Brain tumors
Intracranial pressure
Intracranial pressure (ICP) refers to the pressure within the skull caused by the volume of three main components:
Brain tissue
Cerebrospinal fluid (CSF)
Blood (mainly venous)
Monroe-Kelly doctrine: the volume of the intracranial components - brain tissue, blood, CSF - is constant.
Increase of any of them is possible only at the expense of the other two, and that increases the intracranial pressure.
Symptoms of increased intracranial pressure
Headache (diffuse, continous, progressive in character)
Nausea, vomitus
Disturbances of consciousness
Cushing phenomenon: bradycardia, increased systolic blood pressure
Bilateral edema of the optic disc
Diplopia (due to bilateral abducent nerve palsy)
Increased intracranial pressure
Space-occupying lesions: tumors, brain oedema, inflammation, abscess, haemorrhage, brain infarction, brain contusion, occlusive hydrocephalus, parasites, etc.
Changes in CSF flow: subarachnoideal hemorrhage, meningitis.
Circulatory disturbances: extremely high arterial blood pressure, thrombosis of the cerebral veins or venous sinuses.
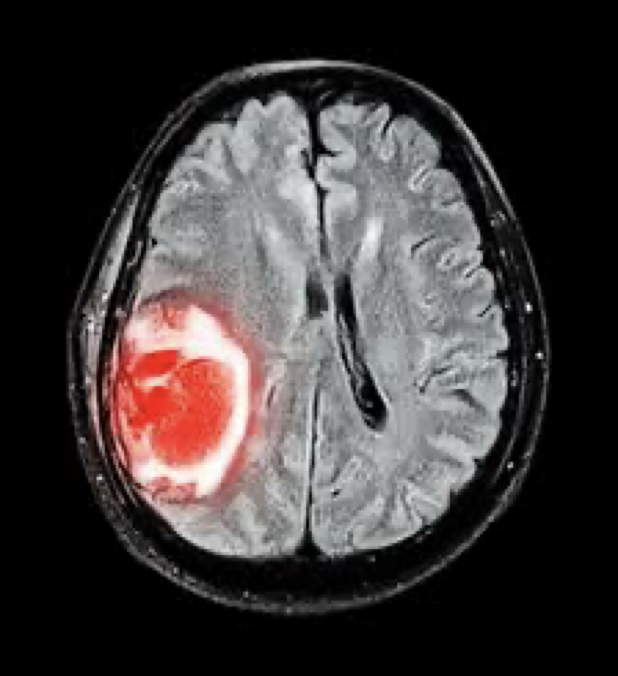
brain tumors
Brain tumors charaterised by:
Insidious development of symptoms is typical for brain tumors.
Sudden worsening or onset of new symptoms may be a consequence of intratumoral haemorrhage or herniation.
Brain tumors - symptoms
Focal signs: Direct effect of the tumor leads to damaged function (e.g. paresis, hypaesthesia, visual field defect). Positive symptoms - focal or generalized epileptic seisures
Compression signs: Effects on surrounding structures, tracts, cranial nerves, CSF pathways resulting in hydrocephalus.
General symptoms caused by the increased intracranial pressure, mass effect of the tumor, independent from its nature.
Psychiatric signs: cognitive, behavioural or personality changes (sometimes leading or only features of the tumor)
Hormonal changes - result of dysfunction of the pituitary gland
Sometimes tumor may be exactly localized by the findings of the physical examination.
In the suspicion of brain tumor imaging methods are indicated.
Brain tumors - diagnostics
Brain CT: Administration of contrast media (containing iodine) is necessary. CT is not proper for small tumors, mainly in the posterior fossa (bony artefacts). CT is prior to MR in evaluation of intratumoral calcification an bone destruction. Some tumors have characteristic CT features (e.g. meningiomas)
Brain MR: The proper method of diadnostics of brain tumors. More detailed spatial resolution, multi-planar imaging, all parts of the brain are well visualized. The best method for surgical planning
Angiography: Disclosing of the blood supply of some hyper-vascularized tumors (e.g. angiomas, meningiomas
Brain SPECT and PET: Evaluation of circulation and metabolism of tumors. Differentation between tumors and lesions of other nature in controversary cases.
Brain biopsy: CT assisted, „stereotaxic” procedure. Exact histological classification of tumors (grading)
Additional tests:
CSF examination
EEG
Evoked potentials
Hormonal tests
Genetics
Brain tumors - classification
Neuroepithelial tumors
Tumors of the peripheral nerves
Tumors originated from the meninges
Metastatic tumors
Neuroepithelial tumors
Astrocytomas (graded I-IV)
The most malignant form is Glioblastoma multiforme
High malignancy, rapid growth, infiltrative
Symptoms: seisures, focal signs, elevated intracranial pressure, headache,
psychiatric disorders (depression, behavioural or personality changes)
Diagnosis: CT, MR
Treatment: surgical; total removal is not possible. Irradiation and chemotheraby mav be added. High rate of recurrence, poor survival (maximum 1,5 year)
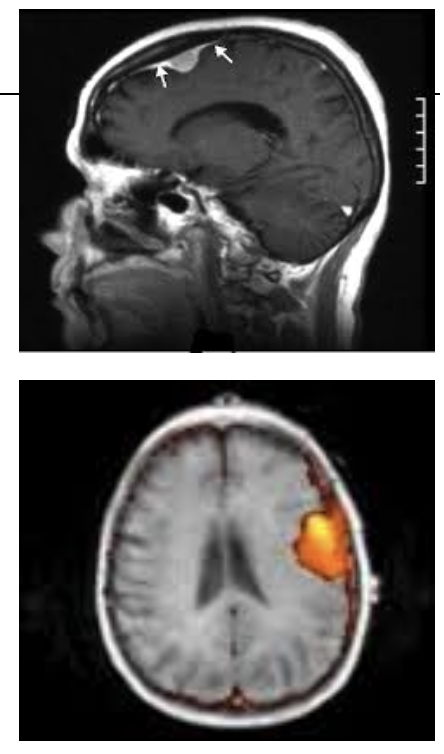
Tumors originated from the meninges
Meningiomas: any age. Slow growth (20-30 years), but may reach extreme sizes. Rarely turns into malignancy. May destroy bones of skull.
Originated from cells of the arachnoidea.
Symptoms: depending on localisation. Epileptic seisures may occur.
Diagnosis: CT, MR
Treatment: surgical, total removal if possible. Total recovery may be achieved.
Metastatic brain tumors
In many cases the brain metastasis is diagnosed before the recognition of the primary tumor. Sometimes the origin is not found at all.
Metastatic brain tumors in order of frequency:
Lung 64%
Breast 14%
Unknown origin 8%
Malignant melanoma 4%
Symptoms: not different than the primary tumors: focal epileptic seizures are quite frequent
Diagnosis: CT, MR and biopsy
Treatment: Solitary metastasis: surgical removal is possible. Multiplex metastasis: irradiation or chemotherapy.
Brain tumors are not frequent, but we have to consider them.
The symptoms of brain tumors are not specific.
New onset headache or epileptic seisures always indicate a search for brain tumor.
Some types of brain tumors recognized in time have good outcome.