2/2/26 Lec 2
EXS 326: Pre-participation Screening and Informed Consent in Exercise Testing and Prescription
Review of Guidelines for Physical Activity
Aerobic Physical Activity Guidelines:
Overview of guidelines and their current adherence:
Guidelines should promote health benefits and exercise safety.
Strength Training Physical Activity Guidelines:
Similar to aerobic guidelines, need to assess adherence and effectiveness.
Variables in Lab Reports:
It is essential to recognize:
Independent vs. dependent variables.
Units of Measurement:
Length
Time
Mass
Distance
Volume
Importance of Screening
Core Responsibility:
As exercise/fitness professionals, the motto is “DO NO HARM.”
Risk Understanding:
Key for exercise prescription.
Steps to understand risk:
Assess need for further evaluation/clearance for exercise.
Identify necessary special considerations in exercise programming.
Develop an appropriate progression plan for exercise.
Communication with Patients/Clients
Understanding Potential Health Risks:
Gathering information requires two components:
Self-Reported Feedback:
Often initiated by questionnaires.
Direct Testing:
Resting measures (e.g., Heart Rate (HR), Blood Pressure (BP)).
May include exercise tests.
Importance of clear communication of rights and purposes of procedures.
Informed Consent in Exercise Testing
Definition and Purpose:
Informed consent involves communicating costs and benefits of tests/procedures.
Essential in research and medical contexts, applicable to exercise testing.
Elements of Informed Consent:
Detailed statement of testing process and objectives.
Clear description of testing procedures in understandable terms.
Risks and benefits of participation should be well-defined.
Right to ask questions and withdraw at any time without consequences.
Assurance of confidentiality in testing.
Learning About Clients/Patients
Pre-Participation Screening Questions:
Medical Clearance Needs:
Identification of individuals needing authorization for initiation or increased frequency/intensity of exercise.
Medical Condition Assessment:
Awareness of conditions that require supervised exercise.
Consideration for exercise restrictions until health improves.
Screening Depth:
Adjust depth of screening based on population (health status).
Healthy individuals need less rigorous screening than those with known health issues.
Initial Screening Components
Key initial screening elements include:
Assessment of the individual's current activity level.
Examination for signs/symptoms of cardiovascular disease (CVD), metabolic syndrome (MetS), or renal dysfunction.
Identifying known cardio-metabolic diseases.
Establishing the individual's goals for the exercise program.
Physical Activity Readiness Questionnaire for Everyone (PAR-Q+)
Definition and Purpose:
PAR-Q+ is a quick screening tool for medical clearance for physical activity.
Safe for pre-screening individuals for low to moderate physical activity.
Structure of PAR-Q+:
Comprises 7 questions aimed at clearing individuals for participation.
If any question elicits concerns, follow-up questions provide further clarification on the need for exercise.
Updates to PAR-Q+ in 2023
If all answers are “NO,” individuals can be considered safe to begin moderate-intensity physical activity.
A “YES” response to any question triggers additional 10 multi-part questions for further evaluation.
PARmed-X
Definition:
PARmed-X is a tool for additional assessment if an individual has any risk indicators on the PAR-Q+.
Utility:
Designed to evaluate whether a “YES” on PAR-Q+ is an acceptable risk and is commonly used in fitness centers.
Emphasizes the need for more rigorous screening when working individually with clients.
ACSM’s Risk Stratification
Logic Model for Exercise Preparticipation Health Screening:
Visualization outlined for assessing participation in aerobic exercise.
Regular Exercise Participation Definition:
Defined as performing structured physical activity for a minimum of 30 minutes at moderate intensity on at least three days a week for at least the last three months.
Exercise Intensity Categories:
Light-Intensity Exercise: 30% to <40% Heart Rate Reserve (HRR) or VO₂ Reserve, typically rated 9-11 on the Rate of Perceived Exertion (RPE) scale.
Moderate-Intensity Exercise: 40% to <60% HRR or VO₂ Reserve, generally rated 12-13 on the RPE scale.
Vigorous-Intensity Exercise: ≥60% HRR or VO₂ Reserve, measured as ≥6 METs, typically rated ≥14 on the RPE scale.
Screening Logic for Exercise Participation
Criteria include consideration of clinical conditions and symptomatology to guide the need for medical clearance.
Medical clearance is recommended for individuals with known cardiovascular, metabolic, or renal disease who exhibit symptoms regardless of disease status.
Key Changes in Screening Practices
Empowerment of Individuals:
The modern screening protocol suggests that most individuals can exercise without needing prior physician consultation.
Points for Consideration Before Exercising:
Current activity level, signs, and symptoms indicative of diseases, and planned exercise intensity play pivotal roles.
Fitness Program Decision-Making Post-Screening
Referrals to Physicians:
Needed for consent or medical consultation to uphold safety principles.
Programs in fitness facilities may necessitate adaptations based on individual evaluations, even in participants deemed fit to exercise.
Educational Requirements:
Provision for educational workshops, seminars, or referral options based on clients’ specific conditions.
Progressing into Fitness Programs
Medical Clearance Protocol:
Immediately refer individuals needing medical clearance to rigid protocols post-authorization.
Clients without clearance but facing other concerns (like special needs) may require additional education or specialized referrals.
Determining Necessary Exercise Supervision
Edge Cases Requiring Close Monitoring:
Include various medical conditions such as:
Alcoholism, anemia, asthma, cancer, diabetes, hip and knee surgeries, and other chronic concerns.
Condition control may necessitate a closer supervisory approach during exercise.
Summary of Key Responsibilities
Fundamentals of Risk Assessment:
The primary responsibility remains to ensure client safety through effective risk assessment and management.
Client-Focused Evaluation:
Determine the necessity for medical clearance and special exercise programming considerations, focusing primarily on potential risks.
Metabolic Syndrome Overview
Definition:
A combination of individual cardiovascular and metabolic risk factors that predispose individuals to diseases such as CVD and Type 2 Diabetes Mellitus (T2DM).
Diagnostic Criteria for MetS:
An individual must exhibit at least three of the following risk factors:
Fasting plasma glucose ≥100 mg/dL.
HDL cholesterol ≤50 mg/dL (women) or ≤40 mg/dL (men).
Fasting triglycerides ≥150 mg/dL.
Waist circumference >88 cm (women) or >102 cm (men).
Systolic BP ≥130 mmHg or Diastolic BP ≥85 mmHg.
Lifestyle Factors Influencing MetS
Significant Factors:
Physical inactivity and unhealthy dietary habits are influential in developing MetS.
Exercise Implications for Abdominal Obesity and Hyperglycemia
Obesity Assessment:
Measured via BMI (>30 categorized as obese) and body composition standards, which vary by gender.
Different body shapes (Pear, Apple etc. search). Waist circumference (part of shape) is crucial for evaluating abdominal adiposity.
Exercise Benefits:
Exercise diminishes acute blood glucose levels and enhances insulin sensitivity effectively over time.
Dyslipidemia and Exercise
Definition of Dyslipidemia:
Characterized by abnormal lipid concentrations in the blood, linked with increased CVD risk.(varieus lipids)
Impact of Exercise, Diet, and Genetics:
Regular exercise usually results in lowered triglyceride levels and elevated HDL cholesterol levels over time.
some drugs manage lipid levels (47million) use to statin medication to lower LDL
Recommended Goals for Lipid Levels:
LDL cholesterol: <100 mg/dL ← Chol carried by Apo B100
HDL cholesterol: >50 mg/dL (females) or >40 mg/dL (males) ← Chol carried by Apo B
Total cholesterol: <200 mg/dL ← All Chol in the system
Triglycerides: <150 mg/dL ← Triglycerides(not FFAs)
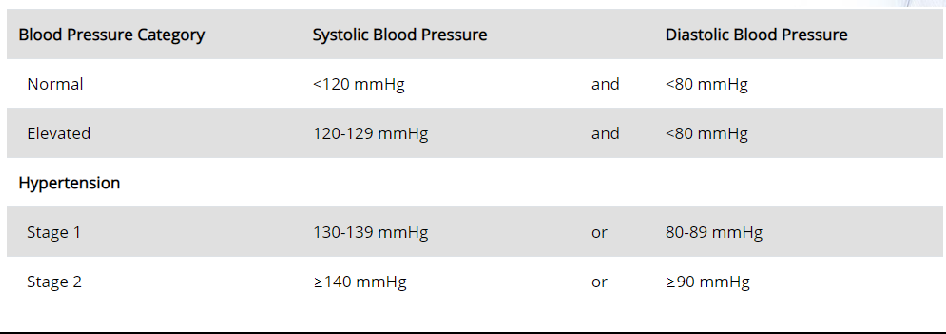
Hypertension and Exercise
Hypertension Defined:
High resting blood pressure, a significant risk factor for heart events.
Effected by → Diet, exercise & genetics.
Increases risk of → MI, Stroke, aneurysm, arterial dissection
Exercise raises MAP → driven by increase in SBP usually no change in DBP
Therefor no concern for exercises with HTN because BP is already elevated
Special Considerations in Exercise Testing (slides)
Higher Risk with MetS in Exercise Testing:
Individuals may need thorough medical evaluations before participating in exercise due to potential underlying conditions.
Exercise will improve Metabolic syndrome , but they need more medical evaluation/screening before (CVD, Diabetes, CKD, S/Sx’s)
Considerations for HTN Participants:
Resting blood pressure levels will influence the safety and effectiveness of exercise testing.
Exercise Prescription for Obesity
Guidelines:
Frequency: ≥5 days/week
Intensity: Moderate to vigorous based on individual capacity.
Time: 30-60 minutes daily or aiming for 250-300 minutes/week.
Type: Aerobic exercise of any modality should be emphasized (although history or risk of orthopedic injury should be considered)
Resistance training → 2-3 non-consecutive days
moderate intensity (8-12 reps to failure for 2-4 sets for each major muscle groups)
Flexibility training → 2-3 days/week static stretching
Exercise Prescription for Hypertension
Guidelines:
Frequency: 5-7 days/week
Intensity: Moderate, adjusted based on fitness level.
Time: ≥30 minutes/day.
Type: Aerobic exercise of any modality should be emphasized
Emphasis on aerobic activities while including resistance training (2-3 days nonconsecutive )
Flexibility Training:
Advised 2-3 days/week (static)
Exercise Prescription for Dyslipidemia
Key Points:
Frequency: ≥5 days/week with emphasis on aerobic activities.
Intensity: Moderate levels, adjusted for individual fitness.
Time: 30-60 minutes daily, where longer sessions can help achieve weight loss.
Type: Aerobic exercise of any modality should be emphasized
Resistance training: 2-3 nonconsecutive days
Moderate intensity: 8-12 repetitions to failure (2-4 sets for major muscle groups)
Flexibility: 2-3 days/week static stretching
Exercise Impact on MetS Criteria
Overall Effects of Exercise on MetS:
While not substitutive for pharmacological treatments, exercise frequently produces ancillary health benefits like improved body composition and cardiovascular fitness (Fasting Glucose, HDL, SBP, Waist circumference, DBP, TAG)
Common Concerns in Pre-Participation Screening
Activity Level Assessment:
Treat as binary; categorize as active or sedentary.
Monitoring Signs/Symptoms:
Pay attention to RED FLAGS (e.g., chest pain, excessive breathlessness), indicating the need for cessation and medical referral.
Cardiometabolic Risk Factors
Definition and Importance:
Encompasses physiological, genetic, and behavioral factors linked to cardiovascular and metabolic diseases. These don’t prevent anyone from exercising, but lean on side of caution
Non-Modifiable Risk Factors:
Family history, risk increase w age, sex, and ethnicity influence the predisposition.
Modifiable Risk Factors:
Includes obesity, hypertension, blood glucose/lipid levels, smoking, physical activity, and dietary habits.
Case Studies for Application
Case Study 1:
55-year-old male with risk factors including obesity and family history of heart disease.
Current exercise history shows moderate risk; clearance not necessary for moderate activities.
Case Study 2:
40-year-old female with light-headedness during exertion and sporadic exercise history; medical clearance warranted.
Case Study 3:
36-year-old male with no evident risks; eligible to maintain moderate to vigorous exercise.
Case Study 4:
50-year-old male with a history of cardiac events; medical clearance essential for increased intensity pursuits.
Case Study 5:
22-year-old female, currently non-exercising with no symptoms; medical clearance unnecessary given current health status.
Conclusion
The primary goal remains to ensure patient safety through effective risk assessment.
Addressing potential complications arising from MetS, dyslipidemia, or hypertension is essential in mitigating risks during exercise.
Upcoming Class and Assignments
Next Class: 2/9 focusing on general principles & measures of Exercise Prescription (ExRx: HR, BP, SpO2, RPE).
Assignments:
Discussion Board #2 due by 2/8.
Case Study #1 due by 2/8.
Questions can be directed to: alexander.pinero@lehman.cuny.edu