The Field of Clinical Psychology - Chapter 1
What is Clinical Psychology?
What does this profession look like in Canada?
How did clinical psychology develop?
Mental Health in Canada
Province
Each province has its own specific regulations and resources to address mental health issues, ensuring that services are tailored to meet the unique needs of their populations
Provincial government make the decisions regarding their funding
Funding Fed vs Prov
Provinces
They are in charge of mental health services, like hospitals, therapy, and crisis programs.
They decide how to spend money on mental health
Provinces: Make the rules and decide how to use funding
Federal
Gives money to provinces through the Canada Health Transfer (CHT).
In 2017, promised $5 billion over 10 years for mental health
Pays for mental health services for Indigenous people, veterans, and federal inmates
Federal: Provides money but does not control how it’s used
Canadian Mental Health Association:
A organization that promotes mental health awareness and provides support services across Canada
Works on a national, provincial and local level
Non profit organization that relies on donations and grants to fund its initiatives and programs aimed at improving mental health care and education
The Mental health Commission of Canada (MHCC: established 2006)
Purpose & Mission
A non-profit organization focused on improving the mental health and well-being of Canadians
Core Principles
Access to Services – Every individual with a mental health condition should receive the necessary support and care.
Respect & Dignity – People with mental disorders should be treated with the same respect as those facing other health challenges.
Key Initiatives & Projects of the MHCC
Opening Minds (Anti-Stigma & Discrimination Campaign)
Canada's largest systematic effort to reduce stigma surrounding mental illness.
Targets healthcare providers, workplaces, youth, and the media to change attitudes.
Uses research-backed approaches to break stereotypes.
Mental Health First Aid (MHFA)
A training program that educates people on how to assist individuals in distress or experiencing a crisis (e.g., panic attacks, suicidal thoughts).
Similar to traditional first aid but focuses on mental health conditions like depression, anxiety, psychosis, and substance use disorders.
Helps reduce fear and misconceptions about mental illness.
Mental Health Strategy for Canada
A nationwide plan to improve mental health services and policies.
Highlights that Canada was lagging behind other developed nations in having a national strategy.
Focuses on prevention, early intervention, and increased funding for mental health services.
Knowledge Exchange Centre
Provides evidence-based resources on mental health to professionals, policymakers, and the public.
Helps ensure that decisions are informed by the latest research.
Aims to bridge the gap between research and practice.
Housing First
Supports homeless individuals with mental illness by providing stable housing without conditions (e.g., sobriety or treatment compliance).
Offers wraparound services tailored to individual needs (mental health support, job assistance, etc.).
Research shows stable housing improves mental health and reduces hospitalizations.
Peer Project
Promotes peer support programs by training people with lived experience of mental illness to help others.
Establishes national guidelines to improve the quality and effectiveness of peer support.
Recognizes peer support as a valuable part of mental health recovery.
Why This Matters
The MHCC plays a critical role in shaping mental health policy in Canada.
Its initiatives are evidence-based and focus on real-world impact.
Programs like Mental Health First Aid and Housing First are proven to be effective in improving lives.
Reducing stigma through Opening Minds helps change societal attitudes toward mental health.
The Mental Health Professions
Psychiatrists?
Medical doctors who specialize in diagnosing, treating, and preventing mental illnesses.
They focus on the biological causes of mental disorders, including brain chemistry and physical health.
Training Path
4 years of medical school.
5-year psychiatry residency.
Can specialize in areas like child psychiatry or geropsychiatry (mental health in older adults).
How They Differ from Psychologists
Psychiatrists study the brain and medications; psychologists focus on thoughts, behaviors, and therapy.
Psychiatrists prescribe medication; psychologists (in Canada) cannot.
Psychiatrists have less training in research and psychological development than clinical psychologists.
Treatment Methods
Mainly use medications to treat mental disorders.
Some psychiatrists also use therapy (e.g., CBT, interpersonal therapy).
Psychiatry has shifted from psychoanalysis to evidence-based treatments like medication and CBT.
Shortage of Psychiatrists
Canada has about 4,770 psychiatrists (as of 2016).
In the U.S., there are 13.7 psychiatrists per 100,000 people.
The number of medical students choosing psychiatry has dropped by 40% since the 1980s
Clinical Social Workers
Improve the health and well-being of individuals, families, groups, and communities.
Work in hospitals, mental health centers, schools, and social service agencies.
Tasks include:
Policy development
Program planning
Case management
Therapy
Advocacy
Regulation & Growth in Canada
Titles like "Social Worker" and "Registered Social Worker" are regulated by provincial/territorial bodies.
The number of registered social workers in Canada grew to nearly 44,000 in 2013 (CIHI, 2015).
Social Workers in Mental Health
Often part of mental health teams.
Frequently work as case managers, coordinating care for people with severe disorders like:
Schizophrenia
Bipolar disorder
Help patients navigate complex healthcare systems and manage conflicting demands from multiple service providers.
Education & Training
Requirements vary by province:
Alberta: Minimum 2-year diploma.
Other provinces: Undergraduate or master’s degree in social work.
Training focuses on:
Social determinants of health (how social factors impact mental health).
Consequences of mental illness on individuals and communities.
Clinical social workers are now required to provide evidence-based therapy, like:
Interpersonal therapy
Cognitive therapy for adult depression
Psychotherapists
Treat mental health issues through talk therapy, focusing on thoughts, emotions, and behaviors.
Help individuals, couples, families, and groups with issues like:
Anxiety & depression
Trauma & PTSD
Addiction
Relationship & family conflicts
Use evidence-based therapies, such as:
Cognitive Behavioral Therapy (CBT)
Interpersonal Therapy (IPT)
Psychodynamic Therapy
Where Do They Work?
Hospitals & mental health clinics
Private practice
Community health centers
Schools & workplaces
Regulation & Licensing in Canada
Title "Psychotherapist" is regulated in some provinces, like Ontario (CRPO) and Québec (OPQ).
In other provinces, psychotherapy can be practiced by psychologists, social workers, or counselors.
Unlike psychiatrists, psychotherapists cannot prescribe medication.
Education & Training
Master’s degree in psychology, social work, or counseling is often required.
Training focuses on:
Human development & cognition
Therapeutic techniques
Ethics & professional practice
Supervised clinical practice is typically required before full licensing
Psychiatric Nurses
Provide care for individuals with mental health and developmental needs.
Work in settings such as:
Acute psychiatry (hospital mental health units)
Geriatric care (older adults' mental health)
Correctional facilities (prisons and rehabilitation centers)
Community mental health programs
Residential care homes
Responsibilities
Administer medications & monitor patients in inpatient settings.
Provide psychoeducation & counseling to patients and families.
Supervise support staff in mental health facilities.
Assist with mental health crisis intervention and patient safety.
Regulation & Workforce in Canada
Regulated in four western provinces (British Columbia, Alberta, Saskatchewan, and Manitoba).
In 2013, there were 5,273 registered psychiatric nurses in these provinces (CIHI, 2015).
Education & Training
Requires either:
2- or 3-year diploma in psychiatric nursing, or
Bachelor’s degree in nursing with specialized mental health training.
Training includes:
Mental health assessment & management
Psychotropic medication administration
Crisis intervention techniques
Case Managers
Role in Mental Health Teams
Many social workers work in mental health teams alongside psychiatrists, psychologists, and nurses.
They often serve as case managers, helping patients access the care they need.
What is Case Management?
Coordinating services between different healthcare and social agencies.
Helping patients navigate complex care systems.
Ensuring services work together smoothly, especially for individuals with severe mental disorders like:
Schizophrenia
Bipolar disorder
Why is Case Management Important?
Patients with severe mental illness often receive care from multiple providers, leading to conflicting demands.
Case managers help:
Reduce confusion in treatment plans.
Improve communication between agencies.
Ensure patients receive consistent and appropriate care
The Role of Mind/Body in Health
Enlightenment/Early Modern Period (Europe)
Descartes: Articulates a common western system of thought
Use of logic and reason to show that there are 2 things: “mind/body” and “body/material”
Which leads to the distinction between mental processes and physical substances, laying the groundwork for future discussions on the interplay between psychological and physiological health
Early Views on Mental Health
Ancient beliefs attributed mental illness to supernatural causes (e.g., witchcraft, possession).
Hippocrates (Father of Medicine) introduced a biopsychosocial approach, suggesting that:
Health is influenced by biological, psychological, and social factors.
Mental illness was due to imbalances in bodily fluids (humors).
Philosophers like Plato and Aristotle expanded on these ideas, focusing on reason, emotion, and behavior.
The Shift Toward Natural Explanations
St. Vincent de Paul (late 1500s) rejected supernatural explanations, arguing that mental illness had natural causes.
Despite this, inhumane asylum treatments continued, including:
Isolation in asylums.
Painful treatments (e.g., bleeding, cold water immersion).
The Enlightenment & Mental Health Reform (Late 1700s)
Science began influencing mental health treatment.
Key reformers:
Philippe Pinel (France): Freed patients from chains and promoted compassionate care.
William Tuke (England): Advocated for humane treatment.
Benjamin Rush (USA): Introduced moral therapy, emphasizing patience over punishment.
The Rise of Neurology & Psychological Approaches
Growing interest in neurology expanded understanding of mental illness.
Jean-Martin Charcot used hypnosis to treat hysteria, influencing:
Pierre Janet – studied psychological trauma.
Sigmund Freud – developed psychoanalysis, focusing on unconscious processes.
This marked the beginning of clinical psychology as a distinct field
History of Treatment/Intervention
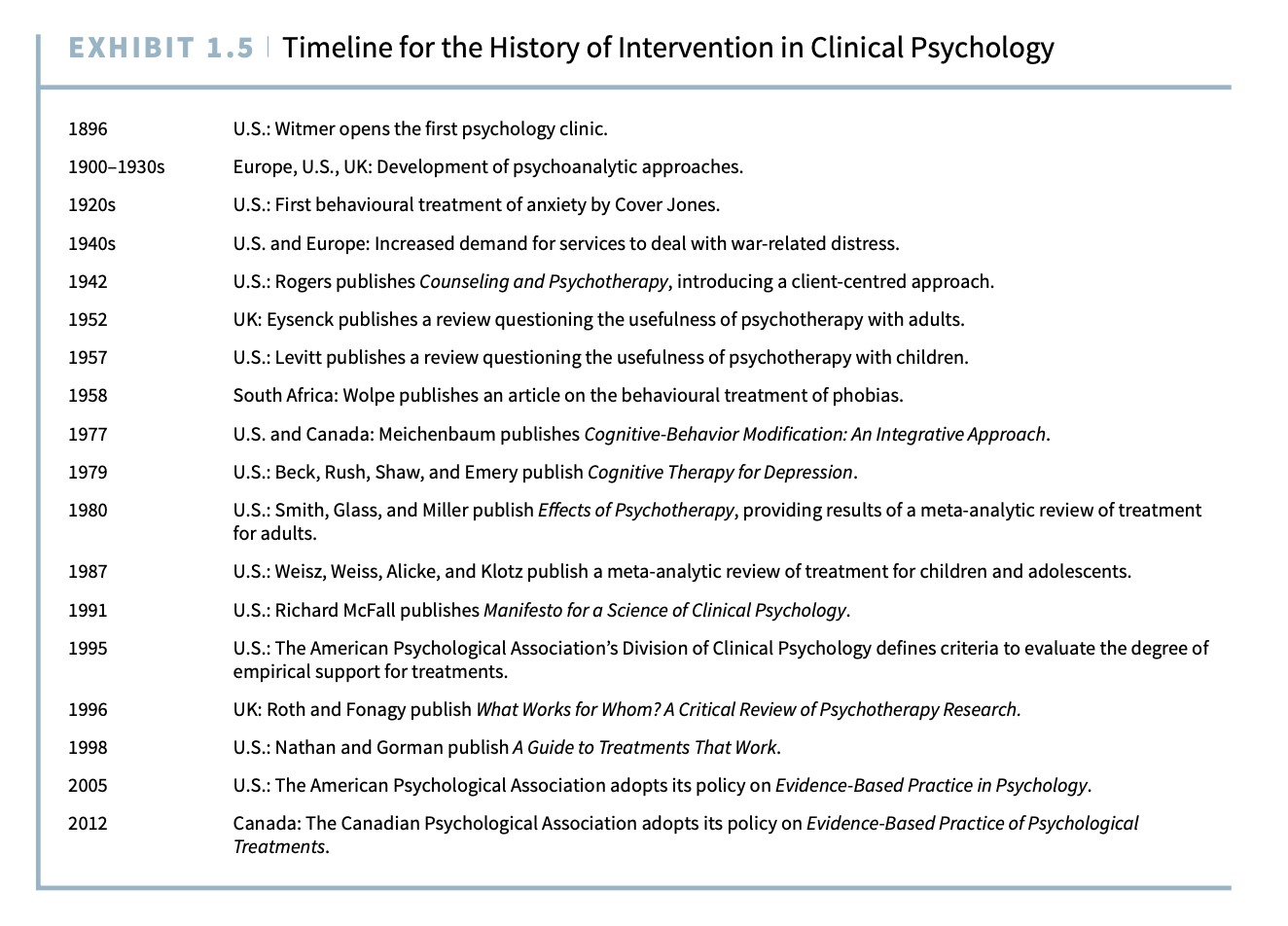
Late 1800s - Early 1900s: The Birth of Clinical Psychology and Psychoanalysis
1896: Lightner Witmer opens the first psychology clinic, marking the beginning of clinical psychology.
1900-1930s: Sigmund Freud develops psychoanalysis, emphasizing the unconscious mind in psychological distress.
Other Key Figures:
Carl Jung: Introduces the concept of the collective unconscious.
Alfred Adler: Focuses on social influences and birth order in personality development.
Anna Freud: Advances ego psychology, emphasizing conscious coping strategies.
1920s - 1940s: The Rise of Behaviourism and Increased Demand for Psychological Services
1920s:
John Watson’s Little Albert experiment demonstrates the conditioning of fear.
Mary Cover Jones applies conditioning principles to treat phobias, laying the groundwork for behaviour therapy.
1940s:
World War II creates a demand for mental health services, leading to an increase in trained clinical psychologists.
The Veterans Administration in the U.S. funds clinical psychology training programs.
1950s - 1970s: The Expansion of Psychotherapy Approaches
1952: Hans Eysenck questions the effectiveness of psychotherapy, sparking a push for research-based treatments.
1957: Carl Rogers introduces client-centred therapy, emphasizing empathy and personal growth.
1958: Joseph Wolpe develops systematic desensitization for phobia treatment.
1960s - 1970s:
Cognitive and behavioural therapies emerge, combining learning principles with cognitive restructuring.
Albert Ellis develops Rational Emotive Therapy (RET).
Aaron Beck publishes Cognitive Therapy for Depression (1979), formalizing cognitive therapy.
Donald Meichenbaum pioneers Cognitive-Behavior Modification (1977).
1980s - 1990s: The Rise of Evidence-Based Practice
1980: Meta-analysis by Smith, Glass, and Miller confirms the effectiveness of psychotherapy.
1987: Research extends to children and adolescents, showing similar benefits from therapy.
1991: Richard McFall’s Manifesto for a Science of Clinical Psychology urges the use of only scientifically validated treatments.
1995: The APA Task Force on Promotion and Dissemination of Psychological Procedures defines criteria for evaluating treatment efficacy.
1996 & 1998: Key research reviews (What Works for Whom? and A Guide to Treatments That Work) establish empirical standards for therapy.
2000s - Present: Adoption of Evidence-Based Practice
2005: The American Psychological Association (APA) formally adopts Evidence-Based Practice in Psychology.
2012: The Canadian Psychological Association follows with its own policy on evidence-based psychological treatments
Key Takeaways:
Clinical psychology evolved from psychoanalysis to behaviourism, then to cognitive and integrative approaches.
WWII played a major role in increasing the need for trained clinical psychologists.
The effectiveness of psychotherapy became a major focus, leading to evidence-based practice.
Modern clinical psychology emphasizes treatments supported by empirical research
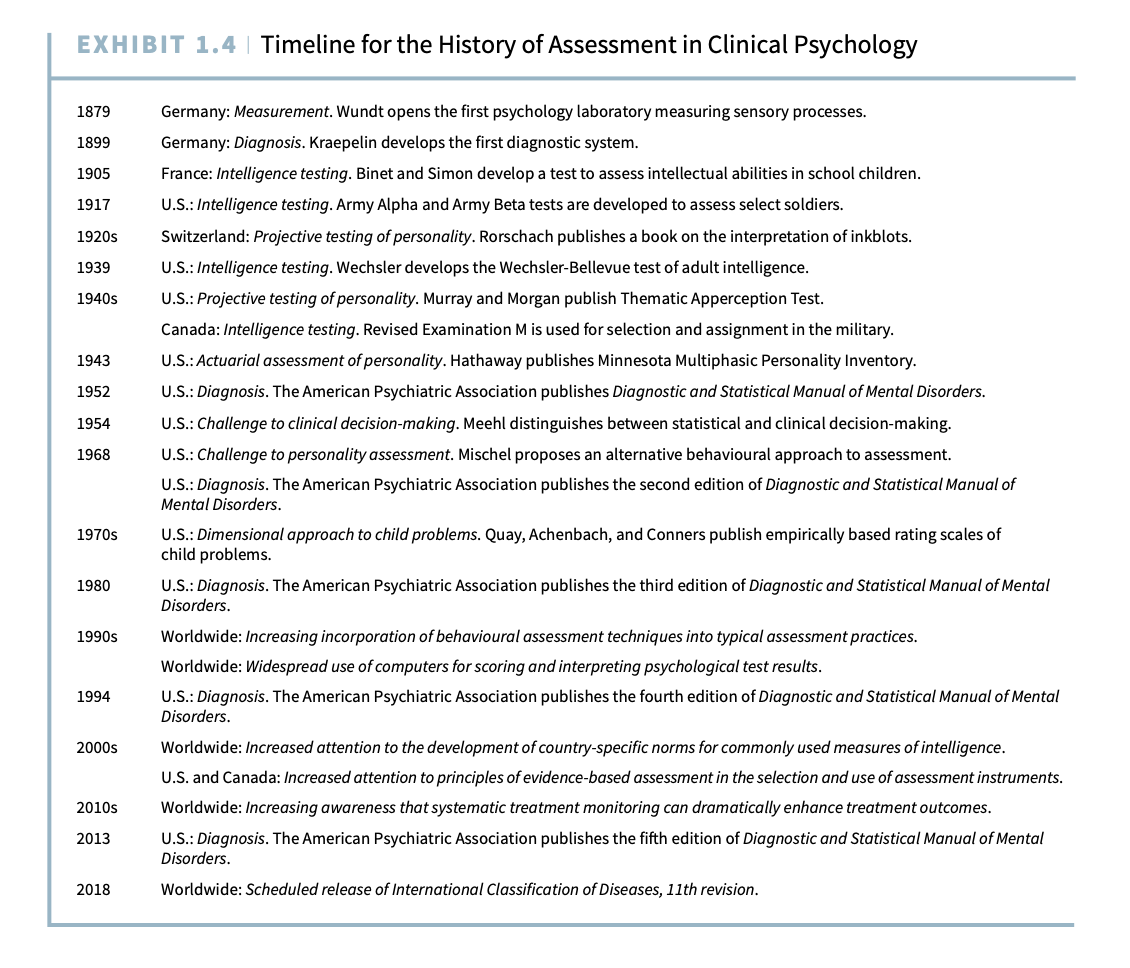
History of Assessment
Early Foundations of Clinical Psychology
Francis Galton (England, late 1800s): Studied individual differences, focusing on reaction times and motor skills to measure intelligence.
Wilhelm Wundt (Germany, 1879): Established the first psychology laboratory, emphasizing experimental methods to study perception and sensation.
James McKeen Cattell (U.S.): Expanded Wundt’s work, coined the term “mental tests”, and studied reaction times as measures of intelligence.
Emil Kraepelin (Germany, 1899): Developed the first classification system for mental disorders, influencing modern diagnostic tools like DSM and ICD.
2. Development of Psychological Testing
1905 – Binet-Simon Intelligence Test (France): Designed to assess schoolchildren’s intellectual abilities. Became the foundation for modern IQ tests.
1917 – Army Alpha and Beta Tests (U.S.): First large-scale intelligence tests used in the military to screen recruits in WWI.
1920s – Rorschach Inkblot Test (Switzerland): Introduced projective personality testing, where people interpret ambiguous inkblots.
1939 – Wechsler-Bellevue Intelligence Test (U.S.): Created a more comprehensive test for adult intelligence, leading to today’s WAIS (Wechsler Adult Intelligence Scale).
1943 – Minnesota Multiphasic Personality Inventory (MMPI, U.S.): First objective, empirically-based personality test to assess psychological disorders.
1940s – Thematic Apperception Test (TAT, U.S.): A projective test where individuals interpret ambiguous pictures, revealing unconscious motives.
3. Standardization of Diagnosis
1952 – DSM-I (U.S.): The American Psychiatric Association (APA) published the first Diagnostic and Statistical Manual of Mental Disorders (DSM), standardizing mental health diagnoses.
1980 – DSM-III: Introduced structured diagnostic criteria and removed Freudian-based concepts, making diagnosis more scientific.
2013 – DSM-5: The latest version, refining classifications and criteria based on new research.
2018 – ICD-11 (Worldwide): Updated version of the International Classification of Diseases, further aligning with DSM standards.
Challenges to Clinical Assessment
1. Clinical vs. Statistical Decision-Making
Paul Meehl (1954): Argued that statistical models often predict psychological outcomes better than subjective clinical judgment.
Walter Mischel (1968): Questioned personality testing, showing that behavior varies by situation rather than stable personality traits.
2. The Shift Toward Empirical and Standardized Methods
1970s: Introduction of behavior-based child assessment tools, using parent ratings and factor analysis (e.g., Achenbach, Quay, and Conners).
1990s: Growth of computerized assessment tools, increasing accuracy in psychological testing.
3. Focus on Clinical Utility & Service Evaluation
Clinical Utility: Does an assessment actually improve diagnosis and treatment?
Service Evaluation: Are psychological services effective in improving patient outcomes?
History of Intervention in Clinical Psychology
1. Early Psychodynamic Approaches
Sigmund Freud (1900): Introduced psychoanalysis, focusing on unconscious conflicts.
Carl Jung & Alfred Adler: Expanded psychoanalysis with concepts like the collective unconscious (Jung) and social development (Adler).
Harry Stack Sullivan (1940s): Developed interpersonal therapy, emphasizing relationships in mental health.
2. Rise of Behavioral and Cognitive Therapies
John Watson & Mary Cover Jones (1920s-30s): Developed behavior therapy by conditioning phobias and showing how they could be "unlearned."
Joseph Wolpe (1958): Created systematic desensitization for phobias, laying the groundwork for behavior therapy.
Albert Ellis (1960s): Developed Rational Emotive Therapy, challenging irrational thoughts to change behavior.
Aaron Beck (1979): Developed Cognitive Therapy of Depression, the foundation of today’s Cognitive-Behavioral Therapy (CBT).
3. The Growth of Empirically Supported Therapies
Hans Eysenck (1952): Criticized psychotherapy’s effectiveness, sparking a demand for research-based treatments.
Meta-Analysis (1980): Smith, Glass, & Miller analyzed 475 studies, confirming therapy’s effectiveness.
1995 – APA Task Force: Emphasized efficacy (lab-proven treatments) vs. effectiveness (real-world results).
2005 – Evidence-Based Practice (APA): Encouraged treatments backed by scientific research.
Key Concepts in Clinical Psychology
1. Meta-Analysis
A statistical technique combining multiple studies to measure overall treatment effectiveness.
Example: In 1980, Smith & colleagues found therapy improved outcomes for 80% of treated individuals.
2. Efficacy vs. Effectiveness
Term | Definition |
|---|---|
Efficacy | Proven effective in controlled lab settings (high internal validity). |
Effectiveness | Works in real-world conditions (high external validity). |
3. Evolution of Short-Term & Manualized Therapy
1990s: Short-term therapy became more common due to cost-cutting in healthcare.
Treatment Manuals: Standardized therapy methods to ensure consistent effectiveness across therapists.
Modern Trends in Clinical Psychology
1. Evidence-Based Practices
Use of research-supported treatments like CBT, Dialectical Behavior Therapy (DBT), and Acceptance & Commitment Therapy (ACT).
2. Technological Integration
Computerized assessments and AI in diagnosis.
Teletherapy and online mental health interventions.
3. Greater Focus on Cultural Sensitivity
Growing recognition of how culture affects mental health and assessment.
Development of culturally adapted therapy models.
Summary of Key Takeaways
Early clinical psychology focused on measuring intelligence (Binet, Wechsler) and diagnosing disorders (Kraepelin, DSM).
Personality assessments evolved from projective tests (Rorschach, TAT) to structured, empirical tools (MMPI).
Challenges to assessment methods led to a shift from clinical intuition to standardized, evidence-based testing.
Intervention methods changed from psychoanalysis to behavior therapy (Wolpe), cognitive therapy (Beck), and today’s evidence-based approaches (CBT).
Modern clinical psychology prioritizes data-driven, cost-effective, culturally aware, and technology-integrated practices
Terms
Evidence-based practice:
a practice model that involves the synthesis of information drawn from research and systematically collected data on the patient in question, the clinician’s professional experience, and the patient’s preferences when considering health care options
Bio-psychosocial approach:
a theoretical framework that takes into account biological, psychological, and social influences on health and illness
Syndrome:
group of symptoms that frequently co-occur
Clinical utility:
usefulness of assessment data to provide information that leads to a clinical outcome that is better (or faster or less expensive) than would be the case if the psychologist did not have the assessment data.
Service evaluation:
Activities designed to examine whether or not services work
Meta-analysis:
a review technique by which groups of studies are statistically combined and compared
efficacy:
evidence that a treatment has been shown to work under research conditions that emphasized internal validity
effectiveness:
evidence that a treatment has been shown to work in real-world conditions.
Important Names
Alfred Binet
The early work on assessment in clinical psychology
IQ tests
Hans Eysenck
Created a turning point for psychotherapy research and training
He analyzed psychotherapy outcomes and concluded that clients receiving psychodynamic or eclectic therapy improved at the same rate as those receiving no therapy.
This led him to argue that there was no evidence that psychotherapy was effective
His work reinforced growing dissatisfaction with Freud-influenced psychodynamic therapy.
It encouraged psychologists to develop empirically supported treatments based on scientific research
Emil Kraepelin
Convinced that all mental disorders were due to biological factors and that these biological factors could not be effectively treated by rather primitive methods
Devoted his career to the study and classification of mental disorders in the hope that his work would result in a scientifically based classification system that would have treatment implications
Richard McFall
He challenged the field of clinical psychology to only provide treatments that research had proven to be both effective and safe.
His stance emphasized the scientific validation of psychological interventions, reinforcing the need for empirical support in clinical practice
Published Manifesto for a science of clinical psychology
Paul Meehl
critiquing the clinical (subjective) approach and advocating for a statistical (objective) approach to diagnosis and prediction
Meehl compared two methods of psychological assessment:
Clinical Approach: Based on interviews, personal judgment, and subjective interpretation.
Statistical Approach: Used demographic data, test scores, and statistical formulas to predict outcomes.
He found that statistical predictions were generally more accurate than clinical judgment alone in diagnosing and predicting behavior
Carl Rogers
Client centered therapy is an approach developed by Carl Rogers that emphasizes the importance of the therapeutic relationship and the client's perspective in the healing process
This approach prioritizes empathy, unconditional positive regard, and active listening, allowing clients to explore their thoughts and feelings in a supportive environment