Human development !!
Sperm pathway…
Vagina → cervix → oviduct → secondary oocyte
Most sperm do not make it to fertilization –> why there are so many
Gravity, Acidic vaginal environment, Inability to get through the cervix, Destruction by uterine phagocytes, Choosing the wrong uterine tube
Secondary Oocyte – ovulated egg
Produced after 1st meiotic division of primary oocyte
Zona pellucida = extracellular matrix made of glycoprotein, it is attached to the plasma membrane of egg cell.
Corona radiata = a collection of remaining follicles cells surrounding the zona pellucida
2 processes MUST occur before fertilization!!!
1. Capacitation = breaking apart parts of the sperm, external layers of the membrane such as proteins on the surface of the sperm, done by enzymes in female reproductive tract, sperm can swim with more force but dies fast.
2. Acrosome reaction = Occurs when the sperm encounters the egg, allows it access inside through the release of acrosome enzymes.
Fertilization
In order for fertilization to occur sperm must migrate through the corona radiata before reaching the zona pellucida where the sperm cell will bind itself. This induces the acrosome to release digestive enzymes which enable the sperm to penetrate the zona pellucida and bind to the eggs plasma membrane.
→ sperm enters the egg and the egg completes meiosis 2
→ sperm ejects its nucleus and fuses with the eggs nucleus following the completion of meiosis 2 (of the egg cell) = zygote!
Polyspermy prevention
depends on changes in the eggs plasma membrane and in the zona pellucida
when sperm touches the eggs plasma membrane = instantly oocyte activation
prevented by chemical factors which are released (exocytosis) from the egg making the zona pellucida impenetrable to other sperm.
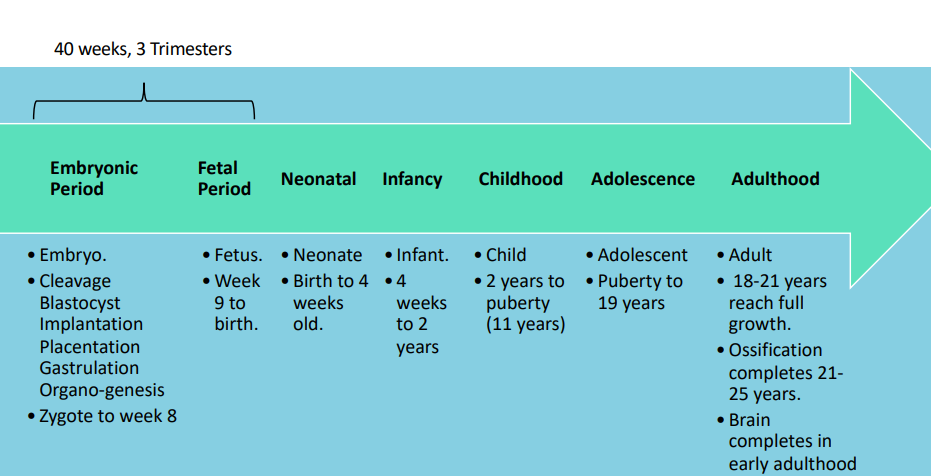
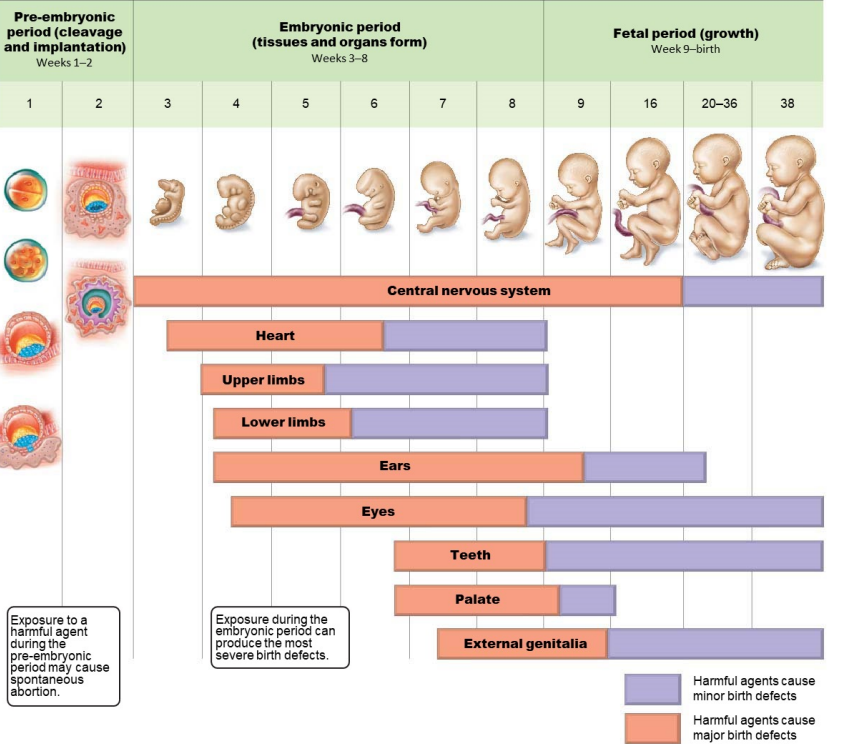
Embryo | Fetus |
- 8 weeks - immediately forms after fertilization, as a zygote - Basic structures/organ systems begin to form | - Weeks 9-40 - Later stages of development - Fetus has formed most of its essential structures and now focuses on growth + maturation |
STAGES OF EMBRYONIC DEVELOPMENT!!
cleavage - mitotic division (no size increase, cells get smaller with every division)
growth - increase in size
differentiation - cells specialize in structure/function
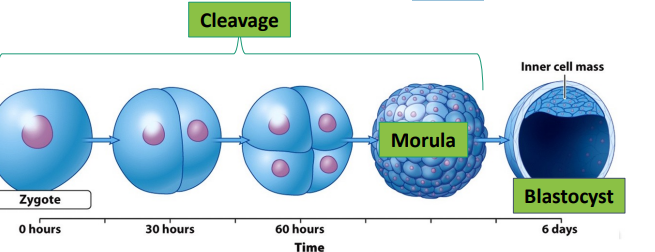
Week 1
Cleavage
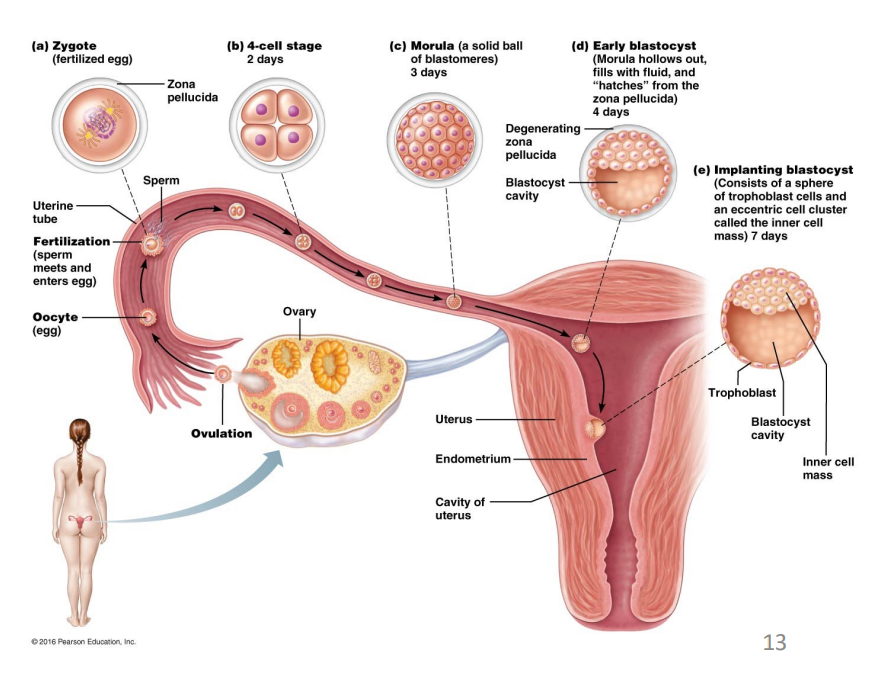
zygote is undergoing rapid mitotic cell division without increasing in size, after 3 days when embryo reaches 100 cells it is called the morula.
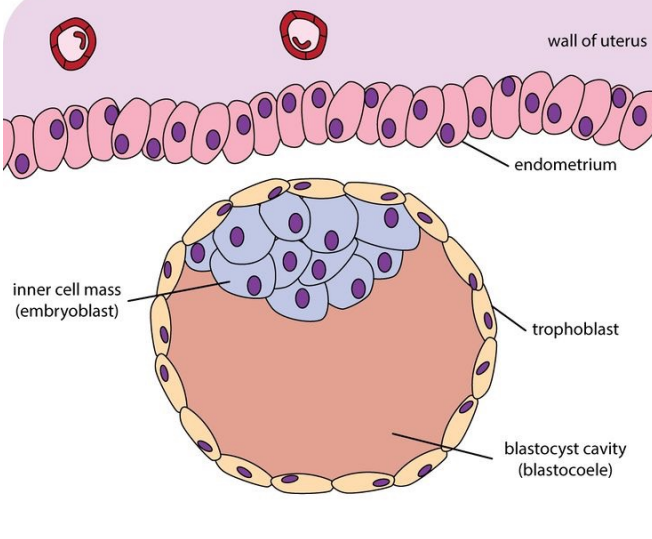
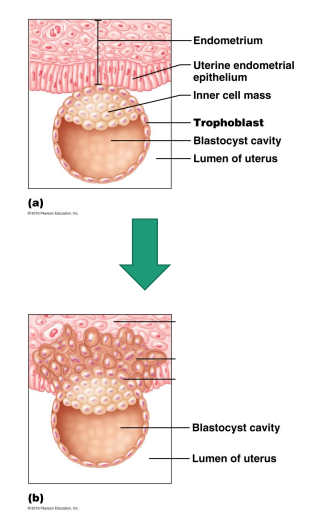
Following this by around day 4, the embryo reaches the blastocyst stage (ready for implantation and approaching uterus) characterized by the formation of a fluid-filled cavity. Some cells gather into an inner cell mass, which will later develop into the embryo, while others form an outer layer called the trophoblast, which will contribute to the placenta. This entire structure remains enclosed by the zona pellucida.
this all occurs as the embryo is travelling through the oviduct to uterus.
trophoblast cells will be involved in the process of implantation.
the inner cell mass is what will develop into the embryo, they are pluripotent stem cells having the capacity to differentiate into any specialized cell type found in the human body.
Twins!
Dizygotic (fraternal twins)
mother ovulated 2 eggs at the same time and both were fertilized
Monozygotic twin (identical)
if two inner cell masses are formed in the blastocyst instead of one inner cell mass.
Week 2
7 days post fertilization implantation occurs and takes 5 days to complete.
trophoblasts produce human chorionic gonadotropin (hCG) to maintain the corpus luteum and promote placental formation.
increasing levels of estrogen and progesterone from the corpus luteum work to thicken the endometrium for implantation.
trophoblast binds to the extracellular matrix of the endometrial cells and releases digestive enzymes to help with implantation.
Note: at this stage embryo is nourished by endometrial cells!!
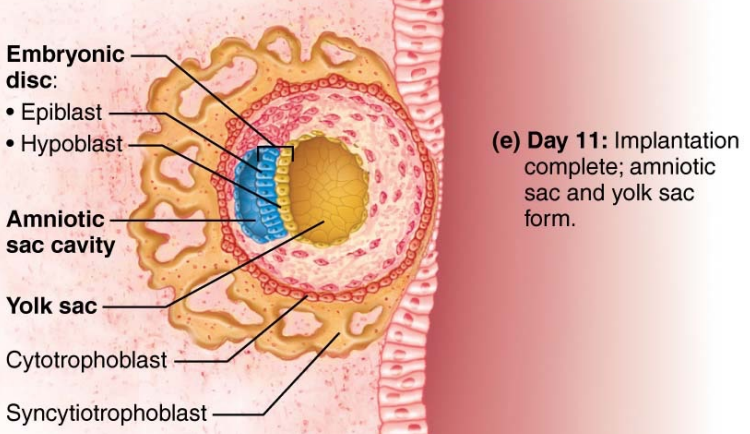
trophoblast will divide into two layers which form the outermost layers of chorion…
inner = cytotrophoblast
outer = syncytiotrophoblast - forms one big multinucleated mass that invades the endometrium and it is sealed off by new endometrial cells
Inner mass cells will become the two layers of the embryonic disc → will form the embryo and the four layers of the extraembryonic membrane (directly or through intermediate structures)
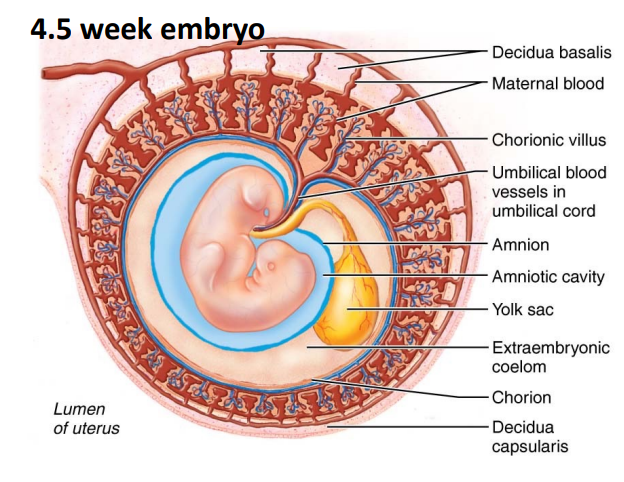
some cells during this stage will begin to differentiate into two of the four extra-embryonic membranes…
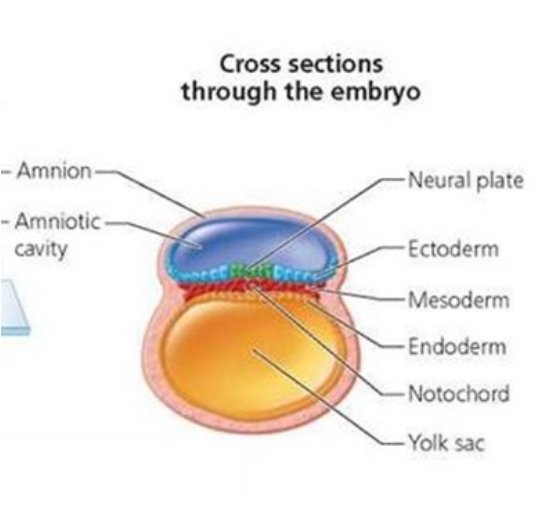
Amnion = sac filled with fluid surrounding the embryo
yolk sac = nutrient supply
Allantois = excretory duct, will develop into blader
Chorion = innermost layer (w3) outermost (w2)!!→ the embryonic portion of the placenta
the last two develop later in week 3!!
Week 3
first embryonic cells are all stem cells → unspecialized, can divide infinitely, described as totipotent (they have the potential to develop into any cell ex; morula)
under specific chemical signals stem cells become pluripotent → no longer support differentiation into any cell type ex; blastocyst
then they become multipotent stem cells and can differentiate into multiple but limited kinds of specialized cells.
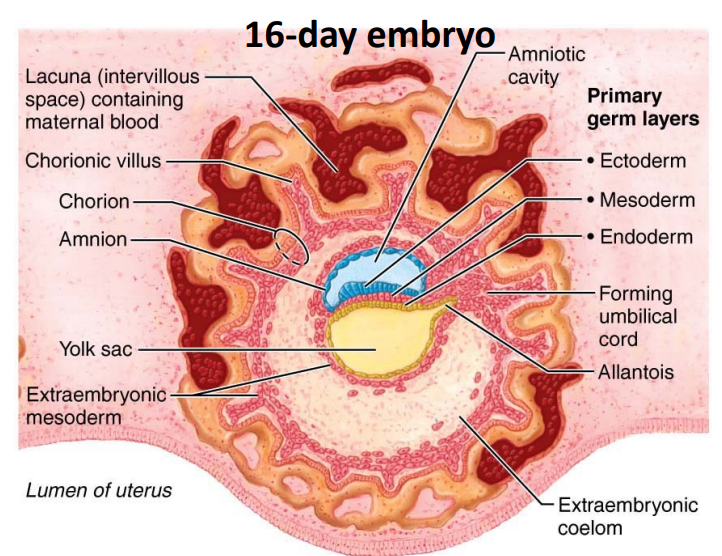
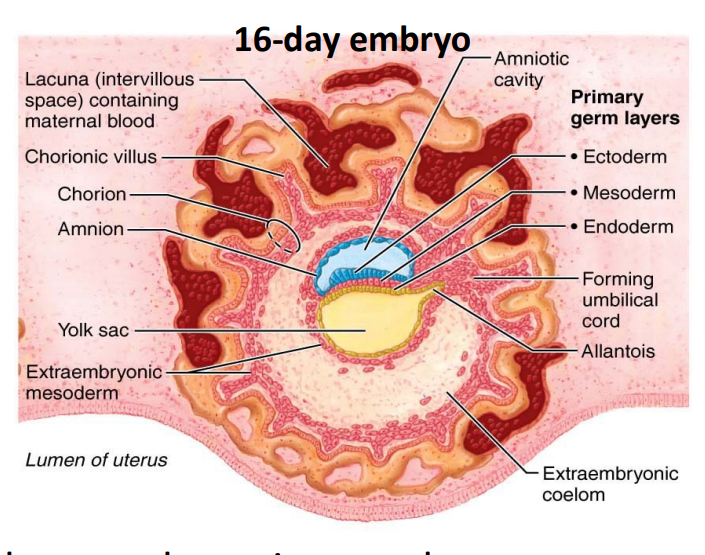
3rd week → two layered embryonic disc becomes a three layered gastrula through the process of gastrulation (cells transition from pluripotency to multipotency)
thee three layers of the gastrula include…
Endoderm → forms digestive and respiratory systems, anterior pituitary gland, thyroid, parathyroid, thymus, pancreas (all produce water soluble hormones)
Mesoderm → forms muscle/connective tissue, kidneys, gonads, adrenal cortex (steroid hormone producers)
Ectoderm → forming skin and nervous tissue, posterior pituitary gland, adrenal medulla, pineal gland
the endocrine glands arise from all three embryonic germ layers.
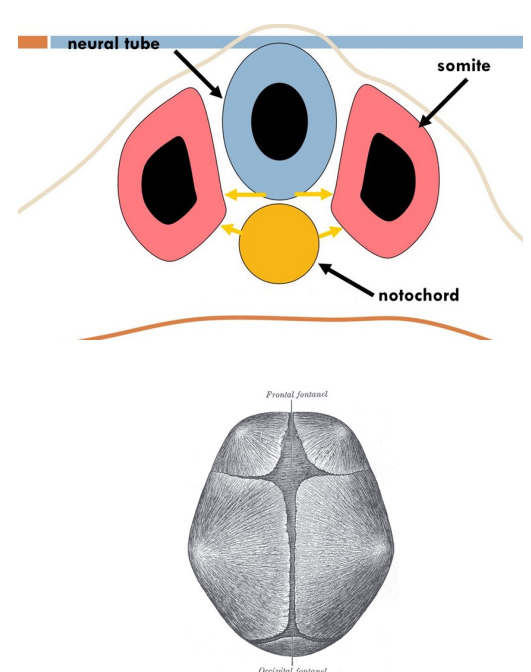
The notochord (mesoderm) will become the intervertebral discs.
forms central axis of the embryo, around it the axial skeleton will form.
Nervous system early formation
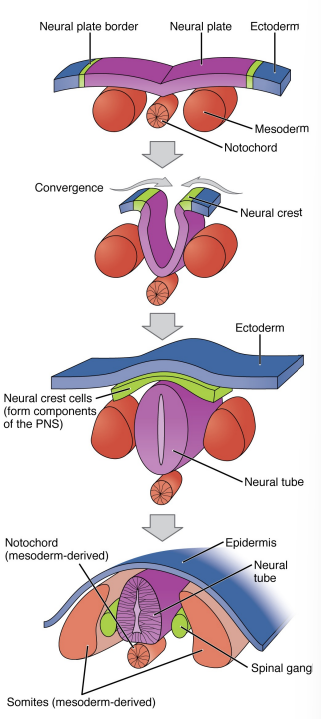
begins with a section of tissues from the ectoderm differentiating to form the neural plate (thickened region)
the neural plate starts to fold inwards which creates a groove called the neural fold, it appears as a visible line along the dorsal surface of the embryo.
as the neural fold comes together it forms the neural tube.
the anterior part of the neural tube will become the brain and the posterior portion will become the spinal cord.
additionally, the borders of the neural plate become the neural crest, and the ectoderm fuses to form the outer superficial layer.
neural crest develops into the peripheral structures (nerves).
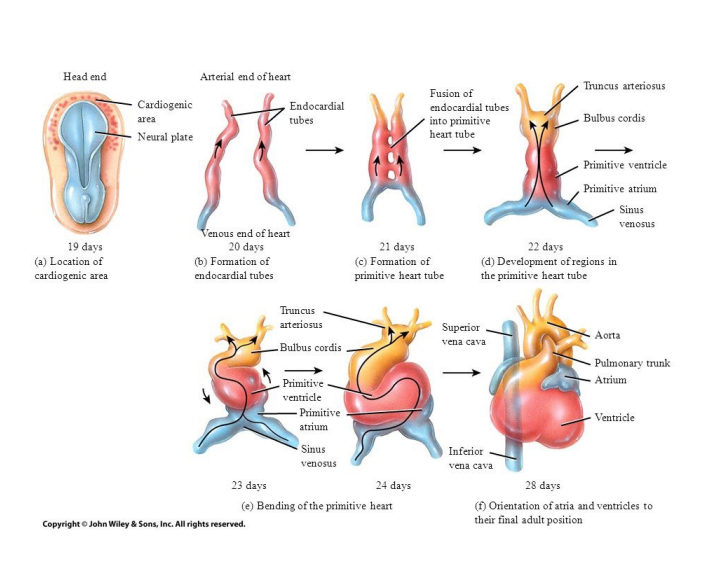
The heart → 1st functional organ to develop, begins pumping around day 21-22.
the heart bulge develops from mesoderm 18-19 days after fertilization in the cardiogenic area near the head of the embryo.
Heart formation…
two strands called cardiogenic cords form
they develop a lumen and will now be called endocardial tubes which will fuse to form a primitive heart tube
the primitive heart tube forms into 5 regions…
truncus arteriosus = pulmonary trunk and arteries
bulbus cordis = right ventricle
primitive ventricle = left ventricle
primitive atrium = right and left atria
sinus venosus = SA node and coronary sinus
→ initially, blood flows in a single circuit, end of week 5 chambers, septum, pulmonary and systemic circuits have developed. (valves complete development during 5-9)
Week 4
Beginning of week 4 embryo goes from flat shaped disc to a C-shaped embryo.
forms 4 folds = 2 lateral, a cranial and a caudal.
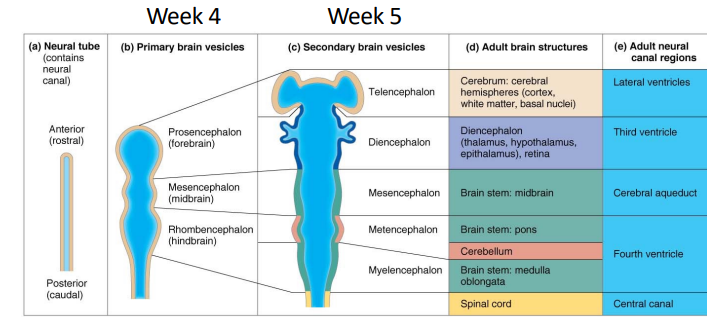
end of week 4 → more complex structures of brain begins development.
→ 3 enlargements called vesicles begin to form…
prosencephalon = forebrain (in adults → cerebrum and diencephalon =, eyes also develop from this)
mesencephalon = midbrain
rhombencephalon = hindbrain (in adults → pons, medulla oblangata, cerebellum)
Note = spinal cord does not differ from its basic layout of the neural tube.
ventricles are remnants of the hollow center of the neural tube
Skeletal system development…
first, mesoderm tissue on either side of the notochord thickens and separates into block-like tissue called somite’s.
the medial portion of this somite called the sclerotome is composed of mesenchyme which develops into the fibrous connective tissues, cartilages, and bones.
bones of the skull arise from mesenchyme, first the top and sides of the brain case through intramembranous ossification (bone formation where bone develops directly from mesenchymal tissue without first forming cartilage)
brain grows within brain case and the bones move further apart, dense connective tissue called fontanelles connect each brain case bone (disappear by age 2)
other bones (except clavicle) develop through endochondral ossification (slow process which forms a cartilage framework first)
Limbs develop at the end of week 4, upper limbs appear first a few days before lower.
note = limbs start off as small bulges called limb buds and they develop along the proximal to distal axis.
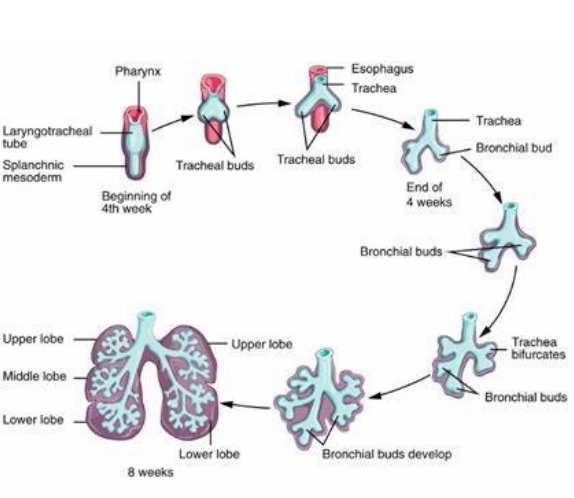
respiratory system development…
begins during week 4, functional by week 28, only full developed in early childhood, 8yrs.
→ ectoderm tissue from the head invaginates to form olfactory pits which will become the nasal cavity.
→ a lung bud forms from a bulge of endoderm tissue in the foregut during the beginning of week 4, starts to branch after
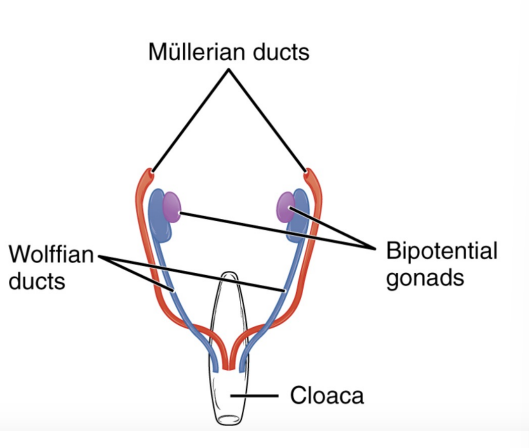
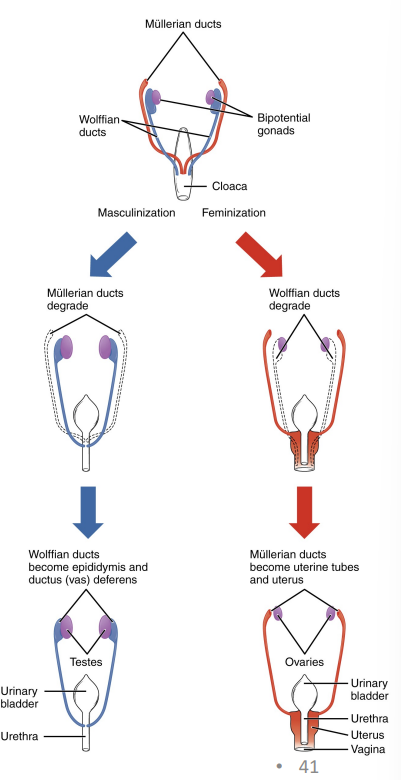
Gonad development…
begins during week 4, sexual differentiation does not begin until fetal period (9-12)
some tissue are bipotential → depending on the chemical signals they can develop into male/female structures during development (gonads, glans penis vs clitoris).
other tissues have both male and female structures → the female tract is the mullerian duct (uterus, oviducts, vagina) male tract is the wolffian duct (epididymis, vas deferens, seminal vesicles).
Placenta
begins to develop after implantation through placentation and is complete by weeks 14-16
made of embyonic and maternal tissues
between prenatal weeks 4-12 developing placenta gradually takes over the role of feeding the embryo (rather than the endometrium).
Decidua basalis = deepest portion of endometrium, forms the maternal portion of the placenta. maternal blood will enter the lacuna surrounding the embryonic portion of the placenta.
the chorion forms the embryonic portion of the placenta.
during week 3 the chorion forms finger-like structures called the chorionic villi which burrow into the endometrium.
during week 4 fetal mesenchymal cells from the mesoderm form fetal capillaries in the chorionic villi, including umbillical vessels
umbilical arteries 2 → bring oxygen poor blood and waste from fetus to placenta
umbilical veins 1 → nutrients and oxygen carried from mother to the fetus
hCG levels increase very rapidly from trophoblast cells to maintain the corpus luteum for the first 8 weeks. hCG then drops off as the developing placenta takes over the role of producing estrogen and progesterone.
The corpus luteum regresses and the ovaries remain dormant due to still elevated estrogen and progesterone levels.
Week 5-8
week 5 → development of the eye, limb buds, lymphatic and digestive system begins during this week.
week 6 → distal ends of the limb buds will expand and flatten into the hand or foot, wrist and elbow development will follow.
limb bud continues growing → endochondral ossification of the limb bones occurs within, synovial joints form between adjacent cartilage. '
fetal limb movements begins!
weeks 7-8
lateral rotation of 90 degrees to position the palm of the hand anteriorly and a medial rotation of 90 degrees to position the big toe to the medial side of the foot.
more complex facial structures are forming
8 week US! → used to check placental growth, # embryos, position of embryo, heart beats.
CRL → excludes the yolk sac and extremities
used to measure gestational age between 6-13 weeks
after 13 weeks, head circumference, biparietal diameter, and femur length measurements become more useful measurements for assessing fetal growth.
weeks 9-12
weeks 9-10
head is larger, ½ CRL, body elongates and ossification continues. bone marrow takes over from the liver for erythropoiesis, bile is being secreted by liver now
face will now be broad, eyes are widely separated, ears are low set, eyelids are fused.
fetus swallows amniotic fluid and produces urine
fingers and toes develop nails
week 11
intestinal coils visible near the proximal end of the umbilical cord outside of the fetus during the beginning of the fetal development (body too small) but eventually will be moving into abdominal cavity where they belong.
week 12
cartilage skeleton continues the ossification process to turn into bone
sexual differentiation is visible
reproductive system development…
Male → sex determining region on the Y chromosome promotes the development of bipotential gonads into testes and suppresses the genes for female development.
once testes are formed = leydig cells will produce testosterone → influences the development of the other male reproductive structures.
proper hormonal signals will cause mullerian duct to degrade and the wolffian duct system will develop (vice versa for females)
bipotential genital tubercle becomes glans penis or clitoris
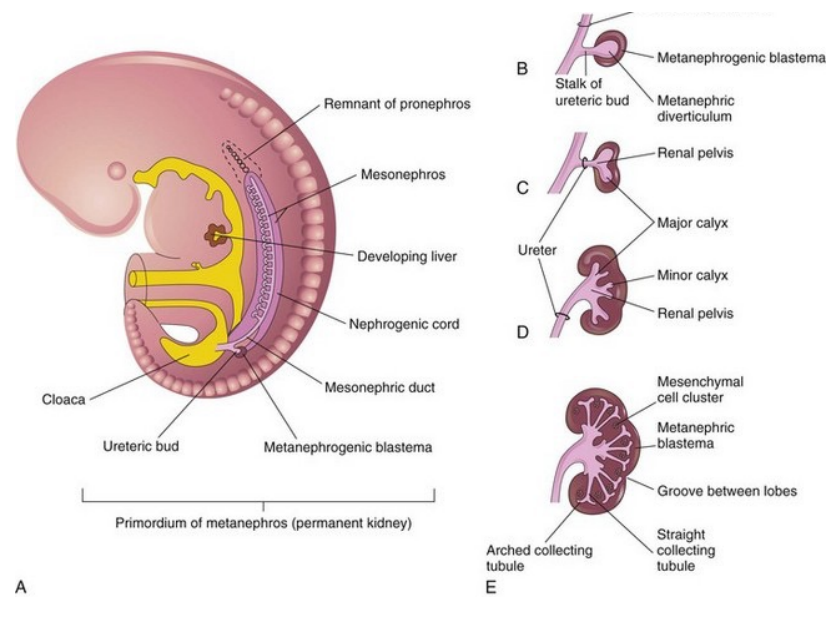
→ urinary system develops from the genital system
1st trimester US…
First trimester ultrasounds will be able to locate the longitudinal fissure, falx cerebri (dura mater in longitudinal fissure), ventricles, cerebrum, diencephalon, brainstem, cerebellum, and fornix (structures of the limbic system).
!!end of 1st trimester!!
weeks 13-16
beginning of 2nd trimester
→ sensory organs are developing, blinking begins, ears are close to their definite positions, lips produce sucking motions.
scalp grows hair, urinary system forms, meconium (fecal feces) accumulate in intestines.
rapid growth along with more coordinated limb movements
in female fetuses, ovaries contain primordial ovarian follicles which contain oogonia.
weeks 17-20 & 21-30
17-20…
during this period growth slows, limb movements are more powerful (felt)
bronchioles form, vascularization, and formation of alveoli takes place
formation of brown fat is specialized adipose tissue which enables heat production (neck, sternum, perirenal)
sebaceous glands coat the skin with vernix caseosa (wax like substance to protect skin and provide lubricant during birth)
silk hair called lanugo covers skin
21-30
rapid weight gain, wrinkled skin
axons become myelinated (not complete until adolescence)
eyelashes develop, eyelids are no longer fused, rapid eye movement.
lungs produce surfactant and breathing movements occur
testes descend into the scrotum for males
2nd trimester US!
The second trimester spans weeks 13 to the end of week 27.
Fetal skull and brain development, face, heart anatomy, heart rate, major blood vessels, diaphragm and lungs, abdominal organs, muscular and skeletal anatomy, placenta, umbilical cord.
The nuchal fold is a normal fold of skin seen at the back of the fetal neck during the second trimester of pregnancy. Increased thickness of the nuchal fold is a soft marker associated with multiple fetal anomalies, such as Trisomy 21.
The cavum septum pellucidum is a slit-like fluid-filled space in the septum pellucidum (membrane separating the anterior horns of the lateral ventricles), it is present in fetuses but is often fused in adults. enlargement can be associated with neurological abnormalities
Weeks 31-birth
white fat increases from 8% at early development to 16% at birth, important for energy storage and insulation after birth
lanugo is shed!! skin is pink and smooth
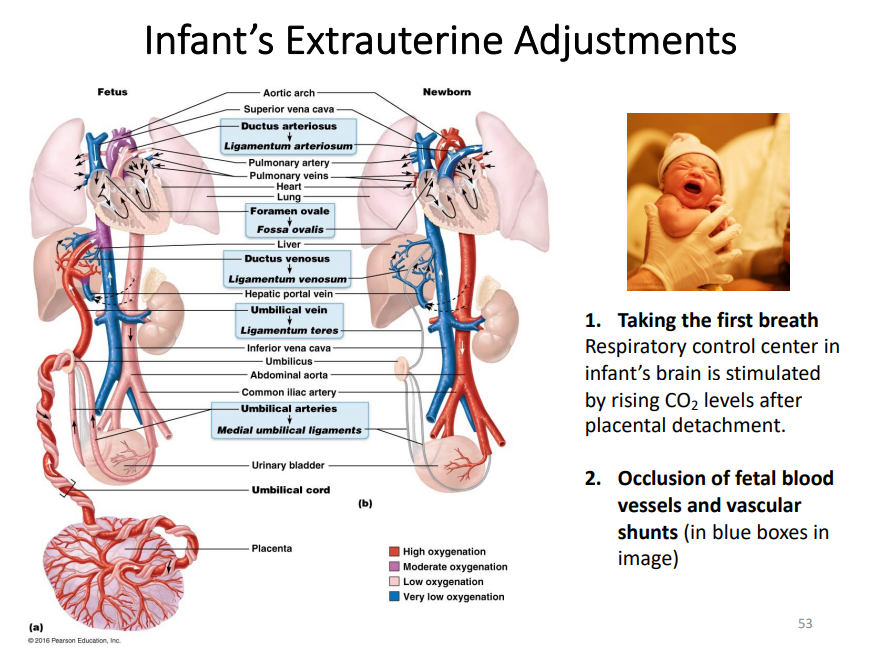
umbilical vein
function = carries oxygenated blood from placenta→ fetus
post-birth = becomes the ligamentum teres (round ligament of the hip)
umbilical arteries
function = carries deoxygenated blood from fetus → placenta
post-birth: becomes the medial umbilical ligaments
Foramen Ovale
a small opening between righ and left atria
allows for blood to bypass the lungs (non functional in utero) by shunting blood from the right atrium to the left atrium
closes and forms the fossa ovalis in the interatrial septum after birth.
ductus arteriosus
a vessel connecting the pulmonary artery to the aorta
shunts blood away from lungs and directs it into the systemic circulation
closes and becomes the ligamentum arteriosum
ductus venosus
vessel connecting the pulmonary artery to aorta
bypasses the liver to deliver oxygenated blood to fetal heart
closes and becomes the ligamentum venosum
The mother
Anatomical changes
organ crowding
relaxation of pelvic ligaments & pubic symphysis due to production of hormone relaxin by the placenta
breast enlargment and engorge with blood, dark areolas
Metabolic changes
Physiological changes
gastrointestinal system
morning sickness due to hormone fluctuation
acid reflex → overcrowded organs
constipation → declining motility of GI tract
urinary system
frequent urination due to burden
uterus compressing bladder
respiratory system
Nasal mucosa becomes congested & swollen (effect of estrogen)
Tidal volume increases initially
Dyspnea (difficult breathing) occurs during later stages of pregnancy as baby puts pressure on diaphragm.
cardiovascular system
Blood volume increases up to 40%
Cardiac output increases
Edema and varicose veins in legs are common due to increased pressure from the uterus on pelvic blood vessels
Labour & delivery
Maturing fetal lungs produce surfactant protein A which softens the cervix of the mother. In the last weeks of pregnancy, the placenta increases the amount of estrogen levels in the body.
High levels of estrogen stimulates myometrial cells to form and insert oxytocin receptors in their membranes.
When oxytocin binds to receptors it causes contractions of the uterine wall initiating softening (effacement) and dilation of the cervix (labour) and pushes baby out (delivery).
Sustained contractions occurring at regular intervals until after baby is birthed.