Untitled Flashcards Set
Hepatic, Pancreatic, & Biliary Systems
Signs & Symptoms of Hepatic Disease:
Dark urine and light stools
Skin changes:
Jaundice
Pallor
Orange or green skin
Spider angiomas
Neurologic symptoms, asterixis
Musculoskeletal pain, hepatic osteodystrophy
Portal hypertension, ascites, hepatic encephalopathy
Liver Disease Complications
Jaundice (Icterus)
Common symptom
Yellow discoloration of skin, sclera, mucous membranes
Due to overproduction of bilirubin, liver disease, or bile obstruction
Cirrhosis
Final common pathway of chronic, progressive
inflammation of the liver.
Progressive loss of normal tissue that is replaced with fibrosis and nodular regeneration.
Most common in the US: alcohol abuse and hepatitis C virus (HCV)
If developed, usually not reversible
Signs & Symptoms:
Fatigue
Weight loss
Jaundice
Coagulopathies
Loss of ability to metabolize drugs
Hypoalbuminemia
Portal Hypertension
Increased hepatic sinusoidal pressure (>6mmHg)
Portal: area where blood vessels enter into the liver.
Common cause: cirrhosis
Other causes:
Thrombus
Tumor
Infection
Complications: gastroesophageal varices
Hepatic Encephalopathy
Also known as portosystemic encephalopathy
Complex neuropsychiatric syndrome
Potentially reversible, decreased level of consciousness in people with severe liver disease.
Can occur with both acute and chronic liver disease.
Clinical Manifestations:
Insidious onset
Mild changes in ability to concentrate and complete complex tasks
Progresses: mental status changes become more obvious
Pathogenesis:
Involves increased levels of ammonia and inflammation
Grades of Hepatic Encephalopathy
Grade 0
Nearly asymptomatic, normal level of consciousness.
No detectable personality or behavior changes.
Minimal changes in memory and concentration (e.g., mildly forgetful or confused).
Minimal changes in intellectual function.
Grade 1
Slight personality changes, mood swings (irritability, restlessness).
Short attention span, mild confusion.
Minimal changes in memory and concentration.
Muscular incoordination, impaired handwriting.
Sleep disorders (inverted sleep patterns).
Tremor; asterixis may be observed with clinical testing.
Grade 2
Tremor progresses to asterixis (liver flap).
Resistance to passive movement.
Bilateral numbness/tingling.
Myoclonus; hypoactive deep tendon reflexes.
Apraxia, ataxia.
Slow or slurred speech.
Unusual behavior (abusive, violent, noisy).
Disorientation to time and place.
Grade 3
Hyperventilation.
Marked confusion, amnesia.
Incoherent speech.
Muscle rigidity.
Hyperreactive deep tendon reflexes.
Positive Babinski sign.
Positive Oculocephalic reflex (doll’s eye).
Sleeps most of the time but can be aroused.
Disinhibited (inappropriate) behavior.
Dilated pupils.
Grade 4
Comatose; unresponsive to verbal or noxious stimuli.
No asterixis.
Lack of response to stimuli.
Decerebrate posturing.
Ascites
Abnormal accumulation of fluid within the peritoneal cavity.
Most often caused by decompensated liver cirrhosis
Mechanism: portal hypertension
Hepatorenal Syndrome
Severe complication of advanced cirrhosis
Result of hemodynamics
Two types:
Type 1 rapid (1-2 weeks)
Both in onset and progression to renal failure
Carries a poor short-term prognosis
Type 2
More insidious in onset with slower progression over months
Key features: ascites
HEPATITIS
Chronic Hepatitis
Classified as either chronic persistent hepatitis or chronic active hepatitis
Causes:
Viruses
Medications
Metabolic abnormalities
Autoimmune disorders
Asymptomatic
If symptoms occur:
Nonspecific and mild
Fatigue
Malaise
Loss of appetite
Polyarthralgia
Intermittent right upper quadrant discomfort
Sleep disturbances
Symptoms of advanced disease:
Acute exacerbation
Nausea
Poor appetite
Weight loss
Muscle weakness
Itching
Dark urine
Jaundice
Diagnosis:
Serologic testing
Liver biopsy
Fulminant Hepatitis
(Acute Liver Failure)
Rapidly progressing form of liver inflammation without prior liver disease or cirrhosis.
Develops in 1 to 2 weeks
Rare; 1% of persons with acute viral hepatitis
Causes:
Acetaminophen hepatotoxicity (50%)
Idiosyncratic drug reaction
Infections:
Hepatitis A and B
Epstein-Barr
Cytomegalovirus
Varicella-zoster
Herpes simplex virus
Hepatic ischemia
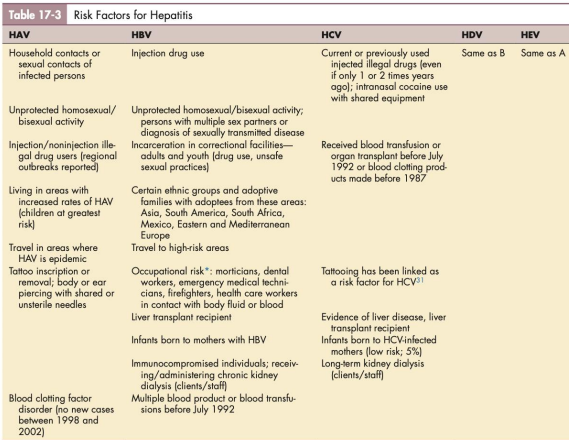
Viral Hepatitis
Incubation period:
HAV: 15 to 50 days
HBV: 1 to 6 months
HCV: 1 week to 6 months
HAV (Hepatitis A Virus)
Formerly known as infectious hepatitis
Transmitted by fecal-oral route
Primarily from poor or improper handwashing and hygiene
Shared use of oral utensils such as straws, silverwares, and toothbrushes
Commonly affects children, sexual activities with the same gender, people who live or travel in underdeveloped countries
Rarely transmitted through transfused blood
Highly contagious
Greatest danger of infection: incubation period, when a person is unaware that the virus is present
Illness can last from 4 to 8 weeks
Last longer and more severe in persons older than 50 years
HBV (Hepatitis B Virus)
Transmitted percutaneously or mucosal contact
Highly infectious (100 times infectious than HIV)
Can be transmitted through heterosexual or homosexual intercourse (considered to be a sexually transmitted disease)
HCV (Hepatitis C Virus)
Formerly posttransfusion non-A, non-B hepatitis
Most commonly associated with injection-drug use
Period of infectivity: before the onset of symptoms
May become a lifetime carrier of the virus
HDV (Hepatitis D Virus)
"Delta virus"
Defective single-stranded RNA that presents as a coinfection or superinfection of HBV
Requires hepatitis B surface antigen (HBsAg) for its replication
Symptoms are similar to those who have HBV
HEV (Hepatitis E Virus)
Previously known as enteric non-A, non-B hepatitis
Transmitted by contaminated water via fecal-oral route
Clinically resembles HAV
Travel-associated, acute, self-limiting liver disease
Occurs in poor socioeconomic conditions
HGV (Hepatitis G Virus)
Accepted term: GBV-A and GBV-B
GBV-B:
Most prevalent in African countries
Identified as the causative agent of approximately 20% of posttransfusion hepatitis cases
Clinical Manifestations
Most acute viral hepatitis are asymptomatic
Classic symptoms:
Malaise
Fatigue
Mild fever
Nausea
Vomiting
Anorexia
Right upper quadrant discomfort
Diarrhea
Jaundice (except acute HCV)
Dark urine
Clay-colored stools
Extrahepatic manifestations
Medical Management
Prevention (primary, secondary, tertiary)
Primary: Education, practicing protective sex or avoiding sexual contact during the period of HBsAg
Secondary: Passive immunization, travel precautions
Tertiary: Education to those infected
Diagnosis: Serology (standard)
PANCREAS
Pancreatitis
Serious inflammation of the pancreas
Acute Pancreatitis
Most common cause: gallstones
Symptoms: Pain, nausea, anorexia, vomiting
Complications: Pancreatic fluid-filled collections, pseudocysts, necrosis
Chronic Pancreatitis
Cause: Chronic alcohol consumption
Symptoms: Abdominal pain, decreased appetite, weight loss
Biliary Disorders (Gallbladder & Bile Ducts)
Cholelithiasis (Gallstone Disease)
Common: 20-35% of people by age 55
Types:
Cholesterol stones (80%)
Bilirubin salts (20%)
Risk Factors: Obesity, pregnancy, women > men
Symptoms:
Pain (RUQ, radiates to right shoulder/back)
Nausea, vomiting, belching, food intolerance
Complications:
Choledocholithiasis: gallstones in the common bile duct
Pancreatitis, cholangitis
Cholecystitis
Inflammation of the gallbladder (gallstone obstruction)
Acute Cholecystitis: more common in older men
Acute Cholangitis
Biliary tree infection
Stages:
Mild (Grade I): responds to therapy
Moderate (Grade II): needs further treatment
Severe (Grade III): organ dysfunction
Symptoms:
Charcot’s Triad: fever, jaundice, right upper quadrant pain
Reynold’s Pentad: Charcot’s Triad + hypotension, confusion
Primary Sclerosing Cholangitis
Progressive bile duct destruction (intrahepatic & extrahepatic)
Common in ages 20-40, often asymptomatic
Symptoms: jaundice, itching, fatigue, anorexia, weight loss
Severe complications: Cirrhosis, portal hypertension
Key Takeaways
Liver diseases involve metabolic dysfunction, jaundice, and severe complications like cirrhosis, portal hypertension, hepatic encephalopathy.
Hepatitis can be viral, autoimmune, or drug-induced, with HAV, HBV, HCV being the most common.
Pancreatic diseases include pancreatitis, which is often alcohol- or gallstone-related.
Biliary diseases involve gallstones, cholecystitis, cholangitis, and progressive bile duct damage (sclerosing cholangitis).