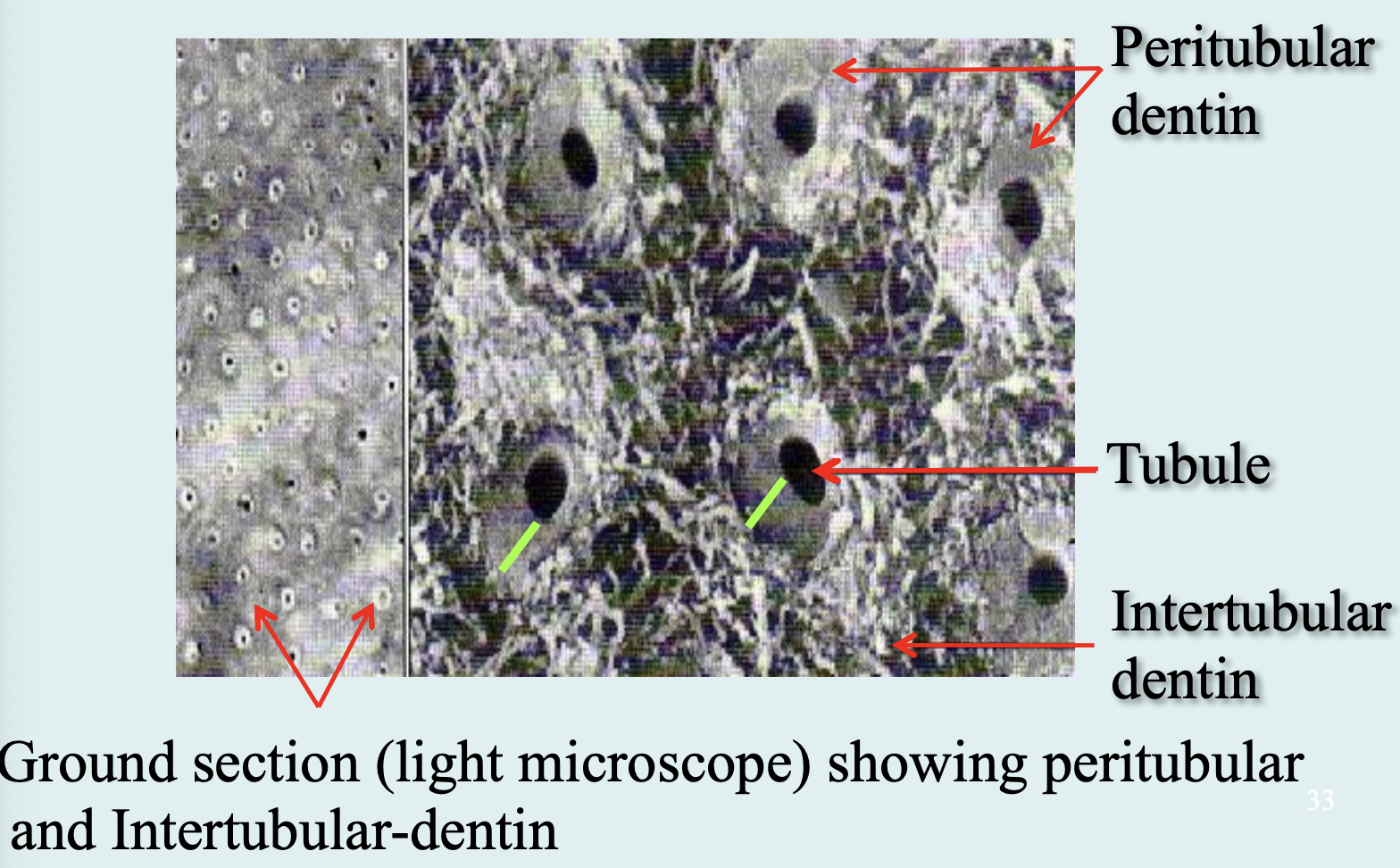
Peritubular Dentin:
Surrounds tubules, 40% more mineralized.
Intertubular Dentin:
Between tubules; main dentin made by odontoblasts.
Interglobular Dentin:
Poorly mineralized spots beneath mantle dentin.
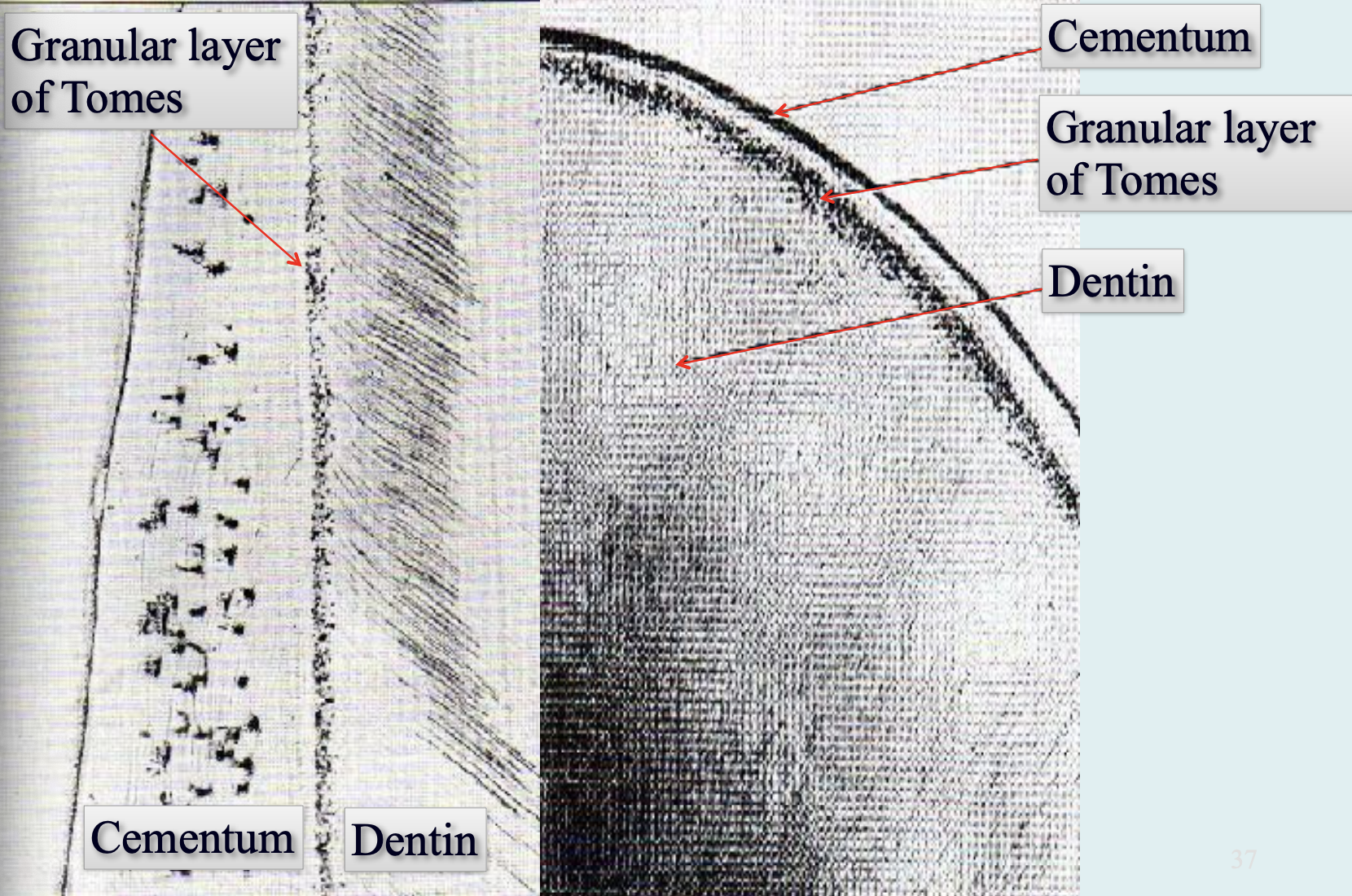
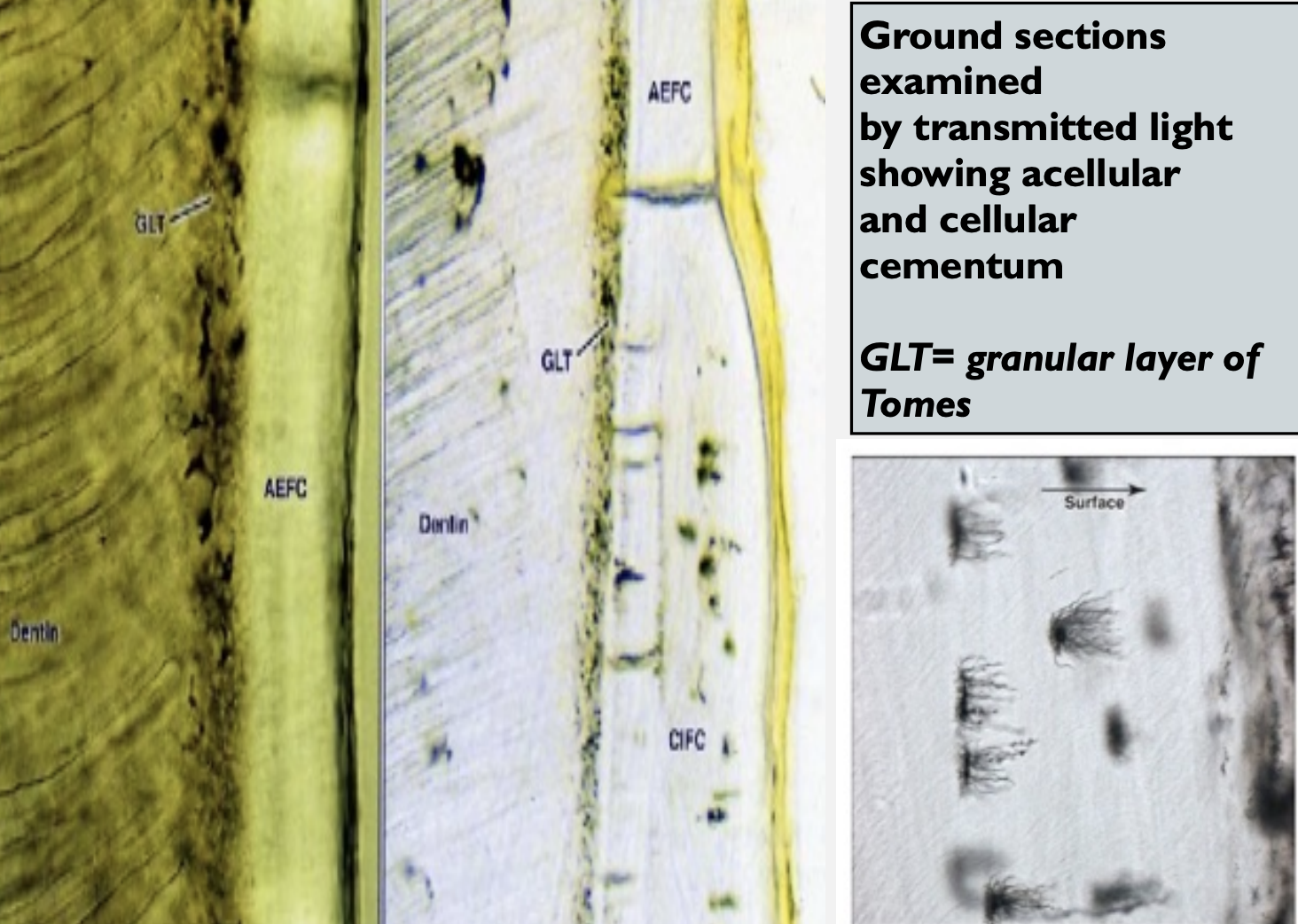
Tomes’ Granular Layer:
Granular appearance in root dentin under cementum.
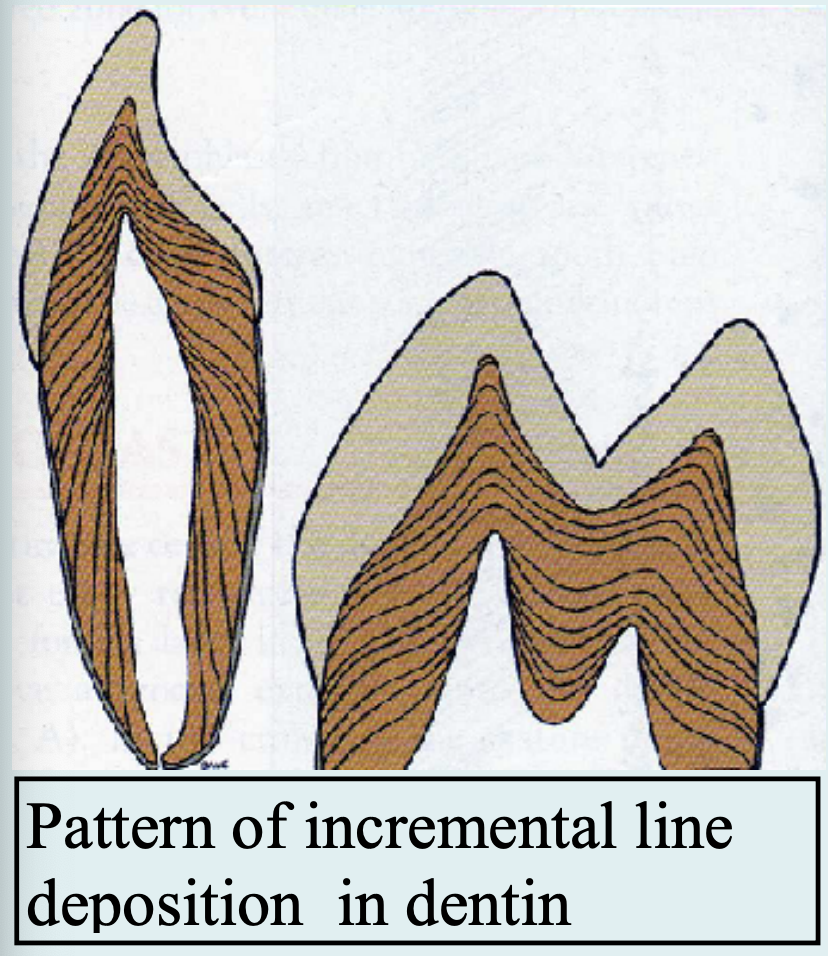
Von Ebner Lines:
Daily growth lines (~4 µm apart).
Odontoblastic Process:
Cell extension inside tubules, contains organelles.
Mantle Dentin:
First dentin near DEJ, less mineralized, type III collagen.
Circumpulpal Dentin:
Main body of dentin formed before root completion.
There are three types of dentin:
Primary dentin: Forms most of the tooth, and outlines the pulp chamber and is referred o as circumferential dentin. The outer layer is mantle dentin (Mineralized differently)
Secondary dentin: Develops after root formation has been completed, it represents the continuing deposition of dentin by odontoblasts. The dentinal tubules are less organized than the primary dentin, some regions may lack tubules or have thicker tubules. (esp in molars
Tertiary dentin: Reactive or reparative dentin, it is produced in reaction to various stimuli. They are produced only by those cells ffected by the stimulus
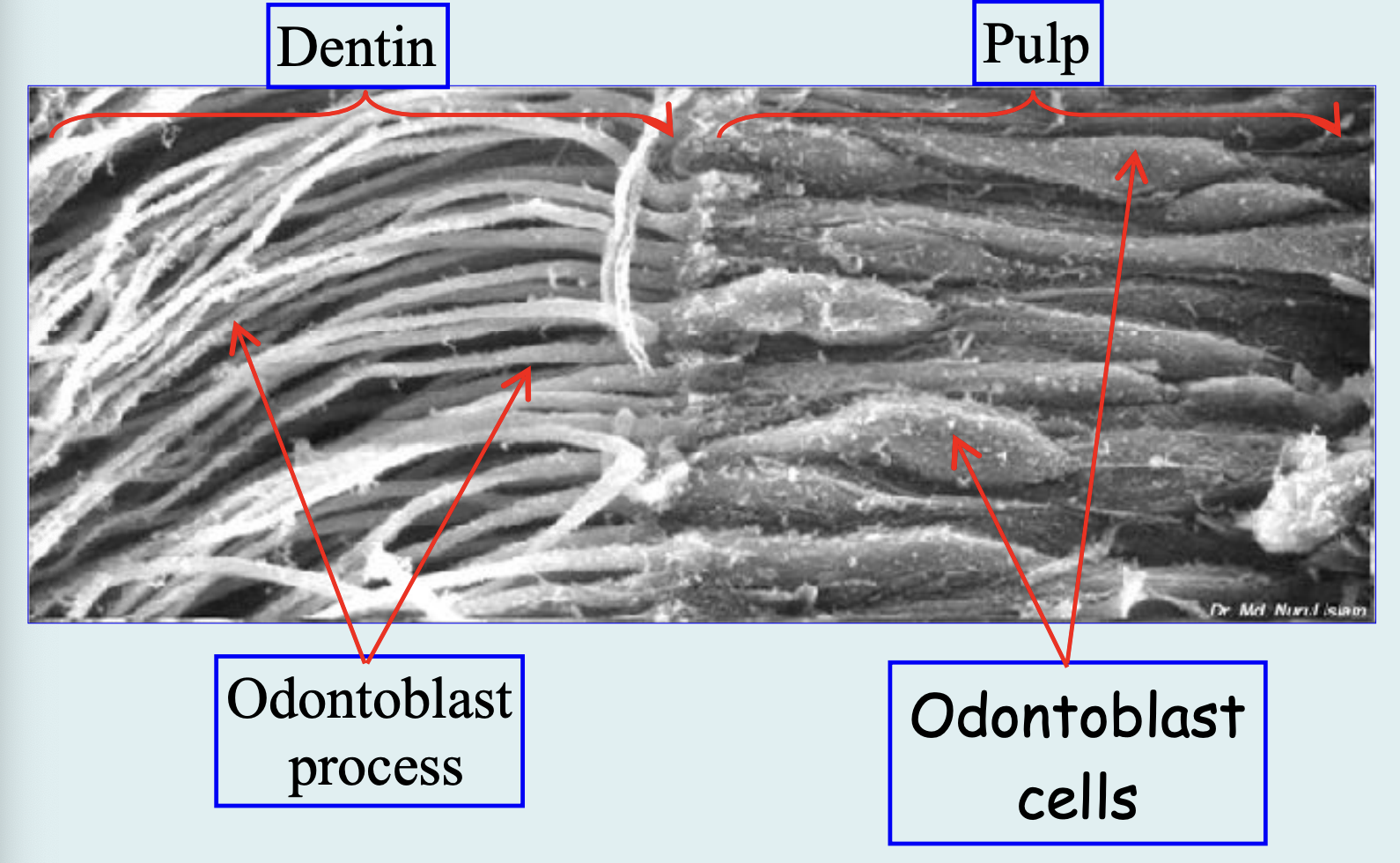
Pulp:
Pulp is Soft connective tissue that supports the dentin
Four distinct zones
odontoblastic zone at the periphery
cell-free zone of Weil
below the ODs
cell-rich zone
pulp core – major vessels and nerves
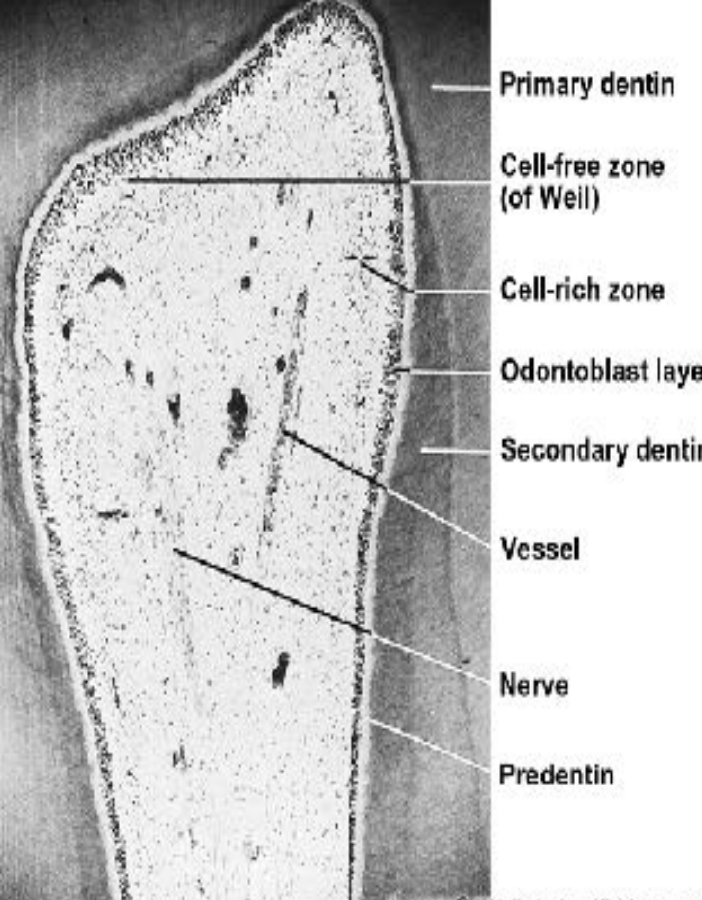
Pulp zones:
Odontoblasts: They line the periphery of the pulp chamber - Larger at the crown region.
Cell free zone of Weil: Some feel it is an artifact
Cell rich zone: Fibroblasts, undifferentiated mesenchymal cells, defense cells, fibers and dendritic cells
Pulp core: Glycosaminoglycans, glycoproteins, and water.
Pulp cells and functions:
Fibroblasts: Greater number - numerous in the coronal portion of the pulp - form the cell rich zone.
Ectomesenchymal cells: Undifferentiated cells of the pulp
Macrophages
Lymphocytes
Dendritic cells
Functions of the pulp:
Inductive
Formative
Nutritive
Protective
Reparative
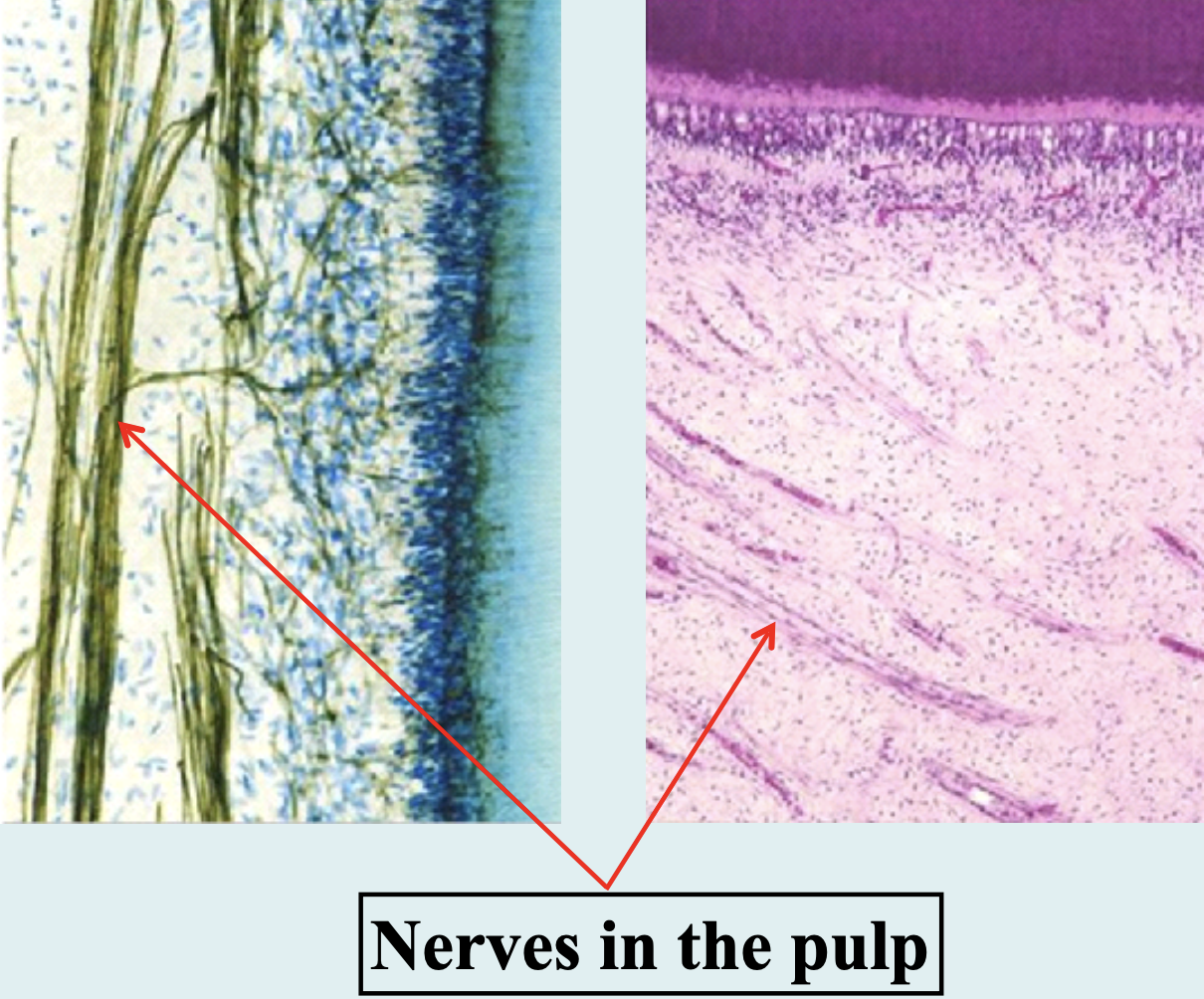
Pulp Vascular & Nerve supply:
Enter and exit via the apical foramen as a bundle of vessels and
nerves
Smaller vessels and nerves enter through the minor foramina
Arteries increase their lumen and decrease their wall thickness as they enter the pulp
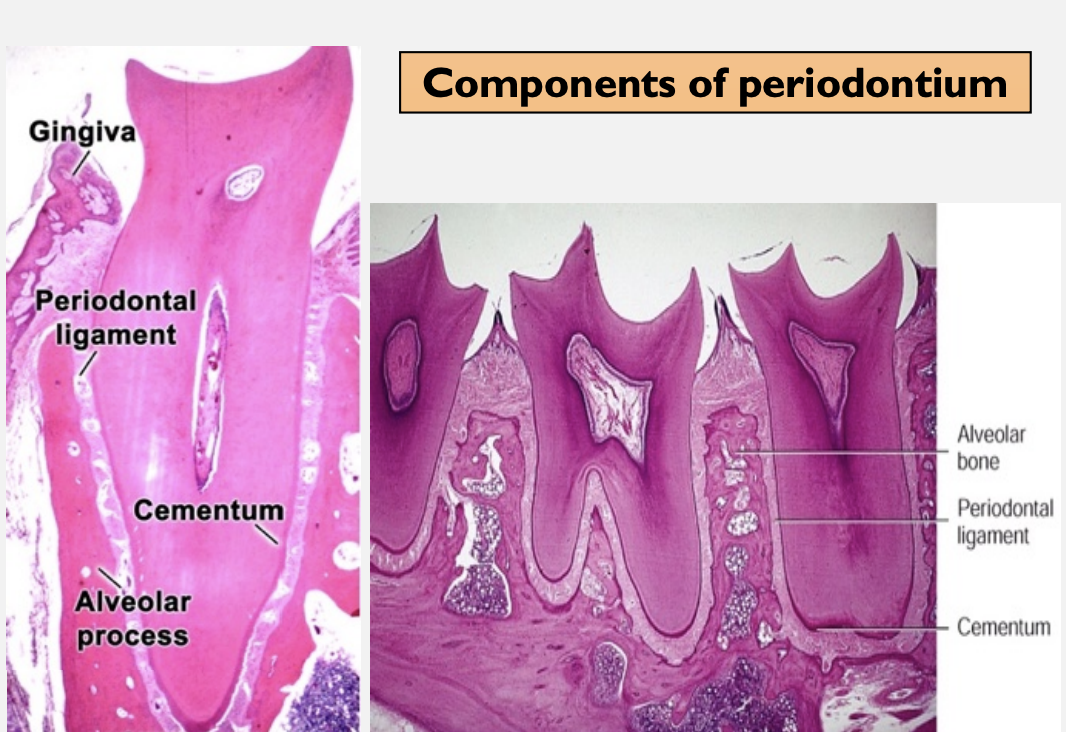
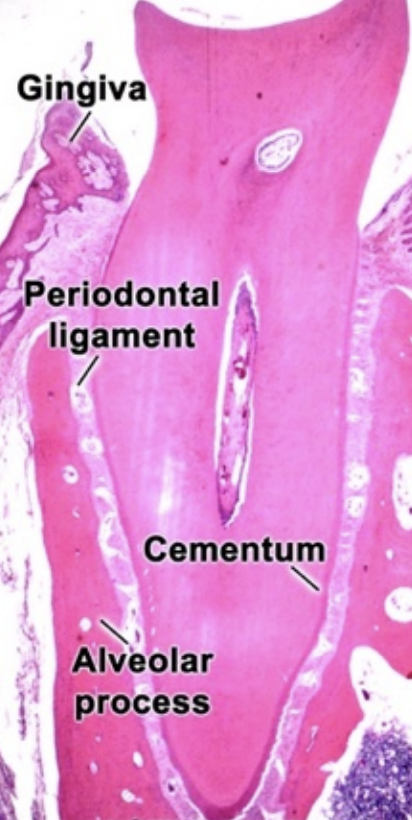
Structures of Periodontium- Cementum, Periodontal Ligament & Alveolar Bone
Periodontium is tissues, which support and invest the tooth.
These include:
Cementum
Periodontal ligaments (PDLs)
Alveolar bone (bone lining the socket)
Gingiva (gum that facing the tooth)
Cementum is a hard avascular connective tissue that covers the roots of the teeth. It covers and protects the root dentin and provides attachment of the periodontal fibers.
The biochemical comppsition of cementum is similar to bone:
Inorganic part: 45% - 50% hydroxypaptite
Organic part: 50% - 55% collagen and non-collagenous matrix proteins and water
Type 1 collagen is the predominant (90%) in cellular cementum
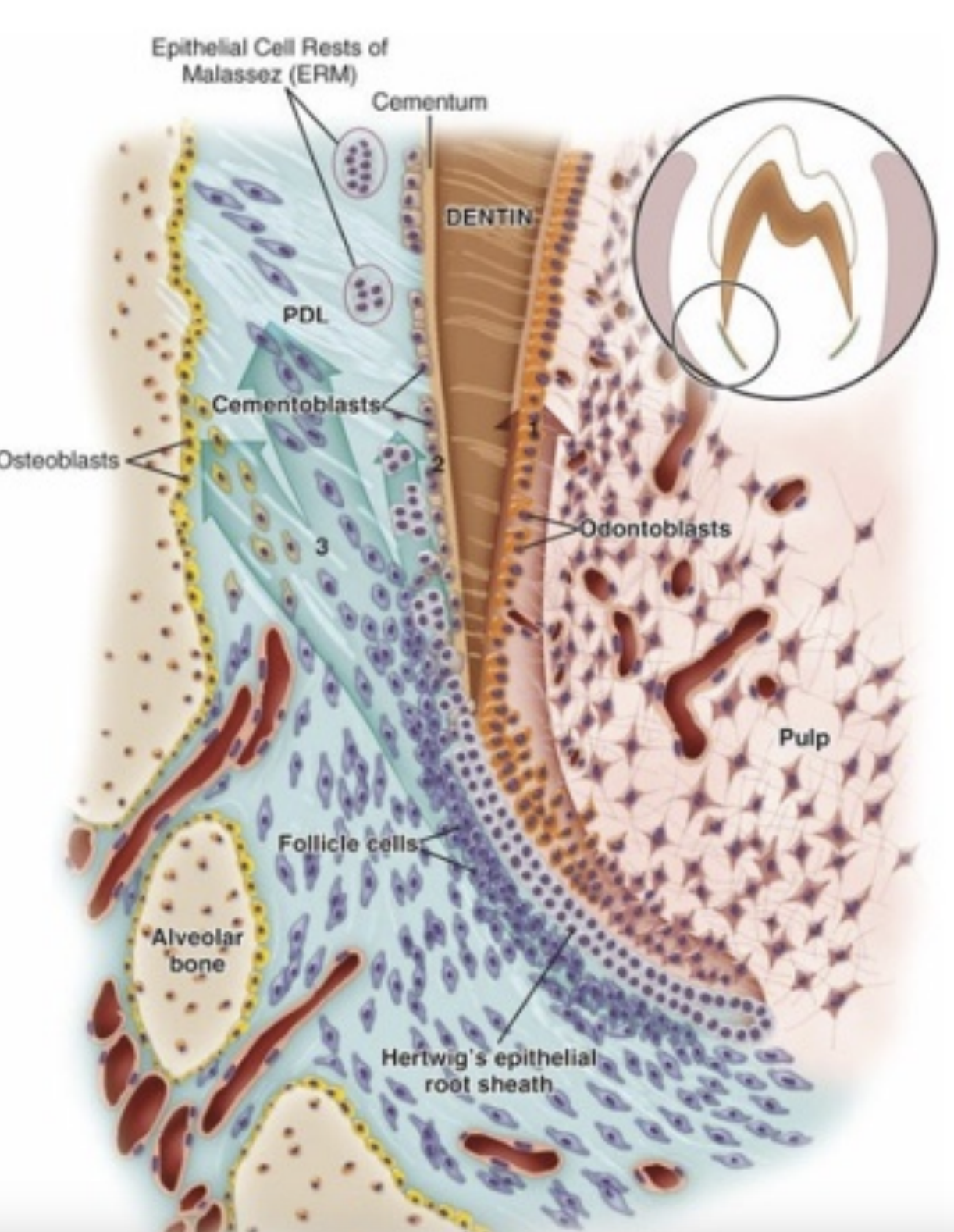
Cementum Formation:
Cementoblasts (cells that form cementum), PDL fibroblasts, and their signals come from the dental follicle.
Hertwig’s Epithelial Root Sheath (HERS) signals pulp cells to become odontoblasts and make predentin.
Some HERS cells turn into cementoblasts.
When the dental follicle touches predentin, cementum begins forming on the root.
As cementum builds up, some cementoblasts get trapped inside it and become cementocytes.
Cementocytes live in small spaces (lacunae) and send out tiny processes into canals (canaliculi).
Phosphate helps control how fast cementum forms.
Broken HERS cells become the Epithelial Rests of Malassez, which stay in the periodontal ligament (PDL) and help maintain and repair tissues there.
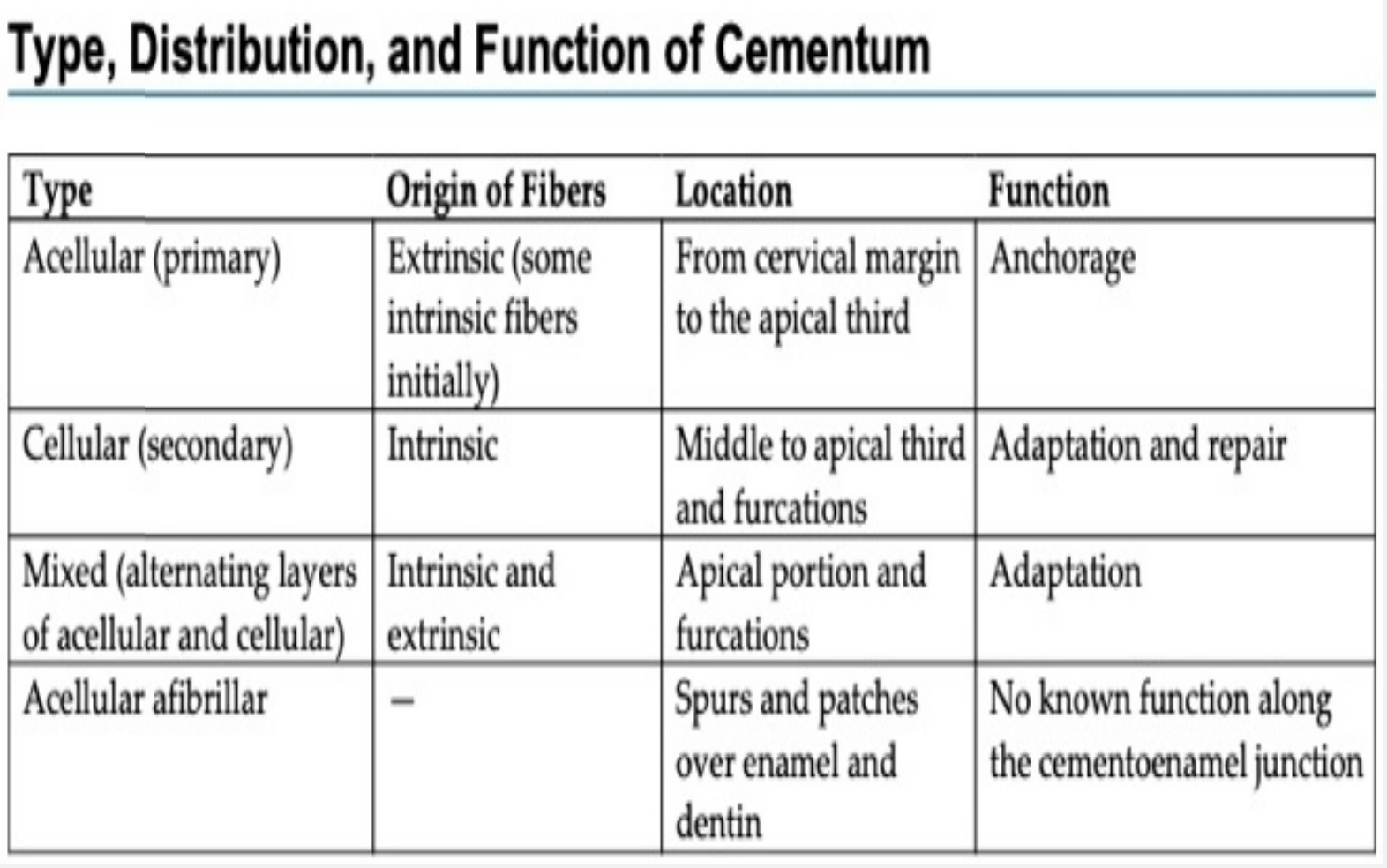
There are four types of cementum
Acellular extrinsic fiber cementum (primary cementum)
Cellular intrinsic fiber cementum (secondary cementum (secondary cementum)
Mixed (alternating layers of acellular and cellular cementum)
Acellular Afibrillar cementum
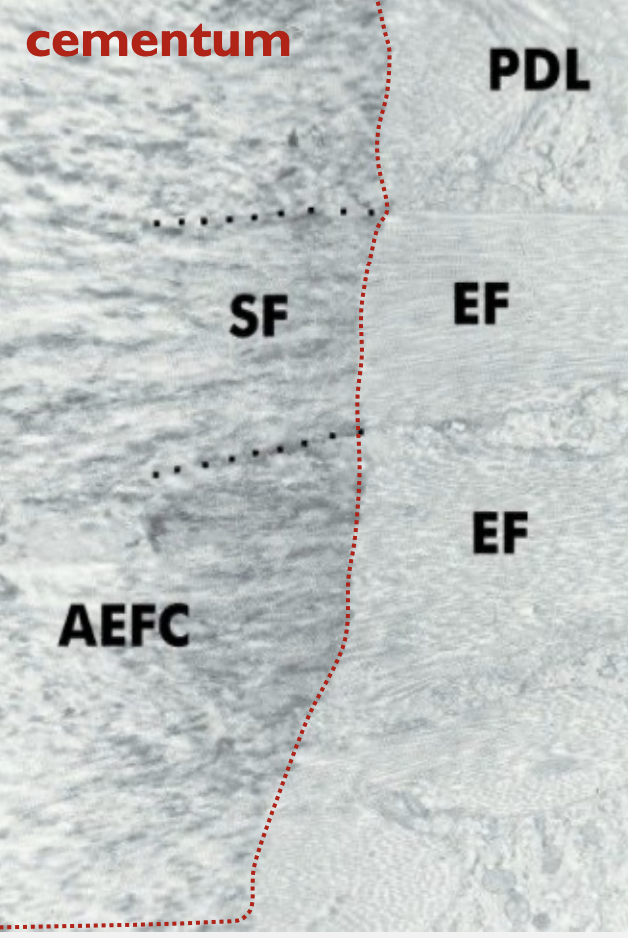
AEFC: Acellular extrinsic fiber cementum
EF: extrinsic fibers of cementum
SF: Sharpey's fiber. (Note: The dots outline the periphery of the fiber.)
PDL: periodontal ligament
There are 3 types of cementoenamel junctions:
Smooth: This occurs when the cementum and enamel join without any overlap.
Overlapping: In this type, the cementum extends over the enamel, creating a unique junction that may have implications for periodontal health.
Gap: This type features a noticeable space between the cementum and enamel, which can be prone to decay and disease.
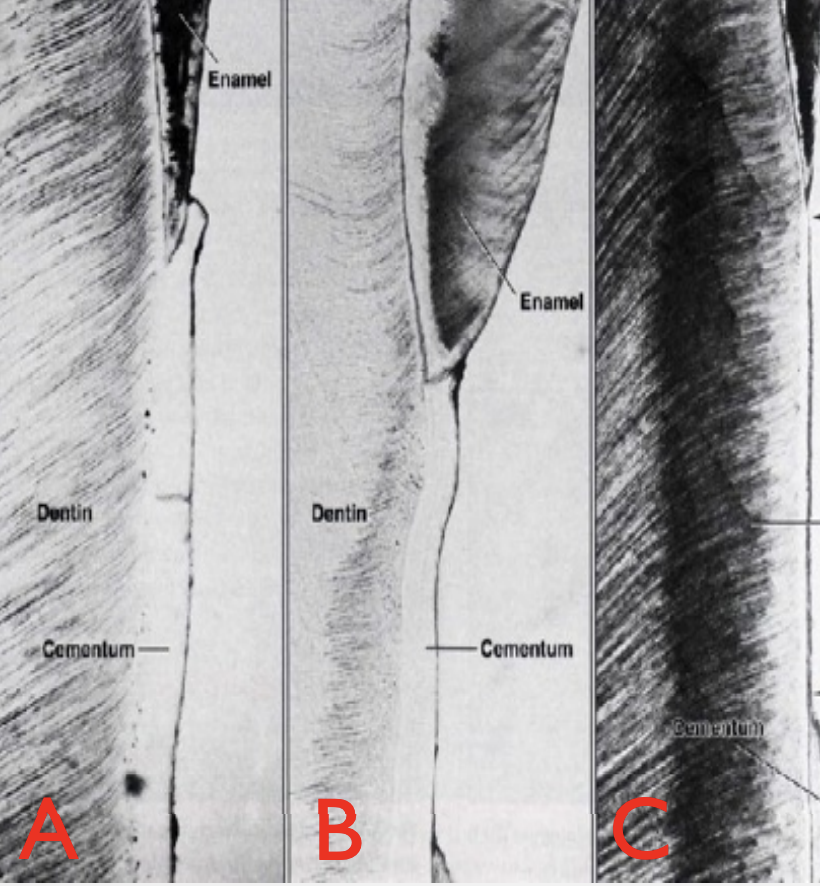
^
A - Cementum is overlapping enamel
B- Butt joint, enamel just meet cementum
C- Cementum deficiency, leaving root dentin exposed
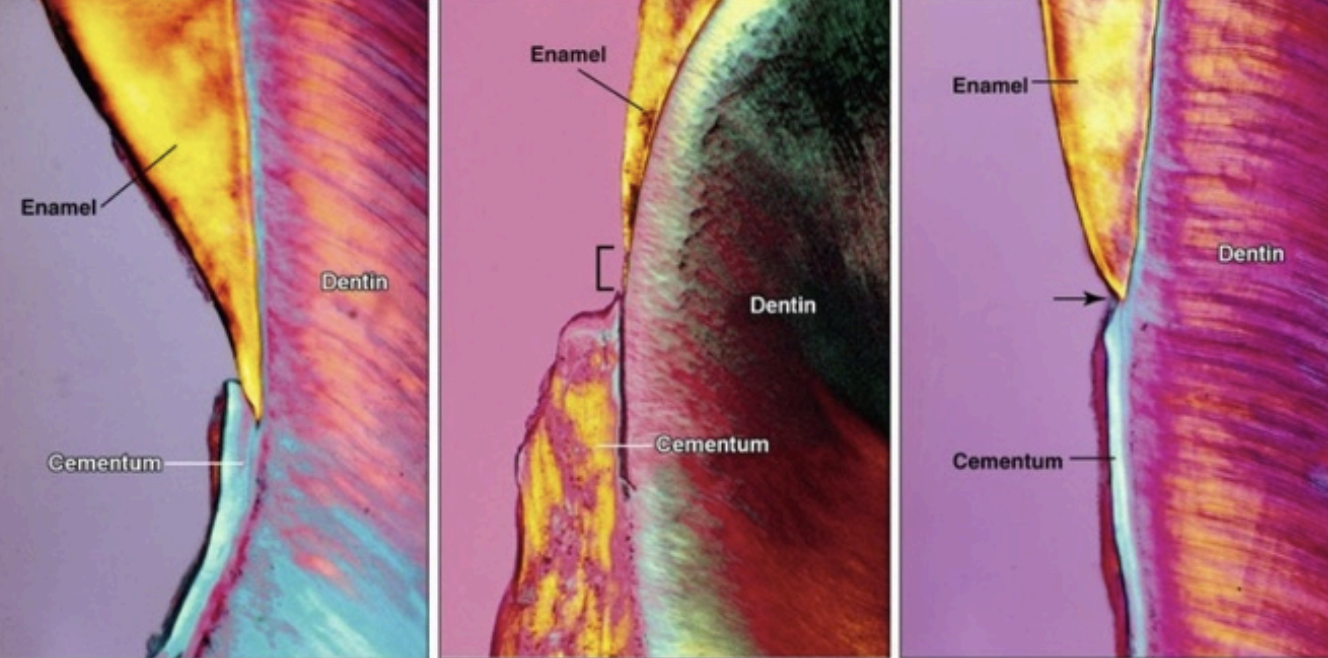
In 60% of the teeth, cementum overlaps the cervical end of enamel for a short distance.
In 30% of all teeth, cementum meets the cervical end of enamel in a relatively sharp line.
In 10% of the teeth, enamel & cementum do not meet.
Periodontal ligament is the soft specialized tissue situated between cementum and alveolar bone proper, it develops from dental sac or dental follicle. It also ranges in thickness between 0.15 and 0.3 mm and is thinnest in the middle portion of the root.
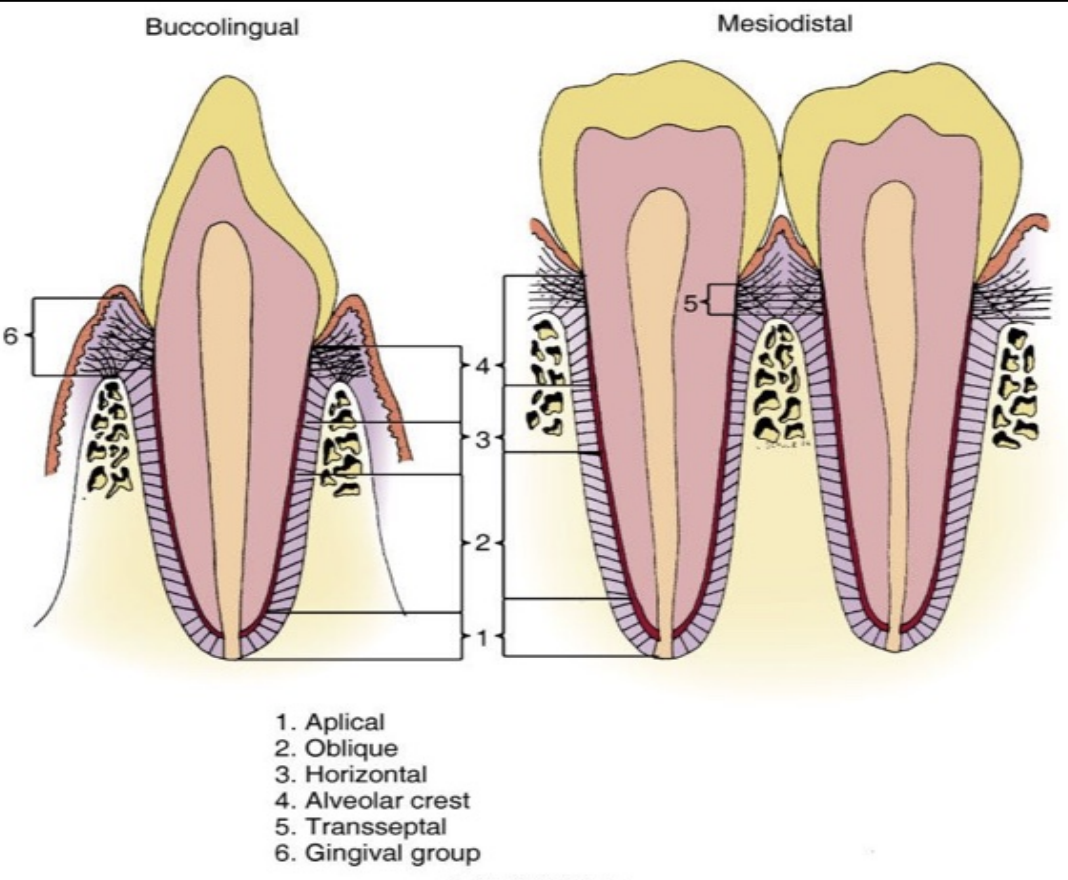
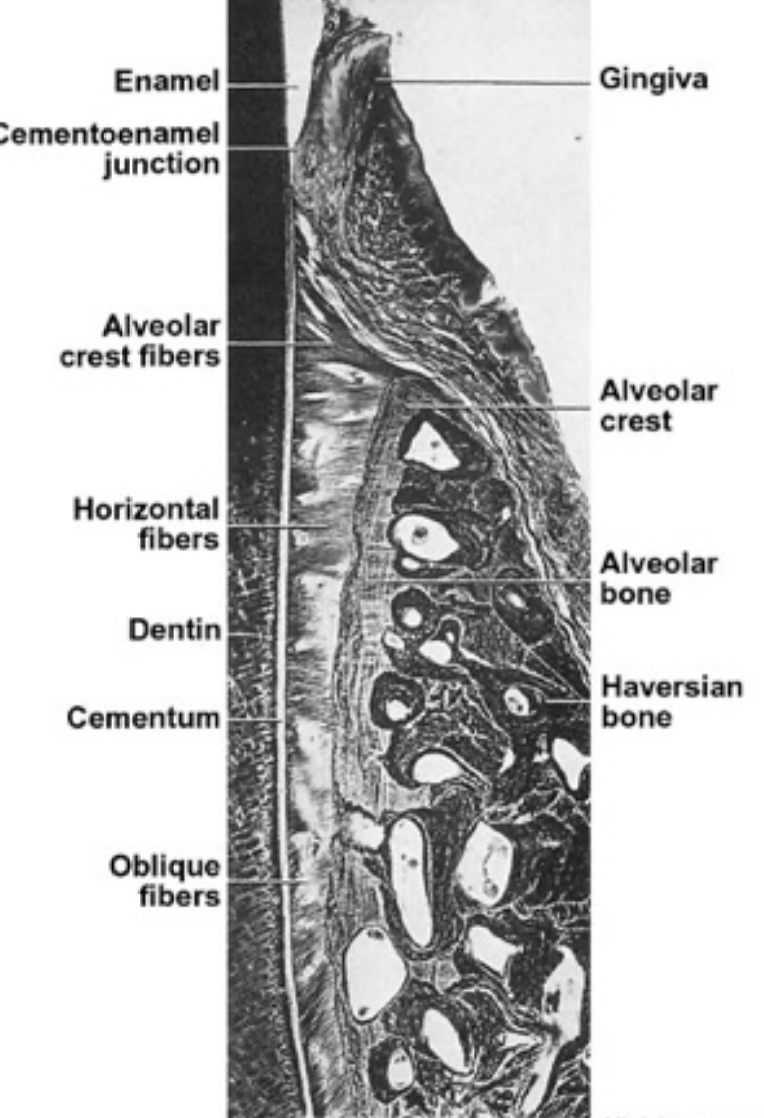
The functions of periodontium are:
Physical function: tooth attachment, support and protection, and shock absorber
Formative and remodeling: All the structures of the periodontium are continuously remodeled or newly formed throughout life.
Sensory: Receptor necessary for proper positioning of the jaw-proprioception rich
Nutritive: Blood vessels provide the essential nutrients of the vitality of the PDL.
The PDL gets its blood supply from the perforating arteries (from the cribriform plate of the bundle bone). The blood supply is rich because the PDL has a very high turnover rate.
The PDL gets its nerve supply from the inferior or the superior alveolar nerves, the fibers enter from the apical region and lateral socket walls.
Permanent Dentition- Anterior Teeth
First tooth from the midline is the maxillary permanent central incisor.
The maxillary permanent central incisor has the longest and widest anterior tooth, the root is broad and tapers in the apical third and short compared to all incisors.
Location in the arch: One on each side of the midline
Universal Number: R#8 - L#9
Eruption date: 7-8 years
Crown completion: 4-5 years
Antagonists: Mandibular central incisor and lateral incisor
Identifying features: Widest anterior tooth mesio-distally and straight incisal edges
Maxillary permanent lateral incisor has rounded incisal angles with the distal angle more convex, and is beside the central incisors.
Location in the arch: Distal to the central incisor, second tooth from the midline
Universal number: R#7 - L#10
Eruption date: 8-9
Crown completion: 4-5 years
Antagonists: Mandibular lateral incisor and canine
Identifying feature: Resembles maxillary central incisor but is smaller
Clinical considerations: May appear pointed (PEG shaped)
Canines are referred as the cornerstone of the dental arch, and are the longest teeth in the mouth (longest root)
Location in the arch: distal to lateral incisor and third tooth from the midline
Universal numbering: R#6 L#11
Eruption date: 11-12 Years old
Crown completion: 6-7 Years old
Antagonists: Mandibular canine and premolar
Idenifying feature: Longest maxillary tooth and Sharp pointed cusp
Clinical considerations: If premoalrs erupt first there will be no room for the maxillary canines to align properly.
Ugly duckling stage: from 9-11 years old, The mal-alignment of anterior teeth corrected by the eruption of the canines
Mandibular central incisors are the smallest teeth of the permanent dentition and the most symmetrical.
Location in the arch: One of each sides of the midline
Universal numbering: R#25 - L#24
Eruption date: 6-7 years old
Crown completion: 4-5 years old
Antagonists: Maxillary central incisor
Identifying feature: Smallest tooth in the oral cavity and only one antagonist
Mandibular lateral incisor is slightly larger than the mandibular central incisor in all dimensions but otherwise similar.
Location in the arch: distal to the central incisor, second tooth from the midline
Universal numbering: R#26 - L#23
Eruption date: 7-8 Years old
Crown Completion: 4-5 Years old
Antagonists: Maxillary central and lateral incisors
Identifying feature: Slightly larger than the mandibular central incisors, crown distally displaced.
Mandibular canine usually erupts before the maxillary canines and after most of the incisors have already erupted
Location in the arch: Distal to mandibular lateral incisor, 3d tooth from midline
Universal numbering: R#27 - L#22
Eruption date: 9 - 10 Years old
Crown completion: 6 - 7 years old
Antagonists: Maxillary lateral incisor and canine
Identifying feature: longest mandibular tooth, and narrower and smoother than maxillary canine.
Permanent Dentition- Posterior Teeth- Molars
The name molar comes from the latin word for “grinding” , there are 3 types of molars: the first molar, second molar, and third molar.
Upper first molar is the largest tooth in the maxillary arch, the cusp of carabelli is found on the mesio-lingual cusp.
Location in the arch: 6th tooth away from the midline, distal to the pre-molar
Universal number: R#3 - L#14
Eruption date: 6 - 7 years old
Crown completion: 2 ½ - 3 years old
Antagonists: Mandibular first and second molar
Identifying feature: 5 cusps , 3 roots
Maxillary right second molar is similar to the Maxillary first molar but one of the main differences is the distal cusps are smaller and less developed and no evidence of fifth cusp.
Location in the arch: 7th tooth away from midline, distal to the maxillary first molar
Universal numbering: R#2 - L#15
Eruption Date: 12 -13 years old
Crown completion: 7 - 8 years old
Antagonists: Mandibular second and third molar
Identifying feature: 4 cusps, and 3 pulp canals (1 in each root)
Maxillary third molars often appear as developmental anomaly, they vary considerably in size, contour and relative position to the other teeth.
Location in the arch: 8th tooth from the midline, distal to second molar
Universal number: R#1 - L#16
Eruption date: 17 - 21 Years old
Crown completion: 12 - 16 years old
Antagonists: Mandibular third molar
Identifying feature: fused roots, crown often heart shaped.
Clinical considerations: Third moalrs may fail to erupt causing them to be stuck in the alveolar bone.
Mandibular first molar have five cusps present and all of them are functional.
Location in the arch: 6th tooth away from the midline, distal from the second pre molar
Universal number: R#30 - L#19
Eruption date: 6 - 7 years
Crown completion: 2 ½ - 3 years
Antagonists: Maxillary second pre molar and first molar
Identifying features: 5 functional cusps, and 2 roots
Mandibular second molar have four cusps present, and the crown is smaller than of 1st molar.
Location at the arch: 7th tooth away from the midline, distal to the 1st molar
Universal number: R#31 - L#18
Eruption date: 11 - 13 years old
Crown completion: 7 - 8 years old
Antagonists: Maxillary first and second molars
Identifying features: 4 cusps , 2 pulp canals (one for each root)
Mandibular third molar is quite similar to the second molar, when it is normally developed
Location in the arch: 8th tooth from the midline, distal to the mandibular second molar.
Universal number: R#32 - L#17
Eruption date: 17 - 21 years old
Crown completion: 12 - 16 years old
Antagonists: Maxillary second and third molars
Identifying feature: Often has fused roots, when well developed looks like first or second molar.
Lab manual
Bud stage of tooth development