mood disorders.docx
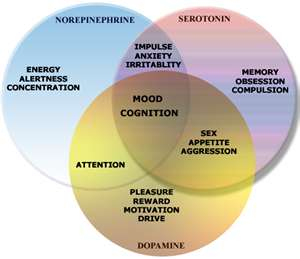
- FYI: 5HT is short hand for serotonin
- Define Mood
- Examine differences between major depressive disorder and Bipolar Disorder
- Review across the lifespan situations that can be associated with mood disorders.
- Discuss assessments, behaviors and risks associated with these two disorders
- Review treatment options for each disorder
- Analyze side effects of each class of medications
- Highlight priority nursing interventions to include teaching with medications.
Types of Disorders
Mood
- a prolonged emotional state; it impacts our personal life and personality
- flat affect= withdrawn
- mood changes are normal and expected, it becomes a mood disorder when it interfers with normal activities; static mood or pronounced change that interferes.
Depression/Major depressive disorder
- Patho:
- Often dysregulation of NE, DA, 5HT
- At risk for depression
- Across the lifespan, gender, social economic
- Young people after starting medications can have more risk of SI, follow up and ask questions. Black box warning on psych meds
- Family history, genetic component
- Children with adverse childhood events
- Across the lifespan, gender, social economic
- At risk for suicide
- Adolescents
- children of color are at higher risk then other of same age due access to guns
- peer pressure; bullying; hormone changes; poor coping skills
- adverse childhood event
- Elderly- poor health and lose their support
- Recent crisis, stress, loss
- Substance use
- No social support
- Chronic or painful illness
- Previous suicide attempt
- Identity crisis
- Withdrawn, depressed
- Hallucinating (this would be the very severe depression that become psychotic = lose touch with reality)
- Adolescents
- Assessment:
- Take a history: self, family
- Blood work to rule out other possible causes
- Children will present BORED or IRRITABLE
- Cognitive
- Suicidal Ideation
- Crying
- Poverty of ideas
- Negative view: self, world, future
- Mood
- Dysphoric
- Depressive
- Despair
- ↓ interest in pleasure (anhedonia)
- Psychomotor
- Agitation of retardation of movement
- Fatigue
- ↓ appetite
- Constipation
- Sleep disturbance
- ↓ libido
- “SIG E CAPS”
- Sleep disturbance
- Interest decrease
- Guilty feeling
- Energy decrease
- Concentration decrease
- Appetite ↑ or ↓
- Psychomotor fxn ↓
- Suicidal ideations
- Postpartum depression
- Depression across the lifespan- due to hormonal changes
- Can be severe = postpartum psychosis; having paranoid thoughts/seeing things not there
- Screen mothers
- Nursing diagnosis
- Ineffective individual coping
- Impaired social interaction or social isolation
- Risk for self harm
- Low self esteem
- Treatment:
- Intervention
- Participation in group, hobbies= ↑ self esteem; improve with endorphins
- Promote expression of feelings
- Safety precautions
- Remove harmful objects
- Close observation 1:1
- Written contract
- Physical needs
- Access weight
- Ask about appetite and what eating
- Prevent side effects meds: example constipation in TCA
- Electroconvulsive therapy
- Not first line; used if need urgent response or failed other tx
- Controlled seizures to “reset the brain”
- Informed consent needed
- IV set up, check Vital signs, give anticholinergic meds to dry secretions so do not aspirate, emergency air way ready to go; preoxygenation; atropine to prevent bradycardia; conscious sedation propofol;
- monitor after tired, headache, confusion will go away
- Intervention
- Pharmacology
- SSRI
- Zoloft® (sertraline), Paxil® (paroxetine), Prozac® (fluoxetine)
- Key teaching: take few weeks to have effect 4 – 6 weeks
- D/D: st. john’s wort, MAO, Zofran = 5HT syndrome
- 5HT 🡪
- hold med; inform MD;
- protect airway, breathing, circulation
- Cooling blanket for fever
- Seizures – antiepileptic
- 5HT 🡪
- TCA
- Elavil ® (Amitriptyline); Tofranil ® (imipramine); Pamelor ® (nortriptyline); Sinequan ® (doxepin)
- Watch for
- Anticholinergic side effects: sedation, orthostatic hypotension, dry mouth, urinary retention, tachycardia
- Not 1st choice for elderly due to Orthostatic hypotension
- MAOIs
- Nardil ® (phenelzine) , Parnate ® (tranylcypromine) Marplan ® (isocarboxazid), selegiline
- SE: sweating,tremors, elevated temp, bounding heart, ↑ BP
- Avoid tyramine foods
- NO aged or fermented cheese, wine
- Cured meats, smoked meats, processed meats
- Pickled or fermented foods
- Sauces (soy, miso, teriyaki)
- Avoid medications that affect 5HT
- NO barbiturates, antihistamines, TCA, OTC cold meds, CNS depressants
- SNRI
- Cymbalta ® (Duloxextine), Effexor® (venlafaxine)
- NE and 5HT
- Check Blood pressure b/c can lower
- NDRI
- Wellbutrin ® (bupropinon):
- DA and NE used for smoking cessation and depression; do help with sleep; at night
- Remeron ® (mirtazapine)
- DA and NE; effect with insomnia
- Used normally only when others uneffective
- Do not use seizures or eating disorders; due to lower seizure threshold
- Wellbutrin ® (bupropinon):
- Atypical
- Desyrel® (trazodone): used for insomnia take at night
- SSRI
Bipolar Disorder ( aka Manic-depressive disorder)
- Patho
- Mania = an alteration in the mood when the person feels elated , has big self esteem, hyperactive.
- There are different types, but not tested on hypomania, delirum mania
- Must have at least one manic episode to be considered Bipolar, can spend more time in either polar state (depression/mania)
- Mania = an alteration in the mood when the person feels elated , has big self esteem, hyperactive.
- Risk for suicide is higher in mania
- Delirious/ unstable
- Reckless behavior
- Unintentionally harm themselves and others
- Symptoms
- Manic
- Patients may like this state b/c they are productive, can start slow and ramp up. They can like these feelings and then not take meds b/c of.
- Onset before 30 yo; begins suddenly and escalates over several days
- Mood
- Elevated, expansive, irritable
- Speech
- Loud-rapid, punning, rhyming, clanging, vulgar
- Flight of ideas
- Weight loss: to active for eating and don’t sit still
- Grandiose delusions: May think they are Michelle Obama or God
- Distracted, hyperactive, ↓ need for sleep
- Depressive
- Mood
- ↓ interest in pleasure
- Negative view
- Fatigue
- ↓ appetite, ↓labido,
- Constipation
- Insomnia
- Agitation or movement retardation
- Manic
- Assessments
- Treatment
- Same as depression; added problems with taking medications and during mania poor choices and risky behaviors
- SET BOUNDARIES
- Professional relationship
- Family education
- Manic state: decrease stimulated environement
- Pharmacology
- Mania
- Anticonvulsants used mood stabilizers
- Valproic acid: with meals and therapeutic levels
- Depakote ® (divalproex)
- Lamictal ® (Lamotrigine): steven johnson syndrome; if rash need to follow up
- Eskalith ® (Lithium)
- Read this Lexicomp
- Use: treat mania
- MOA: related to sodium, effects the sodium ion transport into the nerve and enhances the reuptake of NE and 5HT in the brain therefore decreasing hyperactivity.
- SE:
- Weight gain, n/v, diarrhea, polydipsia, tremor, polyuria, metallic taste in mouth
- Chronic toxicity can lead to endocrine system: hypothyroid, hyperthyroid
- Toxicity:
- Anticonvulsants used mood stabilizers
- Mania
What leads to dehydration, too much drug, issues with renal and excretion
Mild >1.5- 2.0 mEq/L
n/v, diarrhea, abdominal pain, blurred vision
Moderate 2-3
GI: N/V, diarrhea
Neuro:
Mental status changes dysarthria (slurred speech) ataxia ( balance/coordination); confusion, tremors, hyperreflexia, hystagmus, myoclonus ( muscle twitches)
Increased urine output
Seizure, coma
Severe >3 mEg/L
Seizures, coma
May need hemodialysis to survive
- D/D:
- avoid diuretics if possible
- 5HT syndrome drugs
- Nursing:
- Baseline EKG
- Baseline chemistry and maintance labs; includes sodium
- Know the toxicity sx and therapeutics levels
- Blood work/ baseline
- D/D:
Draw am before med given
1 -2 mn checked in beginning weekly;
Therapeutic 0.5 to 1.5 mEq/L
Maintenance 0.6 to 1.2 mEq/L:
- Fluids = 3 L
- Baseline renal test, cardiac, thyroid (can lead to hypothyroid)
- Tx of toxicity:
- Teaching:
- Drink 3 L of fluid daily
- Blood will drawn to access levels
- Monitor salt, keep same because can change level of drug
- SX of n/v, diarrhea needs to be communicated to MD
- Nursing Actions
- Teaching be/c more at risk for suicide or harm during mania
- Be honest with patient
- Help set goals or remind of love ones that may be harmed by actions or behaviors
- Teach families of early signs of mania
- Mania can turn into psychotic episode and lose touch with reality
- Work with patient to have psychiatric advance directives
- Teaching be/c more at risk for suicide or harm during mania
Schizophrenia
- Patho
Suicide Precautions make room safe
- Secure Room
- Windows locked
- Breakproof glass & mirrors
- Plastic flatware
- No cords: phones, IV, extension cords
- No belts, curtains
- No matches or cigarettes
- No sharps/ razors
- No hand santitizer
- Patient care
- Frequently observe 1:1
- Staff communication
- Develop therapeutic relationship
- Written behavior contract with patient
- Restraints as ordered
- Medications as ordered
- Monitor and restrict visitors