Emergency, Terrorism, Disaster Nursing and Eye Trauma
Goal: Apply sequential steps in triage, primary survey, and secondary survey to emergency patients; differentiate MCI triage tags; manage face/eye trauma; understand ethical/practical implications.
Objectives
Apply sequential steps for emergency patient triage, primary, and secondary surveys.
Differentiate MCI triage tags.
Apply correct steps for face and eye trauma.
Integrate ethical, practical, and real-world considerations.
Emergency Department Context & EMTALA
EDs face rapid changes, high risk for errors, and require multispecialty care in often crowded, noisy, potentially hostile environments.
EMTALA: Requires medical screening exams, emergency services, and stabilizing treatment for all, regardless of ability to pay; restricts patient transfers.
Collaborative Teams
Includes prehospital (EMS), ED physicians, nurses (BLS, ACLS, PALS, TNCC certified), and various support staff and specialists.
ED Visits & Crowding
Rising ED visits are due to poor outpatient access, aging population, shorter hospital stays, mental health crises, and insurance gaps, leading to overcrowding and delayed care.
Emergency Nurses Association (ENA)
Advances emergency nursing, provides care standards, and certifies Emergency Nurses (CEN).
Care of the Emergency Patient: Core Concepts
Early recognition of life-threatening issues.
Rapid intervention to prevent/reverse crises.
Prompt identification of patients needing immediate treatment.
Nursing Roles
Assessment, triage, primary/secondary surveys, standing orders, provider assessment, disposition, and client/family teaching.
Triage: Concept & System
"To sort" patients rapidly by acuity, treating life threats first.
5-level Emergency Severity Index (ESI): Assigns priority based on illness severity and resource use.
ESI-1: Immediate, life-threatening intervention.
ESI-2: High-risk/severe pain, rapid assessment.
ESI-3: Stable, requires resources, not immediately life-threatening.
ESI-4: Stable, minor resources, non-urgent.
ESI-5: Minimal workload, no resources.
Primary Survey (ABCDE)
Focuses on identifying and intervening in life-threatening conditions.
If uncontrolled hemorrhage, prioritize C (catastrophic hemorrhage) first.
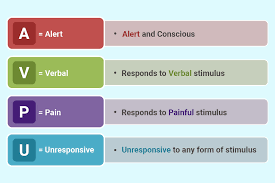
A: Alertness & Airway (AVPU): Assess LOC to guide airway management.
B: Breathing: Identify compromised breathing, provide supplemental O2; may need BVM, decompression, intubation.
C: Circulation: Assess central pulses, skin, mental status; prepare for large-volume resuscitation (two large-bore IVs).
D: Disability (Neurologic Status): Brief neuro exam, GCS, pupil assessment.
E: Exposure & Environmental Control: Remove clothing for thorough exam (preserve forensic evidence); warm patient to prevent hypothermia; do not remove impaled objects.
F: Full Set of Vitals & Family Presence: Obtain vitals (BP in both arms for chest trauma); facilitate family presence during resuscitation.
G: Get Resuscitation Adjuncts (LMNOP):
L = Lab tests
M = Monitor ECG
N = Nasogastric tube (or orogastric for head/facial trauma)
O = Oxygenation & ventilation assessment
P = Pain assessment & management.
Secondary Survey: Head-to-Toe to Identify ALL Injuries
Aims to identify all injuries after initial stabilization.
H = History (SAMPLE) & Head-to-Toe Assessment:
S = Symptoms
A = Allergies/tetanus
M = Medications
P = Past Medical History (PMH)
L = Last meal/oral intake
E = Events leading to injury.
Head-to-Toe Assessment: Covers head, neck, face, chest, abdomen, pelvis, perineum, extremities.
Key: Protect C-spine, stabilize impaled objects, assess for bruising/deformities, check pulses, assess for compartment syndrome.
I = Inspect Posterior Surfaces: Logroll with C-spine immobilization to inspect the back and palpate the spine.
Acute Care & Evaluation
Tetanus prophylaxis, ongoing monitoring, diagnostic testing, and disposition planning.
Death in the ED
Provide privacy/comfort for families, chaplain support, notify medical examiner/coroner, and organ procurement organization.
Agents of Terrorism
Biologic (anthrax, smallpox), chemical (nerve gas like sarin), radiologic/nuclear (acute radiation syndrome), and explosive devices.
Bioterrorism education (4-hour CEU) is mandated for nurses for license renewal.
Mass Casualty Incidents (MCI): Tagging & Triage
Triage Tags:
Green = minor
Yellow = urgent, non-life-threatening
Red = life-threatening, immediate intervention
Black = deceased/expected to die.
Triage in 15 seconds per person; decontamination if applicable.
Hospitals need emergency response plans and Community Emergency Response Teams (CERTs).
Eye Trauma: Emergency Management
Etiology: chemical, foreign bodies, thermal burns, trauma.
Key steps: Assess tissue integrity, visual field, drainage.
Eye Trauma: Nursing Management
Determine mechanism/exposure; irrigate for chemical exposure; do not apply pressure or remove impaled objects; cover injured eye; elevate head of bed.
Ethical, Philosophical, & Practical Implications
Balance patient autonomy vs. triage efficiency, family presence in resuscitation, forensic considerations, resource allocation, healthcare worker safety, and bioterrorism readiness.
Quick Reference Mnemonics & Key Points
ESI: (threat to life to minimal workload).
ABCDEFG: Airway, Breathing, Circulation, Disability, Exposure, Full vitals, Get resuscitation adjuncts.
AVPU: Alert, Voice, Pain, Unresponsive.
LMNOP: Labs, Monitor ECG, Nasogastric tube, Oxygenation, Pain management.
SAMPLE: Symptoms, Allergies, Meds, PMH, Last meal, Events.
Logroll for posterior exam with C-spine immobilization.
MCI tags: Green, Yellow, Red, Black.
Final Takeaways
Mastery of primary/secondary surveys and ESI triage is critical.
Ethical considerations are integral to practice.
Eye trauma requires careful assessment and injury prevention.
MCI preparedness relies on teamwork, protocols, and ongoing education.