ME3 Drugs
NICE: Prescribing in Dental Practice
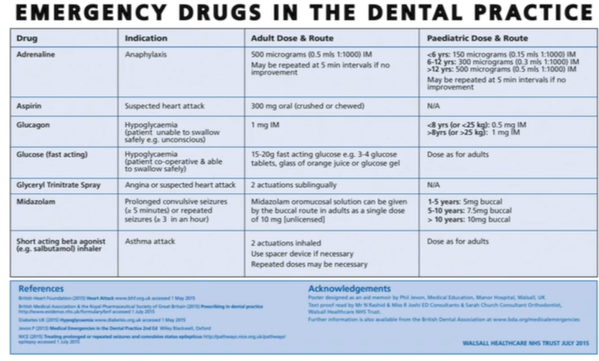
These should be available to manage common medical emergencies:
Adrenaline/epinephrine injection, adrenaline 1:1000 (adrenaline 1mg/mL as acid tartrate), 1mL amps
Aspirin dispersible tablets 300mg
Glucagon injection, glucagon (as hydrochloride), 1-unit vial (with solvent)
Glucose (for administration by mouth)
Glyceryl trinitrate spray
Midazolam oromucosal solution
Oxygen
Salbutamol aerosol inhalation, salbutamol 100um/metered inhalation.
BDA Guidance
Adrenaline
Emeregncy: Anaphylaxis
MOA: alpha-receptor agonist effects reverse peripheral vasodilation and reduce oedema. Its beta-receptor agonist effects dilate the bronchial airways, increase the force of myocardial contraction and suppress histamine and leukotriene release. There are also beta-2 adrenergic receptors on mast cells that inhibit activation and so early adrenaline attenuates the severity of IgE-mediated allergic reactions. Adrenaline seems to be most effective when administered early after the onset of the reaction.
Presentation:
Ampoules: glass ampoules, with both a drawing up filtered needle and a 23g (blue) needle, or in a large patient a 21g (green) needle, for IM injection.
Pre-filled syringe: where possible, adrenaline should be in a pre-filled syringe
Auto-injector device: although it would be reasonable to use an auto-injector device if one is immediately available (i.e. patient’s own device), their routine use by dental practitioners is not recommended as:
They are relatively expensive with a limited shelf life compared with the cost of an ampule of adrenaline, syringe and needle.
Anaphylactic reactions are rare and auto-injectors purchased for dental practices will not be used
Auto-injectors come with a standard-length needle which may not be long enough to administer IM adrenaline for some patients
Most healthcare staff likely to deal with an anaphylactic reaction in the healthcare setting should have the skills to draw up adrenaline and administer IM injections of adrenaline
Dose and route of administration
Adult: 500um IM (repeated if necessary at 5 min intervals according to BP, pulse and respiratory function)
Paediatric: 150-500ug IM
Side effects: include palpitations, dry mouth and tremors. The only reported severe adverse effect following IM administration of adrenaline was a MI in a patient with severe ischaemic heart disease.
Adrenaline from a glass ampoule
Equipment: ampoule, gauze, syringe, 2 needles
Safely break open the glass with gauze
Red needle has a filter (prevents drawing up glass) so it is the drawing up needle (also blunt ended)
Second needle is used for our injection
Aspirin
Emergency: MI
MOA: Aspirin inhibits both platelet actiavtiona dn aggregation. Non-selective COX-1 and COX-2 inhibitors, in platelts COX-1 enzyme produces thromboxane A2 which promtoes plateelt aggregation. Thus, aspirin, by irreversibly inactivating COX-1, blocks the egeneration of thromboxane A2, derives a potential antiplatelet effect, which in turn inhibits thrombus formation
Presentation: soluble apsirin 300mg, either in child proof container or blister pack
Dose and rout of administration: 300mg crushed or chewed (reduced the incidence of reocclusion following thrombolytic therapy)
Side effects: anaphylactic reaction
Contraindications: known allergy to aspirin
Glucagon
Emergency: unconscious hypoglycaemia (blood sugar less than 3.0mmol/L)
MOA: increases the patient’s blood sugar levels by mobilising glycogen in the liver
Presentation: glucagon injection is available as GlucaGen Hypokit. Can be stroed in the fridge or out below 25C for up to 18m within the shelf-life period
Dose and route of administration:
8+ or >25kg = all of syringe (1ml)
<8 or <25kg = half of syringe (0.5ml)
Side effects: nausea, vomiting and temporary fast heartbeat or pounding in your chest (tachycardia)
Contraindications: do not use if allergic to glucagon or lactose, have a tumour of the adrenal gland called pheochromocytoma, or have a tumour of the pancreas called insulinoma.
How to Use Glucagon Injection Kit
Inject liquid of syringe into glass container of powder
Shake and mix around
Draw up liquid
Remove bubbles
Glucose
Emergency: hypoglycaemia (where conscious, cooperative and intact gag reflex)
MOA: blood glucose levels increase, cell function returns
Presentation: solution/tablets/gel/powder
Dose and route of administration: 10-20g of 40% fast-acting glucose, placed inside patient’s cheek and gently rubbed to aid absorption.
GTN
Emergency: angina and suspected MI
MOA: rapidly absorbed through the buccal and sublingual mucosa, reaching peak concentrations at 4 mins. Increases production of NO, which initiates relaxation of smooth muscle to produce arterial and venous vasodilation that results in reduction of venous return and improves myocardial perfusion (reduces work of the heart and therefore oxygen demand)
Presentation: typically comes in pressurised container (typically red) which delivers a metered spray of 400ug.
Dose and route of administration: one or two metered doses (400-800ug) should be given under the tongue while the patient holds their breath. No more than 3 doses at one time. If symptoms have not settled within 5 mins of taking the 3rd dose (15 mins in total from the onset of symptoms) emergency medical services should be contacted.
Side effects: headaches (due to vasodilation), palpitations and hypotension.
Midazolam
Emergency: status epilepticus
MOA: midazolam binds to the GABA receptor but does not displace GABA; rather, it enhances the affinity of GABA for its receptor site on the same receptor complex. The pharmacodynamic consequence of this agonist action is the reduction of seizure activity.
Presentation: oromucosal solution as Buccolam or Epistatus
Buccolam:
Each pre-filled oral syringe:
2.5mg midazolam (as hydrochloride) in 0.5ml solution
5mg midazolam (as hydrochloride) in 1ml solution
7.5mg midazolam (as hydrochloride) in 1.5ml solution
10mg midazolam (as hydrochloride) in 2ml solution
Epistatus - 10mg oromucosal solution
Salbutamol
Emergency: acute asthma attack
MOA: beta-2 adrenergic agonists act on bronchial smooth muscle inducing bronchodilation and relieving bronchospasm
Presentation: pressurised metered dose inhalers (pMDIs)
Dose and route of administration: salbutamol inhaler, 4 puffs (100ug per actuation), through a large-volume spacer, repeat as needed
Side effects: palpitations and tremors. If a severe episode does not respond to treatment within 5 mins, they should be transferred to the hospital as an emergency.