(Week 2) Self-defense PP and lecture notes
Microbiome (AKA normal flora)
Compete with pathogens for nutrients.
Block pathogen epithelial attachment.
Produce toxins to inhibit pathogenic colonization.
Induce growth of lymphoid tissue.
Altered with prolonged broad-spectrum antibiotics.
Innate vs. Adaptive
Innate immunity has constant/immediate defense timing.
Adaptive immunity has initially delayed response, but immediate response when exposed again to same pathogen.
Inflammatory response
Diverse causes; nonspecific.
Act at site of cellular injury to:
Confine damage
Kill microorganisms
remove debris.
Can be painful and harm healthy tissue
Vasodilation
Increases vascular permeability and leakage
Increases WBC adherence to inner vessel walls and migration through vessel walls to injury site (Diapedesis).
Cardinal “signs” of inflammation
Redness, heat, swelling, pain, and dysfunction (local).
Fever, leukocytosis, plasma protein synthesis (systemic).
Plasma protein systems
Anaphylatoxin- is a peptide fragment that plays a crucial role in the inflammatory response by promoting vasodilation and increasing vascular permeability.
Opsonization- the process by which pathogens are marked for ingestion and destruction by phagocytes.
Chemotaxis- the movement of immune cells toward the site of infection or injury, driven by chemical signals released by pathogens or damaged tissues.
Fibrin- a fibrous protein involved in the clotting process that forms a mesh-like structure to stabilize the platelet plug during hemostasis.
Bradykinin
Histamine-like effects
Increased permeability
Vasodilation
Stimulates nerve endings which cause pain.
Inflammation: Systemic manifestations
Fever
Caused by exogenous (pathogen-produced) and endogenous (cytokines) pyrogens.
Endogenous pyrogens are IL-1, IL-6, TNF- a cytokines)
Act directly on hypothalamus.
Leukocytosis
Increased number of circulating leukocytes.
“Left shift” in ratio of immature to mature neutrophils.
Increased plasma protein synthesis
Acute-phase reactants (pro or anti inflammatory)
C-reactive protein (CRP), fibrinogen, complement components, etc.
Inflammatory mediators
Vasodilation
Prostaglandins
Histamine
Nitric oxide
Pain
Prostaglandins
Bradykinin
(Systemic effect) Fever
IL-1
IL-6
TNG-a
Prostaglandins
Limit inflammation
IL-10 (inhibits cytokine production)
TGF-B (inhibits macrophage proliferation)
ECF- A (Attracts eosinophils)
Histaminase, Arylsulfatase (Destroy histamine and leukotrienes)
Vascular permeability
Histamine
Bradykinin
Leukotrienes
PAF
Mast Cells
After activated due to activated complement, the mast cells degranulate. This release of mediators, including histamine and leukotrienes, contributes to increased vascular permeability and bronchoconstriction, playing a significant role in allergic reactions and asthma.
After eosinophils arrive, they activate and release histaminase which then destroys histamine and lowers inflammation.
Histamine receptors
Histamine 1 receptor- primarily mediates allergic reactions by causing vasodilation and increased permeability in blood vessels, leading to the typical symptoms such as redness, swelling, and itchiness. (INFLAMMATION).
Histamine 2 receptor- it stimulates gastric acid secretion from parietal cells in the stomach lining, which decreases WBCs activity. (ANTI-INFLAMMATORY).
Wound healing
Resolution (regeneration) vs. repair (scar tissue)
Fill → Seal → shrink
Coagulation, inflammation, proliferation, remodeling.
Tissue repair:
Fibrin clot
Proteinases/inhibitors
Structural proteins → matrix
Adhesion molecules
Growth factors
Adaptive immunity
Antigens
Non- self substances
Antibodies (immunoglobulins)
Specificity (lymphocyte receptor)
Memory
Lymphocytes
Phases
Clonal diversity- production of T and B cells with all possible receptors for antigen.
Clonal selection- Selection, proliferation, and differentiation of individual T and B cells with receptors for a specific antigen.
T cells are cell mediated immunity while B cells are humoral immunity
Primary & Secondary responses
IgG is the most dominant immunoglobulin.
IgM is the first one to appear when there’s an exposure to an antigen.
Active vs. Passive immunity
Active immunity
Antibodies or T cells produced after either natural exposure to antigen or immunization.
Long-lived
Passive immunity
Preformed antibodies or T lymphocytes transferred from donor to recipient (eg. placenta).
Short-lived.
Inappropriate immune reactions
Allergy- exaggerated immune response against exogenous environmental antigens (Hay fever).
Autoimmunity- immune response directed against “self” (Lupus).
Alloimmunity- immune response against beneficial foreign tissue (Transfusion reaction, transplant rejection).
Immune deficiency- response insufficient to protect host (AIDS).
Hypersensitivity
Altered immunologic response to antigen → damage to host.
Can be immediate or delayed.
Hypersensitivity reactions:
Anaphylaxis (Bee sting, penicillin allergy, shellfish, peanuts)
Most rapid and severe, immediate
Systemic vs. localized
Treatment: Epinephrine (systemic). Epinephrine vasoconstricts the blood vessels and dilatates the lungs so counteract the bronchospasm.
Histamine release
Histamine 1 (smooth muscle contraction → bronchospasm) & Histamine 2 (Increase in gastric acid secretion, decrease in histamine release from mast cell) Receptors.
Hypersensitivity Type I
IgE mediated
Mast cells
Against environmental antigens (allergens).
Ex. Hay fever, food allergies.
S/S: itching, urticaria, conjunctivitis, rhinitis, GI cramps or malabsorption, vasodilation/edema, bronchospasm.
Treatment: Antihistamine; epinephrine.
Desensitization therapies can also be considered for long-term management in cases where avoidance is not possible, as they aim to gradually reduce the sensitivity to allergens.
Hypersensitivity Type II
Tissue-specific
Antibody (IgG or IgM) binds to specific tissue antigen on cell surface and activates complement cascade, leading to cell membrane damage and lysis, phagocytosis, and other mechanisms.
Ex. Autoimmune hemolytic anemia, ABO-mismatched blood, Graves disease.
Manifestations are dependent on the tissue.
Hypersensitivity Type III
Immune complex- mediated (Antigen-antibody complexes formed in blood and deposited in vessel wall or extravascular tissue).
IgG or IgM binds to circulating antigen.
Not tissue-specific.
Dynamic and heterogeneous.
Complement activation → Neutrophils and lysosomal enzymes → tissue damage.
Ex. Raynauds phenomenon, SLE, glomerulonephritis, arthritis.
Systemic Lupus Erythematosus (SLE)
Autoimmune collagen-vascular disorder (Immune system attacks native tissue)
Antigen-antibody (immune) complexes (type III) trapped in tissues. This can lead to intense inflammatory response which then leads to arthritis, dermatitis, pleuritis, pericarditis, glomerulonephritis.
Immune complexes on blood cell surfaces lead to complement activation. This leads to cell lysis, which in turn leads to:
Anemia
Leukopenia
Thrombocytopenia
Lymphopenia
Hypersensitivity Type IV
Cell-mediated (NOT ANTIBODY MEDIATED)
Mediated by T lymphocytes, not antibody.
Cytotoxic T lymphocytes or Th cells leads to ROS and cell lysis.
Ex. Acute graft rejection, TB skin test, poison ivy, metal allergies, type 1 DM.
HIV/AIDS Pathophysiology
Ongoing viral replication- hallmark of symptomatic HIV infection.
Asymptomatic until CD4+ Cell count <200/mm³.
Release of HIV copies into blood.
Manifestations
Early stage HIV infection: fatigue, headache, fever.
AIDS: Weight loss, anorexia, opportunistic infections/cancers, cachexia, fever.
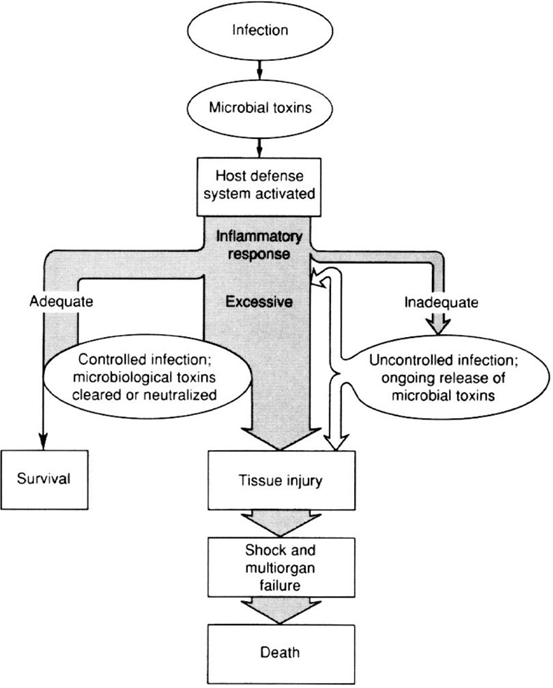
Infection
Microorganisms → Disease
Stages of infection
Encounter/transmission → colonization → invasion → dissemination & tissue damage.
Tissue damage from bacterial products (eg. toxins) and/or inflammatory response.
Toxin production
Exotoxins (gram-positive)
Enzymes released during bacterial growth
Immunogenic- antitoxin production (eg. Tetanus, diphtheria).
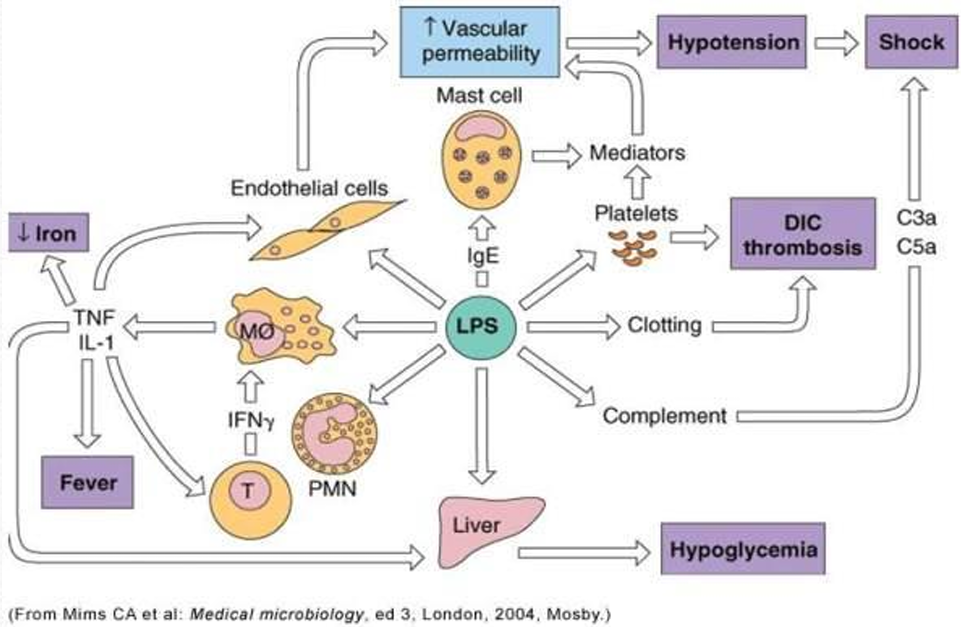
Endotoxins (Gram-negative)
Lipopolysaccharides (LPS) contained in cell walls.
LPS is the toxin.
When gram negative bacteria die, the endotoxins are released.
Pyrogenic effects.
Release of vasoactive peptides leads to vasodilation.
Clotting cascade activated leads to intravascular coagulation.
Clinical stages of infection
Incubation- Exposure to manifestations (aka. clinical latency).
Prodromal- mild manifestations (sickness behaviors).
Invasion (acute illness)- Inflammatory & immune responses triggered; manifestations due to pathogen and/or immune responses.
Convalescence- pathogen removed, fatal, latency.
Manifestations:
Variable, nonspecific
Malaise
Fatigue
Weakness
Aches
Lower concentration
Lower appetite
Fever
Endogenous pyrogens
Released by host cells
IL-1, IL-6, TNF-a.
What is bacteremia?
Bacteremia refers to the presence of bacteria in the bloodstream, which can lead to severe infections and trigger systemic inflammatory responses in the body.
What is sepsis?
Sepsis is a life-threatening condition that arises when the body's response to infection injures its own tissues and organs, often leading to a cascade of systemic inflammation, organ dysfunction, and in severe cases, septic shock.
What is septicemia?
Septicemia is a serious bloodstream infection characterized by the presence of pathogens, such as bacteria or fungi, in the blood, which can lead to sepsis and require urgent medical intervention.
What is septic shock?
Septic shock is a severe and potentially fatal condition that occurs when sepsis leads to a significant drop in blood pressure, resulting in inadequate blood flow to organs and tissues. This state of profound circulatory failure is a medical emergency that requires immediate treatment to restore hemodynamic stability and prevent multi-organ failure.
Toxin Production
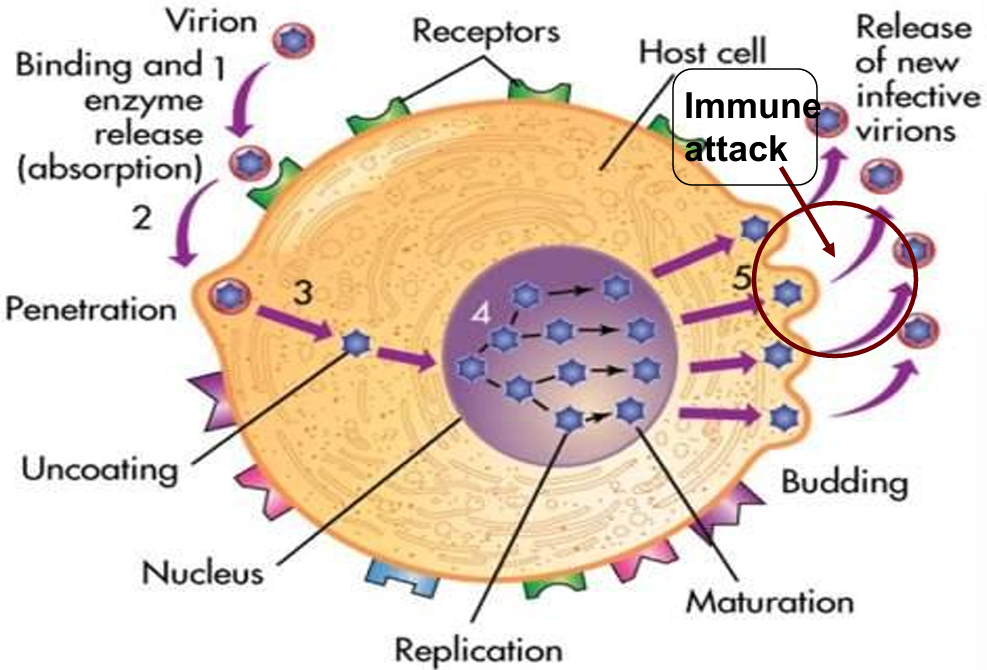
Viral replication
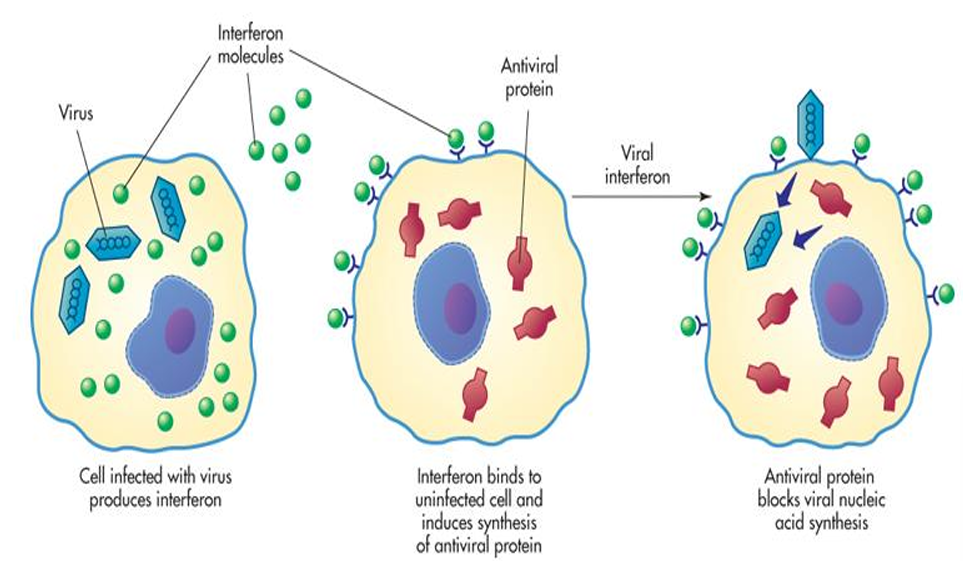
Interferon as Viral Protector
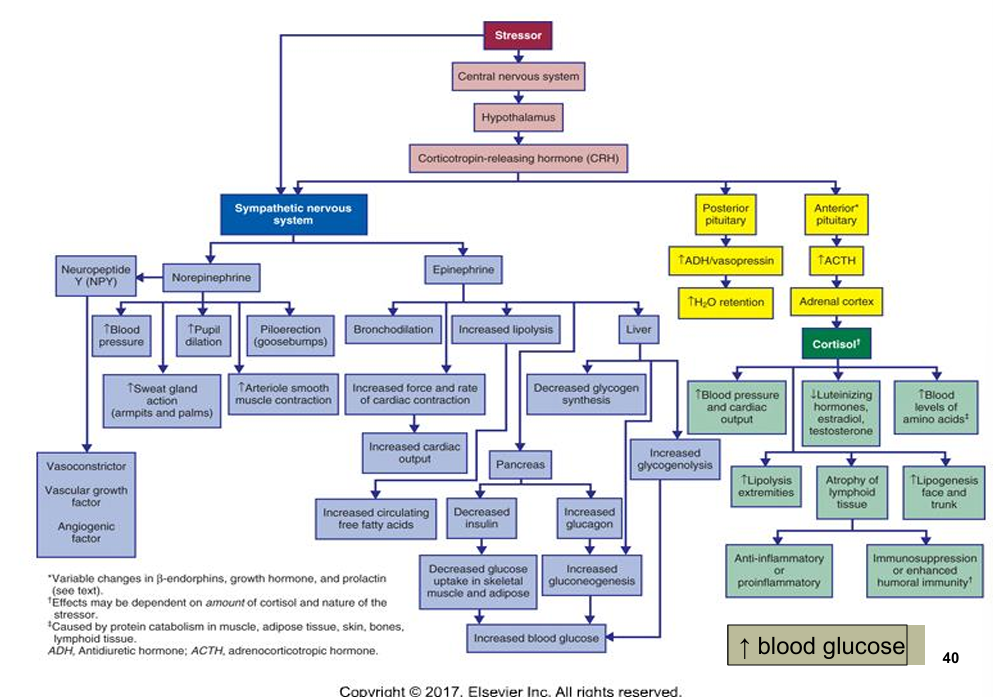
General adaptation syndrome (theory of stress)
Alarm stage (arousal)
Activates sympathetic nervous system (SNS) which leads to release of epinephrine & norepinephrine.
Activates hypothalamic-pituitary-adrenal (HPA) axis, which leads to release of Cortisol.
Resistance/Adaptation stage (mobilization to fight/flee/freeze)
Continued SNS & HPA stress hormone secretion (epinephrine and cortisol).
Exhaustion stage (Aka. Allostatic overload)
If stress continued & adaptation unsuccessful → progressive breakdown of compensatory mechanisms → disease onset.
Impaired immune response → death.
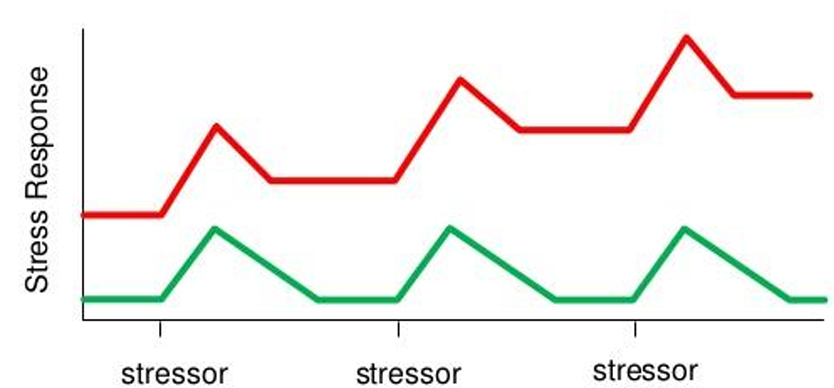
Stress Response
Allostasis vs allostatic load (theory of stress)
Constructive/adaptive coping (Allostasis): Arousal reactions return to a healthy baseline after stressor is dealt with.
Maladaptive coping (Allostatic overload): Arousal reaction continues after stressor has been dealt with. Baseline of arousal reaction moves steadily upward causing progressive “wear and tear”.
Enzyme inhibitors stop the inflammatory response.
Effects of Glucocorticoid Rx
Adaptive (Pros)
Gluconeogenesis which creates energy.
Catabolism → amino acids for protein synthesis.
Protein redistribution to damage tissue.
Lower B cell and T cell activity prevents immune-mediated tissue damage.
Destructive (Cons)
Decreased wound healing, increased infection risk, decreased inflammatory response. Inhibits:
Leukocytes at site of inflammation.
Kinins, prostaglandins, histamine.
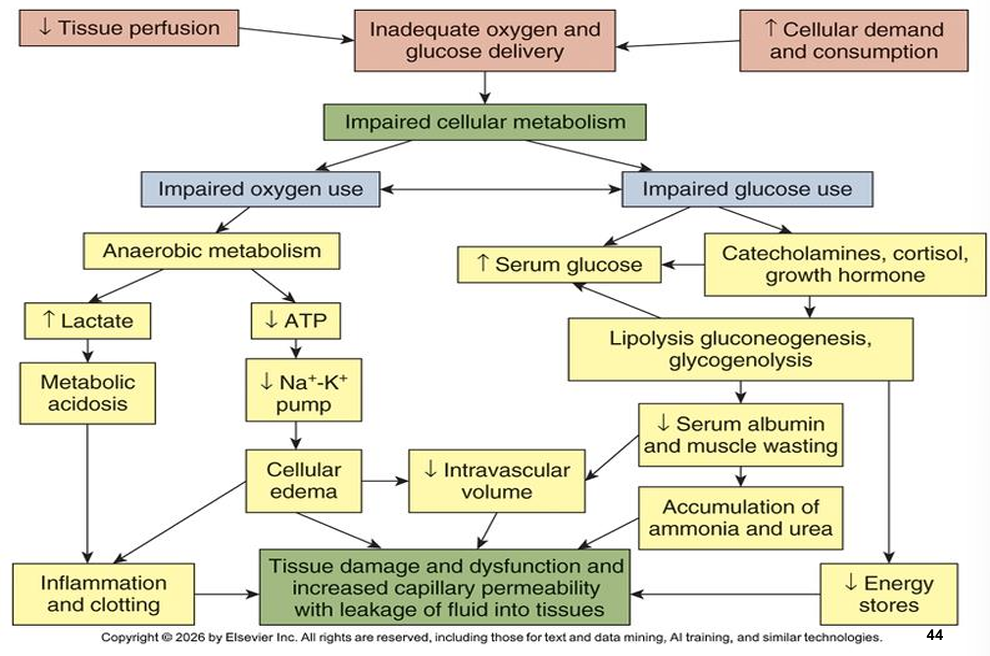
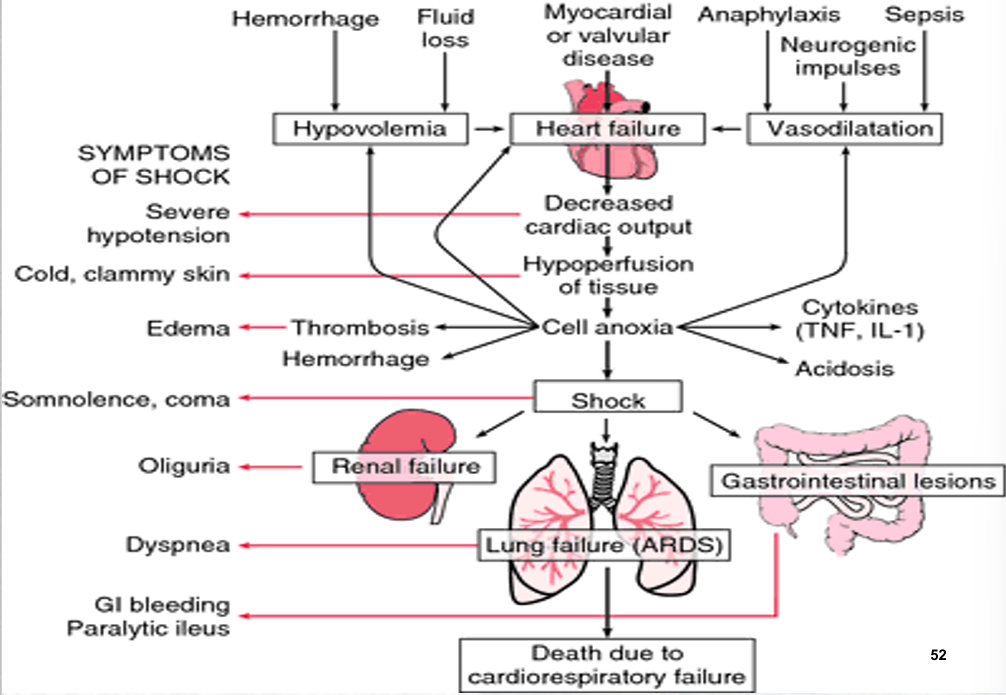
Shock: Impaired Cellular Metabolism
Preload and afterload
Preload
Volume of blood in ventricles at end of diastole (End diastolic pressure).
Afterload
Resistance left ventricle must overcome to circulate blood.
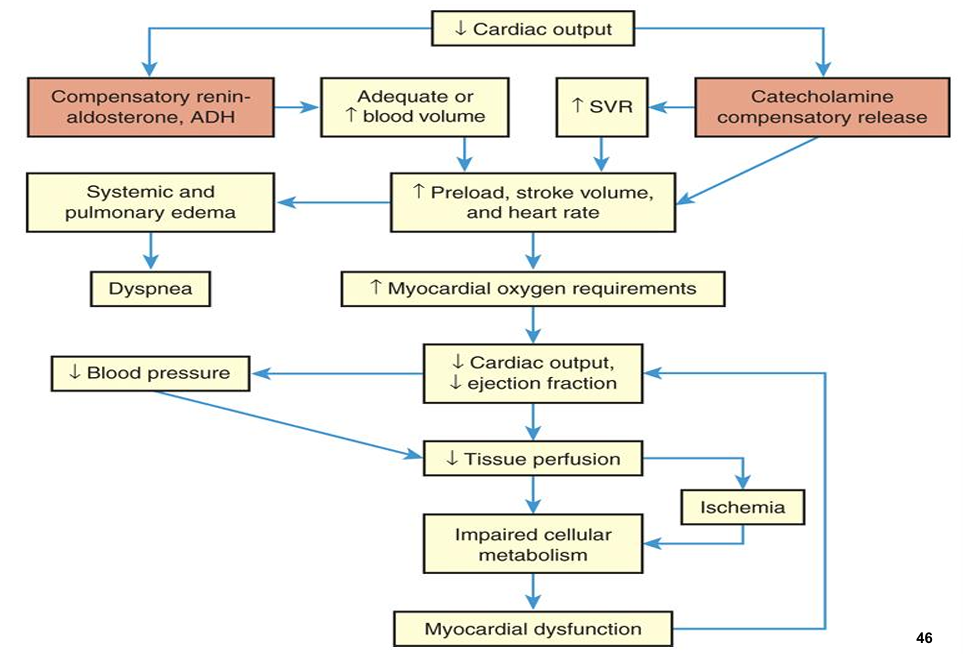
Shock: Cardiogenic
Occurs when the heart is unable to pump sufficiently to maintain blood flow to meet the body's needs, often resulting from conditions such as myocardial infarction or severe heart failure.
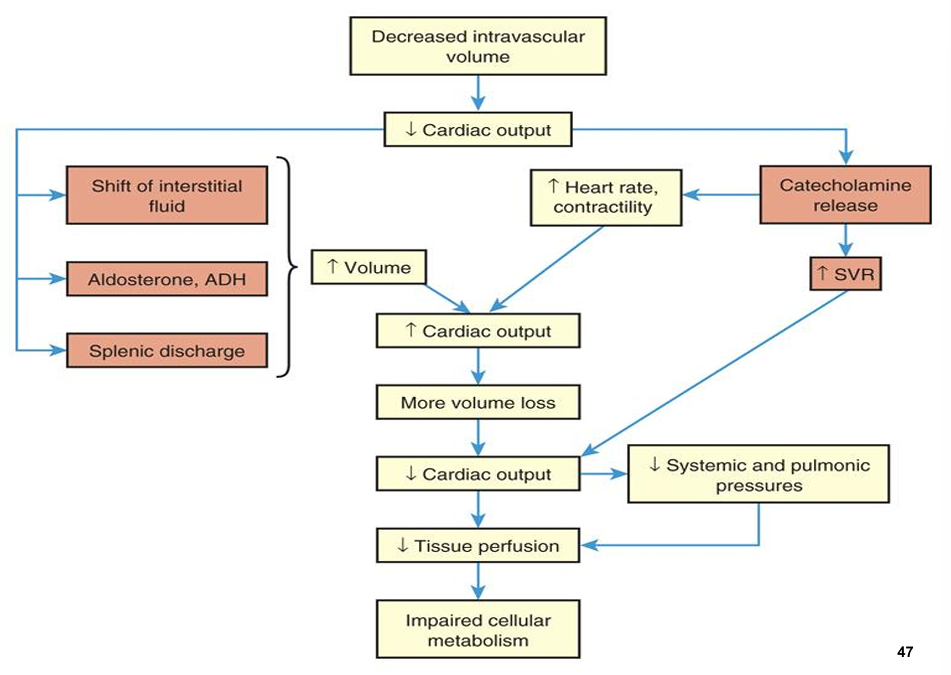
Shock: Hypovolemic
Occurs when there is insufficient blood volume, often due to severe bleeding, dehydration, or fluid loss. This type of shock can lead to a drop in blood pressure and is critical to address promptly to restore adequate circulation.
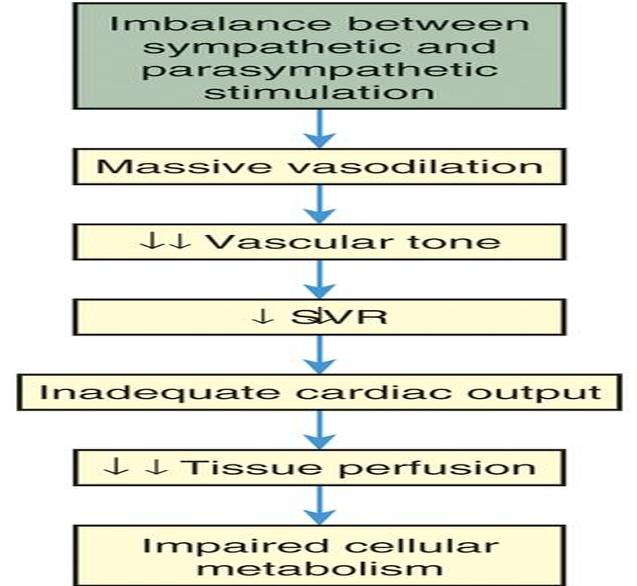
Shock: Neurogenic
This type of shock occurs when there is a disruption in the autonomic nervous system regulation of blood vessels, often resulting from spinal cord injuries or severe pain. It can lead to widespread vasodilation, causing hypotension and inadequate perfusion to vital organs.
No compensation compared to other forms of shock.
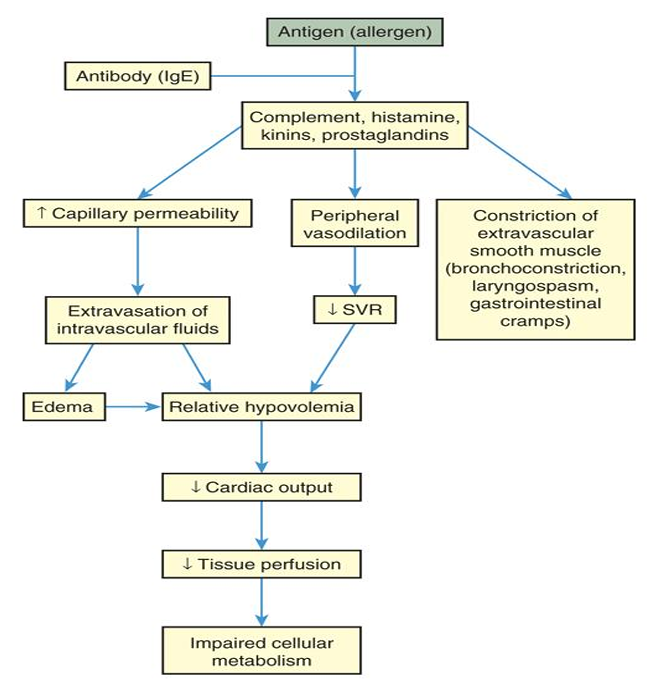
Shock: Anaphylactic
This type of shock is a severe allergic reaction that causes the release of histamine and other chemicals into the bloodstream, resulting in widespread vasodilation, bronchoconstriction, and increased vascular permeability. Symptoms may include difficulty breathing, swelling of the throat, and a rapid drop in blood pressure, making it crucial to administer epinephrine promptly to counteract these effects.
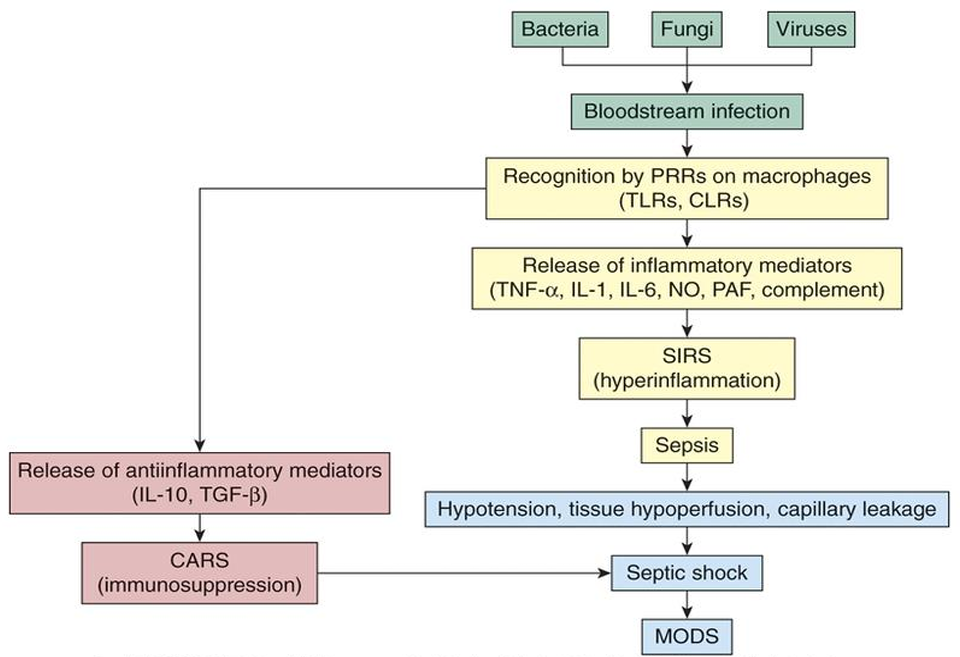
Shock: Septic
This type of shock is due to severe infections that lead to systemic inflammatory response syndrome (SIRS). In septic shock, pathogens or toxins enter the bloodstream, causing widespread inflammation and subsequent vasodilation. As a result, patients may experience fever, chills, and altered mental status, along with hypotension and organ dysfunction. Early recognition and treatment with antibiotics and fluid resuscitation are essential to improve outcomes.
Shock: Clinical manifestations
The clinical manifestations of shock can vary depending on its etiology, but common signs include:
Tachycardia: Increased heart rate as the body attempts to maintain adequate perfusion.
Hypotension: Low blood pressure reflecting reduced blood flow to vital organs.
Cool, clammy skin: Due to peripheral vasoconstriction as the body redirects blood flow to essential organs.
Altered mental status: Patients may appear anxious, confused, or lethargic depending on the severity of the shock.
Rapid or shallow breathing: A compensatory mechanism in response to metabolic acidosis and reduced oxygen levels.
Decreased urine output: Resulting from renal hypoperfusion.
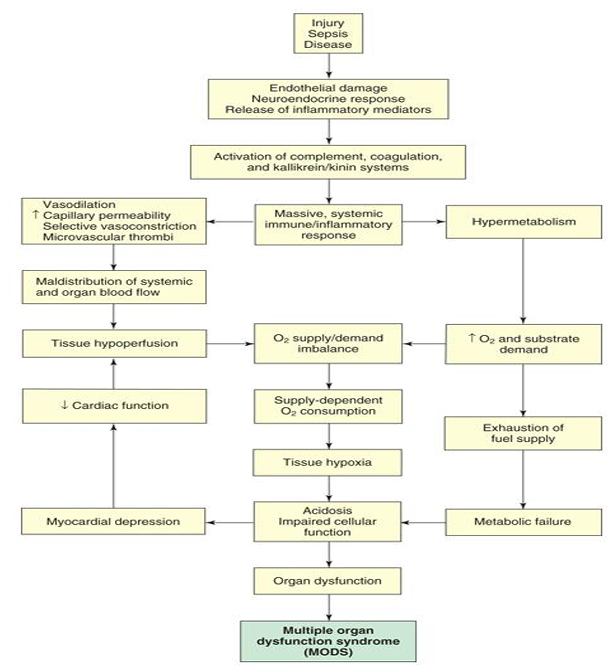
MODS: Pathophysiology
Multi-Organ Dysfunction Syndrome (MODS): A complex clinical syndrome characterized by the progressive failure of two or more organ systems, often triggered by an initial insult such as sepsis or trauma, leading to derangements in homeostasis. In MODS, the interplay between systemic inflammation and impaired perfusion culminates in organ dysfunction, necessitating prompt recognition and intervention to mitigate further damage.