Mycoplasmas Exam 2
Mycoplasmas
General Characteristics
No Cell Wall:
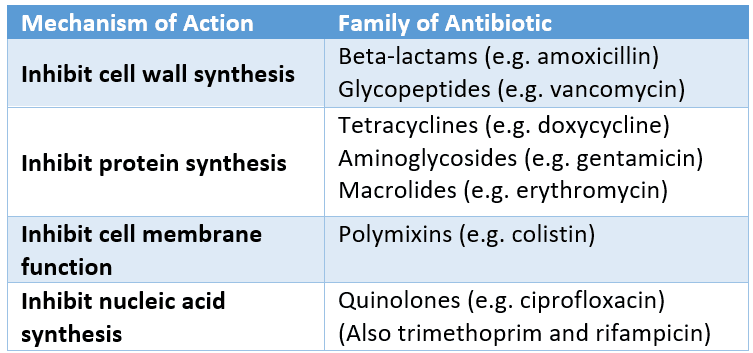
Significance: Many antibiotics target the bacterial cell wall (e.g., penicillins, beta-lactam antibiotics), making them ineffective against mycoplasmas.
Membrane Structure: Strong membrane containing sterols helps maintain integrity in absence of a cell wall.
Size: Among the smallest free-living organisms (around 0.2 microns), often appearing as specks of dust under a microscope.
Cultural Characteristics:
Often exhibit a "fried egg" appearance on agar media (dense center with a thin peripheral layer).
Clinically Important Species
Mycoplasma pneumoniae:
Causes respiratory infections; significant virulence due to cytotoxin production leading to cell death.
Adheres to respiratory epithelial cells, inhibits ciliary movement, leading to cough and respiratory distress.
Symptoms of Walking Pneumonia: Slow onset, less acute than typical bacterial pneumonia, often resulting in community-acquired infections.
Mycoplasma genitalium:
Associated with urethritis (not gonococcal). So, NGU, and pelvic inflammatory disease.
Mycoplasma hominis
Respiratory and genitourinary, ststemic infection in compromised patients and pyelonephritis.
Ureaplasma urealyticum:
Involved in various urogenital infections including pelvic inflammatory disease. Can be respiratory and genitourinary. NGU, premature birth or spontaneous abortion.
Mycoplasma pneumoniae Specifics (walking pneuomnia)
Cytotoxin:
Causes significant cell death and contributes to the pathophysiology of the disease.
Virulence Factors:
Attachment to epithelial cells due to special terminal protein attachment factor that disrupts normal respiratory function and ciliary action or the beating of the cilia.
Symptoms:
Gradual onset of headache, sore throat, chest pain; can culminate in full-blown pneumonia.
Often causes primary atypical pneumonia or walking pneumonia. Atypical means the onset is insidious, not abrupt as with bacterial pneumonias like S. pneumoniae.
Not treatable with penicillin, no cell wall.
Incidence and Diagnosis:
High incidence, especially in young children; diagnosis includes antibody detection and PCR tests.
Pneumoniae caused by this bug is about 20% community acquired. Can be skin lesions called erythema multiforme. Can cause eye infections and lead to stevens johnson syndrome that causes immune system to overreact.
Treatment:
Not treatable with beta-lactams; require antibiotics targeting protein synthesis (e.g., macrolides, tetracyclines). Tetracycline in adults and erythromycin.
Diagnosis :PCR
Mycoplasma Hominis and Genitalium
Diseases:
Mycoplasma hominis linked with pelvic inflammatory disease, vaginitis; can lead to severe complications including spontaneous abortion.
Mycoplasma genitalium associated with non-gonococcal urethritis (NGU) and reproductive complications, prostatitis.
PID is an ascending infection in women 15-25 usually.
Chronis Fatigue Syndrome
Diagnosis for Urogenital Infections:
Similar to pneumonia, PCR is a preferred diagnostic method.
L form Bacteria
Definition: Cell wall-deficient bacteria observed in clinical settings or laboratory. L-form bacteria are cell wall deficient.
Two Types:
Spheroplasts: retain some cell wall, unstable, may revert. These are unstable and can revert to their original morphology.
Protoplasts: lose all cell wall, stable, fragile, no sterols. They are unable to revet to their original morphology.
L form indications are wall-deficient bacterial variants, can produce “part” of the cell wall only, so may be osmotically fragile. No sterols in the cell membrane, so reproduction is stopped by penicillin.
Association with Diseases: Potential involvement in chronic fatigue syndrome and sarcoidosis, highlighting their clinical significance. L-forms may be involved in sarcoidosis, a chronic disease of unknown cause marked by the formation of nodules in the lungs and liver and lymph/salivary glands.
Rickettsia and Chlamydia
General Characteristics of Rickettsia
Type:
Gram-negative, obligate intracellular organisms; small size (0.1 micron), arthropod vector, coccobacillus.
Major Types and Characteristics:
Rocky Mountain Spotted Fever (Rickettsia rickettsii).
Transmission: Via ticks and mites and fleas (dog tick, brown dog tick); causes endothelial cell infection, increased vascular permeability.
Infect endothelial cells.
Symptoms: Fever, rash (starts on wrists and ankles, spreads), possibly progressing to more severe complications. Infection can become more severe, skin necrosis, edema, respiratory issues.
Diagnosis: PCR, tissue, serology.
Treatment: doxycycline, chloramphenicol, macrolides.
Major Rickettsial Infections
Rocky Mountain Spotted Fever:
Seasonal prevalence, especially in southern states; diagnosis via PCR, treated with appropriate antibiotics.
Typhus (Rickettsia prowazekii):
Transmitted by lice in unsanitary conditions; sudden onset of fever and rash.
Rickettsia prowazekii causes typhus.
Epidemic typhus outbreaks occur in areas with poor sanitation, rare.
Murine typhus, from R. typhi comes from fleas, in tropics and subtropics.
Scrub typhus, from Orientia tsutsugamushi is from mites, chiggers, in SE asia, japan, australia.
Diagnosis: PCR
Treatment: doxycyline
Rickettsial Pox (Rickettsia akari):
Mild symptoms; transmitted by mites.
Diagnose with serology.
Treat with doxy.
Coxiella burnetii (Q Fever)
Characteristics: Gram-negative, intracellular, zoonotic infection; resistant to environmental stress; primarily sheep and goats are reservoirs. Shares virulence genes with legionella pneumophila. Highly resistant in environments, Q is “query” fever, contact with animals the aerosols they produce and inhaling. Fever, chills, headache, self-limiting. Can progress to pneumonia, incubates 2-3 weeks, and can develop months to a year after initial infection. Can recover without antibiotics.
Symptoms: Undulating fever, can potentially lead to severe respiratory issues.
Diagnosis and Treatment: PCR tests; generally, the infection is self-limiting.
General Characteristics of Chlamydia
Type: Obligate intracellular parasites, difficult for immune response to target. Gram negative, coccobacillus.
Key Species:
Chlamydia trachomatis: leads to ocular infections and genitourinary diseases, major cause of preventable blindness.
Chlamydia pneumoniae: aerosol transmission, community-acquired pneumonia.
Chlamydia psittaci: associated with birds, leading to respiratory symptoms.
Chlamydia trachomatis
Symptoms and Associations:
Leading cause of blindness and sexually transmitted infections; presents as urethritis, pelvic inflammatory disease.
Higher incidence in women, especially those using oral contraceptives.
Infects epithelial cells of cervix, urethrae, rectum, and conjunctiva. Major cause of blindness worldwide. UTI is most common. STI, higher rate versus gonorrhea.
Risk of transmission per sex is less than gonorrhea, and risk increases with frewuency of sex. Co-infection with gonorrhea is common and increases the risk of transmission.
Urethritis is common in men and has a 7-14 day incubation period with potential burning and discharge along with potential prostate infection.
In women, high rated associated in contraceptive use, most cases asymptomatic, PID in 20%, infertility, ectopic pregnancy, and discharge, bleeding, burning urination and abdominal pain.
Arthritis (reiters syndrome) can occur after infection, infant conjunctivitis, lymph node ulcerative diease, and eye infection (blindness)
TRACHOMA
disease progression conjuctiva= hyperemia and folliculitis
most common cause of preventable blindness
Surgery, antibiotics, facial cleanliness, environment
Neonatal vertical transmission, just like with neisseria.
treat with erythromycin or silver nitrate
pneumonia: gentamicin
LGV (lymphogranuloma Venereum)
sexual
serovars 1.2.3
Ulceration at site of infection, buboes, painful regional lymphadenopathy, proctitis and anorectal pain.
Diagnosis:
Nucleic acid tests (PCR) and serology for infection detection. Culture, NAAT
Treatment:
Doxycycline, erythromycin, azithromycin, ofloxacin
Chlamydophila pneumoniae
Transmission: Aerosol; classified under community-acquired pneumonia.
Treat with doxy, beta lactams dont work. Can use macrolides, fluoroquinolones, and sulfa drugs too.
Clinical Considerations: PCR for diagnosis; treat promptly to prevent complications.
Chlamydia psittaci
Reservoir: Birds, pet birds particularly.
Symptoms: Fever, chills, headache, nonproductive cough; potential for systemic infections.
Diagnosis and Management: Laboratory tests; importance of controlling aviary sources.
Closing Remarks
Final thoughts on the importance of understanding these pathogens for effective diagnosis, treatment, and prevention.
Reminder for students to prepare questions for the follow-up session on Friday at 09:00.
Which of the following micororganisms is not sensitive to penicillin? Mycoplasma Pneumonia is not. However, staph aureas, strep pneum, and L-forms of bacteria are.