Traditional, Complementary & Alternative Medicine: Notes for Exam Preparation
Defining and Attitudes to Traditional, Complementary & Alternative Medicine (TCAM)
Definitions of TCAM Components:
Traditional vs. Modern: Distinguishes between historical, culturally ingrained practices and contemporary, scientifically developed approaches.
Conventional vs. Alternative: Differentiates mainstream medical practices from those outside the dominant healthcare system.
Western vs. Eastern: Highlights geographical and philosophical origins of medical systems.
Science vs. Pseudoscience: Challenges the scientific validity and evidence base of certain practices.
Attitudes Towards TCAM:
"Quackery" & Pseudoscience: Often viewed skeptically due to lack of scientific evidence.
Medicine Works - If it Doesn't Work it's Not Medicine: A critical stance suggesting effective treatments are inherently scientific.
Alternative Implies Effective Alternative: Suggests that if something is 'alternative,' it should offer a viable, effective substitute for science-based medicine.
Complementary Implies Boosting Effectiveness: Indicates that 'complementary' treatments are expected to enhance the efficacy of science-based medicine.
No Universal Defining Quality: As Kate Chatfield (2018) notes, there's a perceived shared understanding of these terms, yet no single quality applies to all types of TCAM.
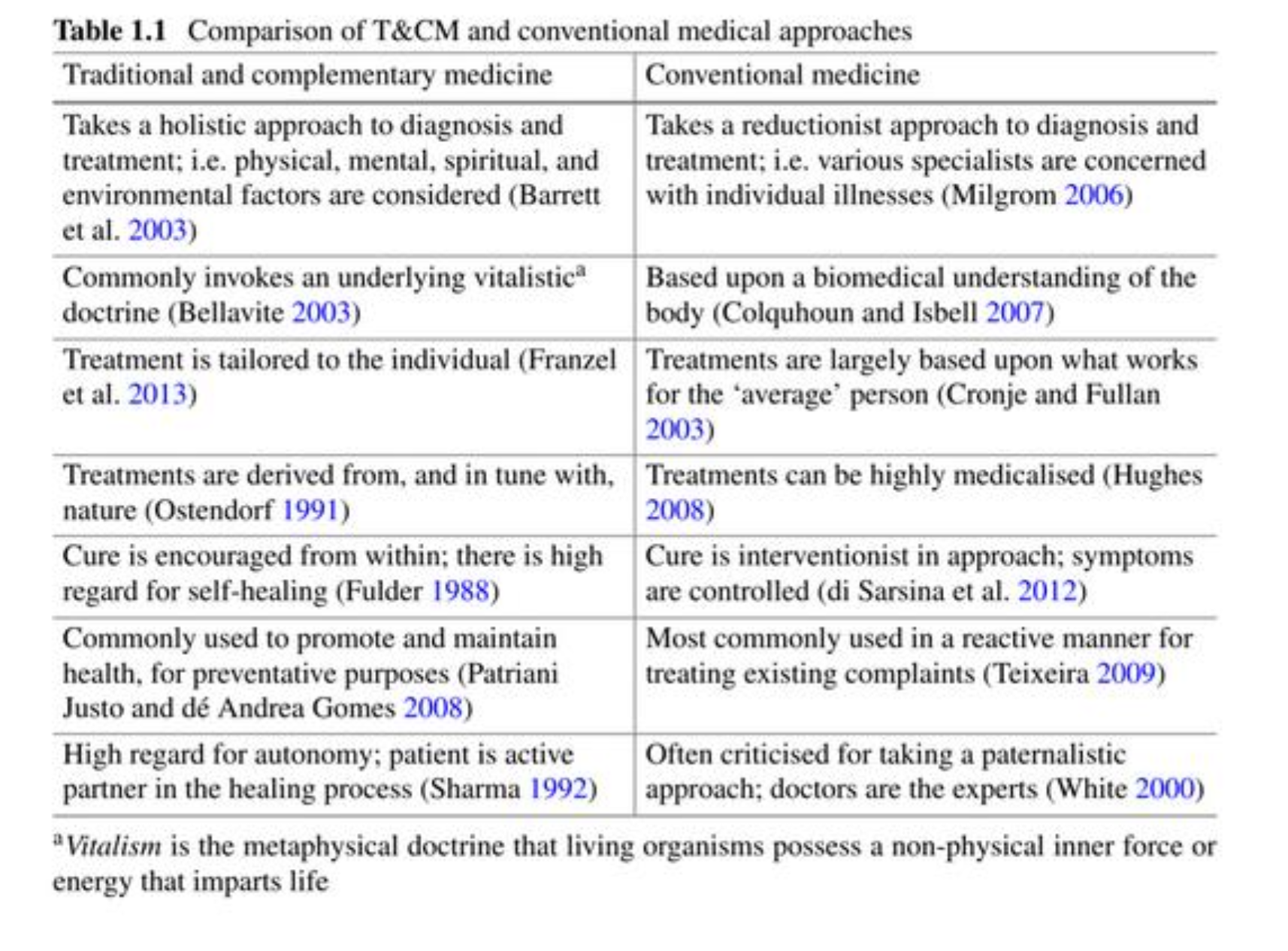
Comparison of T&CM and Conventional Medical Approaches
Traditional and Complementary Medicine:
Holistic Approach: Diagnosis and treatment consider physical, mental, spiritual, and environmental factors (Barrett et al. 2003).
Vitalistic Doctrine: Commonly invokes an underlying non-physical inner force or energy that imparts life () (Bellavite 2003).
Individualized Treatment: Tailored to the unique needs of the individual (Franzel et al. 2013).
Nature-Derived Treatments: Derived from and in tune with nature (Ostendorf 1991).
Self-Healing Emphasis: Encourages cure from within, with high regard for the body's self-healing capabilities (Fulder 1988).
Preventative Focus: Commonly used for health promotion, maintenance, and prevention (Patriani Justo and dé Andrea Gomes 2008).
Patient Autonomy: High regard for patient autonomy, making the patient an active partner in healing (Sharma 1992).
Conventional Medicine:
Reductionist Approach: Diagnosis and treatment are reductionist, with specialists focusing on individual illnesses (Milgrom 2006).
Biomedical Understanding: Based upon a biomedical understanding of the body (Colquhoun and Isbell 2007).
Averaged Treatments: Treatments are largely based on what works for the 'average' person (Cronje and Fullan 2003).
Medicalized Treatments: Treatments can be highly medicalized (Hughes 2008).
Interventionist Cure: Cure is interventionist, focusing on controlling symptoms (di Sarsina et al. 2012).
Reactive Use: Most commonly used reactively for treating existing complaints (Teixeira 2009).
Paternalistic Approach: Often criticized for a paternalistic approach, where doctors are seen as the sole experts (White 2000).
Professional Ethics Regarding TCAM
Widespread Use: TCAM therapies are widely available and increasingly utilized by the public.
Requests for Advice: Professionals may be asked for advice on TCAM.
Treating Patients Using TCAM: Professionals may need to treat patients who are concurrently using TCAM.
Obligation to Sell: In some contexts, professionals may be obliged to sell TCAM products.
Personal Practice: Professionals might choose to practice a TCAM modality themselves.
Personal Beliefs vs. Professional Behavior: A critical ethical question arises regarding the extent to which personal beliefs should influence professional conduct when dealing with TCAM.
Criticisms and Safety Concerns of TCAM
Use of Endangered Species: Some traditional practices involve the use of endangered species, raising ethical and environmental concerns.
Safety Concerns: The World Health Organization (WHO) highlights that "inappropriate use of traditional medicines or practices can have negative or dangerous effects."
Need for Research: The WHO emphasizes that "further research is needed to ascertain the efficacy and safety" of such practices and medicinal plants.
WHO Strategy: In response, the WHO has implemented a nine-year strategy to support Member States in developing proactive policies to strengthen the role of traditional medicine in population health, focusing on appropriate integration, regulation, and supervision.
The Placebo Effect
Definition: Occurs when a person's physical or mental health appears to improve after receiving a placebo (dummy treatment).
Scientific Basis: Science demonstrates that placebos:
Brain Modulation: Work best on symptoms modulated by the brain, such as pain management, stress-related insomnia, and cancer treatment side effects (e.g., fatigue and nausea).
Neurobiological Reaction: Involve a complex neurobiological reaction, including increases in "feel-good" neurotransmitters (e.g., endorphins and dopamine) and greater activity in brain regions linked to moods, emotional reactions, and self-awareness.
Ritual of Treatment: Necessitate the ritual of treatment, incorporating elements of conditioning and expectation to be effective.
WHO Traditional Medicine Strategy
Importance of TCAM: Recognized as an important and often underestimated part of healthcare, with increasing global demand.
Goal: To ensure that all people have access to safe, respectful, cost-efficient, and effective care, including Traditional Medicine (TM) of proven quality, safety, and efficacy.
Integrative Approach: Many countries acknowledge the need for a cohesive and integrative approach to healthcare, enabling governments, practitioners, and users to access TCAM appropriately.
Three Strategic Sectors:
Build Knowledge Base: Develop national policies that understand and recognize the role and potential of TCAM.
Strengthen Quality Assurance & Safety: Regulate products, practices, and practitioners through education, training, skills development, services, and therapies.
Promote Universal Health Coverage: Integrate TCAM services into health service delivery and self-health care, capitalizing on their potential to improve health outcomes and enable informed choices.
Areas Identified by WHO for TCAM Development
Safety and Efficacy
Education and Training of Practitioners
Regulation of Practices
Intellectual Property
Research and Development
Integration into Health Systems
Growing Economic Importance
WHO Definitions: Traditional and Complementary Medicine
Traditional Medicine (TM):
Has a long history.
Defined as the sum total of knowledge, skills, and practices based on theories, beliefs, and experiences indigenous to different cultures, whether explicable or not.
Used for health maintenance, prevention, diagnosis, improvement, or treatment of physical and mental illness.
When adopted outside its traditional culture, it is often referred to as "complementary and alternative medicine."
Complementary Medicine (CM) / Alternative Medicine (AM):
Refers to a broad set of healthcare practices not part of a country's own tradition or conventional medicine.
Not fully integrated into the dominant healthcare system.
Used interchangeably with traditional medicine in some countries.
An Australian Perspective on CAM
National Health and Medical Research Council Act 1992 (NHMRC):
Responsibility: Inquires into, issues guidelines on, and advises the community on health improvement, disease prevention/diagnosis/treatment, healthcare provision, public health/medical research, and ethical health issues.
Evaluation Mandate: States that all health treatments (conventional, traditional, complementary) should undergo rigorous evaluation for effectiveness.
CAM Initiatives: Has committed since to building the evidence base for CAM through stimulating research and aiming to strengthen integration.
Broadened Focus (2012-2015): Ensured all health treatments are subject to rigorous evidence evaluation and funded investigator-driven CAM research.
Therapeutic Goods Administration (TGA):
Definition: Defines "complementary medicines" (also known as 'traditional' or 'alternative') to include vitamin, mineral, herbal, aromatherapy, and homeopathic products.
Regulation: Complementary medicines may be either listed or registered, depending on their ingredients and the claims made.
What is Modern Medicine?
Terminology: Also referred to as contemporary medicine, Western medicine, science-based medicine, or allopathic medicine.
Treatment Focus: Aims to treat or prevent disease, primarily through pharmacologically active agents, physical interventions (e.g., surgery), and other therapies (e.g., psychotherapy, medical devices, ionizing radiation).
Historical Origins: While human disease treatment has a long history, modern medicine is generally considered to have developed from advances in the and centuries, driven by industrial and scientific progress.
Evidence and Empirical Evidence
Definition of Evidence: (Collins dictionary, )
Ground for belief or disbelief; data for proof or establishing truth/falsehood.
A mark or sign that makes evident; indication.
Legal matter presented in court to prove or disprove a point.
Evidence in Science: Meaning varies, but in science, there is reliance on empirical evidence.
Empirical Evidence: Information acquired by observation or experimentation.
Experimentation vs. Observation: Experimentation is generally prioritized over mere observation due to its controlled nature.
Challenge to TCAM: The question arises whether TCAM approaches, often based on hundreds of years of observation, can be considered scientific or evidence-based if they lack formal experimentation.
What is Evidence-Based Medicine (EBM)?
Historical Context: Prior to EBM, clinical decision-making was largely subjective, relying on individual practitioners' research interpretation, personal experience, and beliefs.
Movement in 1960s-1970s: A movement emerged questioning clinical reasoning, identifying practitioner biases, and noting the lack of controlled trials for many 'effective' treatments.
Clinical practice was seen as the "art of medicine," based on expert opinion, experience, and authoritarian judgment. Scientific methodology and statistical analysis were rare (Sur & Dahm, ).
Coined Term (1990s): The term EBM was coined to describe a new, systematic approach to clinical decision-making.
Components of EBM:
Best Research Evidence
Clinical Experience
Patient Values & Preferences
Criticism of EBM: Some critics suggest that its emphasis on randomized trials has limited usefulness for individual patients, though evidence is considered one of several considerations alongside clinical experience and an individual's unique situation.
Evaluating Clinical Data
To evaluate clinical data, typically four factors are considered:
The Level of Evidence: What type of study was conducted?
The Quality of the Evidence: How well was the study conducted?
The Relevance of the Evidence: How applicable is the evidence to the specific question at hand (not covered in detail here).
The Strength of the Evidence: The magnitude of the effect and confidence in that effect.
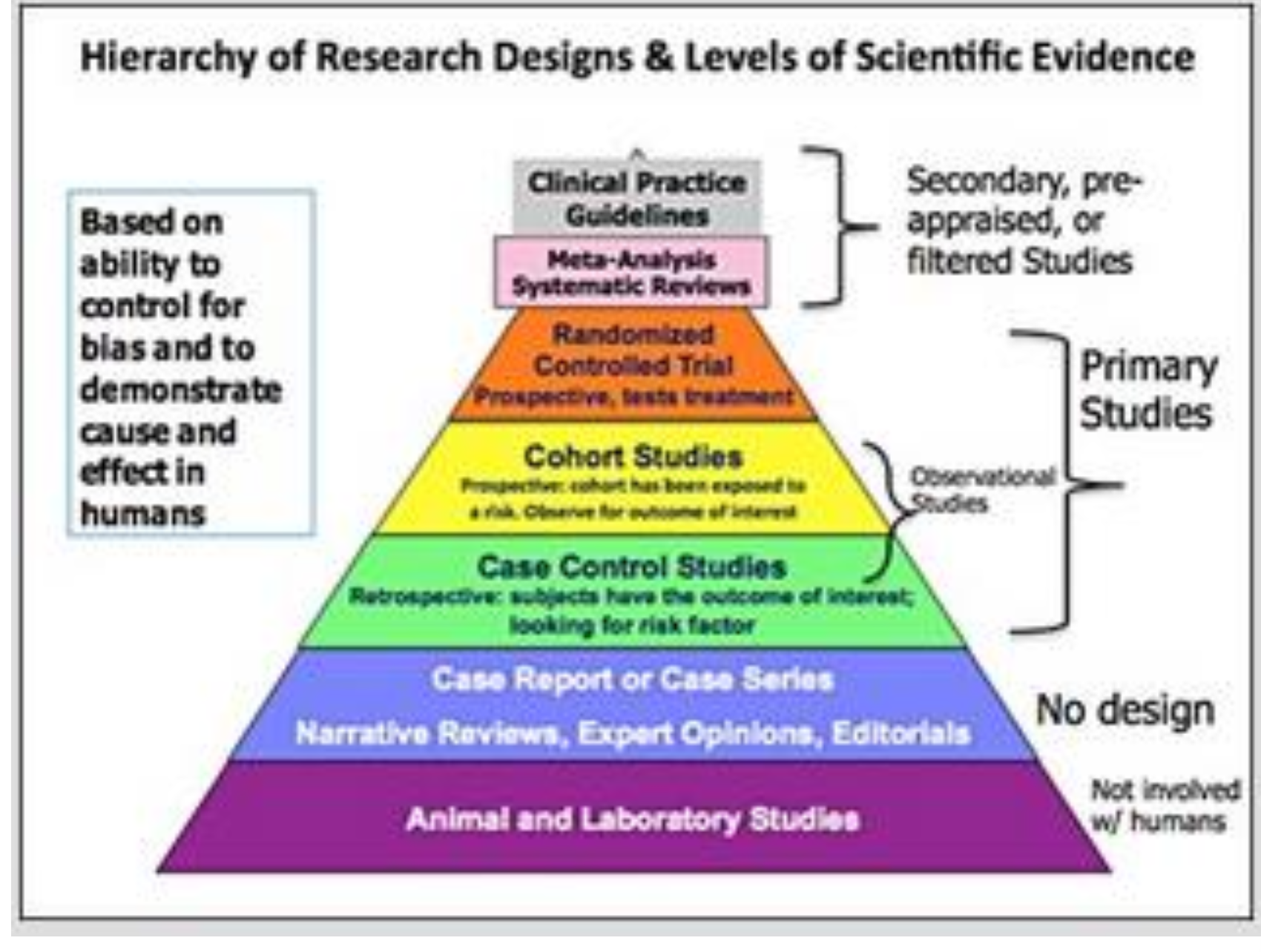
The Level of Evidence: Study Types
Hierarchy of Study Designs: A well-established hierarchy exists for clinical interventions, often represented as a pyramid with the most biased designs at the base and least biased at the top.
Classifications:
Observational Studies: (More prone to bias)
Case Reports
Case-Control Studies
Cohort Studies
Experimental Studies: (Less biased)
Randomized Controlled Trials (RCTs)
Analytical Studies: (Investigate causes/associations)
RCTs
Cohort Studies
Case-Control Studies
Descriptive Studies: (Describe occurrences)
Case Reports
Case Series
Primary vs. Secondary Studies: Primary studies collect new data, while secondary studies synthesize existing data (e.g., systematic reviews, meta-analyses).
The Quality of the Evidence
Assessment: Typically based on how well research methods prevent results from being affected by bias and confounding factors.
Confounding Factors: Patient features and other possible causal factors that can influence the study outcome.
Bias: Systemic error introduced in selection, allocation, treatment, or measurement.
Subject Selection Bias: How subjects were chosen.
Allocation Bias: How subjects were assigned to groups.
Treatment/Follow-up Bias: Potential for bias in how subjects were treated, maintained, or followed up.
Measurement Bias: Potential for bias in how measurements were made.
RAMMbo (Method for Eliminating Bias): A mnemonic for assessing study methods designed to reduce bias:
Recruitment:
Who did the subjects represent?
Were subjects representative of the target population?
Was the sample large enough?
Were subjects recruited randomly or consecutively?
Allocation:
Was allocation to treatments randomized or matched?
Were the groups similar at the start?
Maintenance:
Were the groups treated equally (apart from the intervention)?
Were outcomes ascertained and analyzed for most patients?
Measurement:
Were the measurements blind or objective?
The Strength of the Evidence
Definition: Depends on the of the treatment effect observed in clinical studies and the in that observed effect.
Confidence is often indicated by the of the confidence interval.
Also depends on the of findings across multiple studies.
Reasons for Importance: (NHMRC, )
Strong effects are less likely to result from study bias and are more likely to be real.
Strong effects are more likely to be clinically important.
**Outcome Measures:
Binary Measures: Typically yes/no outcomes (e.g., cancer, heart attack, stroke, death).
Reported as percentages ( ext{%}), rates, relative risk, absolute risk, hazard ratios, odds ratios, absolute risk reduction (), relative risk reduction ().
Continuous Measures: Vary along a continuum (e.g., height, weight, cholesterol).
Typically reported as means.
Are the Results Real and Relevant?
Generalizability: How do we know if an estimate from a study sample is true for the larger population?
Statistics - Hypothesis Testing:
p-values: A measure of the probability that a result is purely due to chance.
If the resulting probability is less than the pre-set alpha () level, the result is statistically significant.
Confidence Intervals (CI) - Estimation:
An estimate of the range of values likely to include the real population value.
Usually quoted as a 95 ext{%} confidence interval, meaning there is a 95 ext{%} chance that this range of values includes the real value.
More subjects generally lead to a narrower CI.
Important Distinction: Statistical significance does not necessarily imply clinical importance, and vice versa.
Evidence Versus Authority
Professional Importance: As professionals, distinguishing between evidence and authority is crucial; questioning and not accepting things at face value is vital.
Challenging Authority: Statements from figures of authority (e.g., a Harvard-educated doctor) do not automatically make them right or true. People can subconsciously bias their own data.
Critical Thinking: Apply critical thinking to lecture material; consider if information is accepted based on authority or verifiable evidence.
Authority-Based Conclusions: Arise from "opinion, experience, intuition, judgment, and scientific inference" (Guzelian & Guzelian, ).
Evidence-Based Conclusions: "Derived from an objective, unbiased, and systematic analysis of scientific knowledge" (Guzelian & Guzelian, ).
Risk
Definition: The possibility of something bad happening; the effect of uncertainty on objectives.
Absolute Risk
Definition: The probability that a specified event will happen in a specified population.
Example: Breast Cancer Risk:
in women will develop breast cancer in their lifetime, an absolute risk of 12.5 ext{%}.
Absolute risk increases with age:
From age to : in (0.43 ext{%}).
From age to : in (1.4 ext{%}).
From age to : in (2.6 ext{%}).
From age to : in (3.7 ext{%}).
Relative Risk (RR)
Definition: Compares the risk in one group relative to another; it is a ratio.
Interpretation:
: No difference in risk between the two groups.
RR < 1: The event is less likely to occur in the experimental group than in the control group.
RR > 1: The event is more likely to occur in the experimental group than in the control group.
Reporting Risk (Absolute vs. Relative)
Media Example: "Compared to women who do not drink, women who have two or more drinks per day have a 25 ext{%} higher risk of breast cancer."
Research Study Example: "Compared to women who do not drink, women who have two or more drinks per day have a relative risk of .
Context is Key: A 25 ext{%} increase (relative risk) sounds significant, but when considering the absolute risk:
If absolute lifetime risk is 12.5 ext{%}, an RR of means the new absolute risk is 12.5 ext{%} imes 1.25 = 15.63 ext{%}.
This is an increase from 12.5 ext{%} to 15.63 ext{%}, which is a 3.13 ext{%} absolute increase, not a 25 ext{%} increase in absolute terms.
Comparing Impact of Risk Reduction
Case 1: Absolute risk of disease A is per . Drug Y reduces it to per . Relative risk reduction () = 50 ext{%}.
Case 2: Absolute risk of disease B is per . Drug Q reduces it to per . Relative risk reduction () = 50 ext{%}.
Impact: Both have a 50 ext{%} RRR, but Case 2 has a much greater absolute impact (reducing disease in people vs. person).
Understanding Relative Risk Increase/Reduction
Case 3 (Relative Risk Increase):
Absolute risk of disease in non-smokers is in .
Relative risk increases by 50 ext{%} in smokers.
The 50 ext{%} relates to the absolute risk of . 50 ext{%} of is .
So, the absolute risk for smokers is in .
Case 4 (Relative Risk Reduction):
Men have a in risk of a disease by age .
New treatment reduces relative risk by 50 ext{%}.
The 50 ext{%} refers to the effect on the absolute risk of . 50 ext{%} of is .
The absolute risk is reduced from in to in .
Odds Ratio (OR)
Definition: The ratio of the odds of an event occurring in one group to the odds of it occurring in another group.
Use: Describes the strength of association, often used in retrospective studies.
Formula: Odds ratio () = (Likelihood of having risk factor if you have the disease) / (Likelihood of not having risk factor if you have the disease).
Distinction from Relative Risk: Often used interchangeably but is NOT the same as relative risk.
Approximation:
If the effect (disease occurrence) is small (e.g., in ):
Risk =
Odds =
In this case, OR () and risk () are very close.
If the effect is large (>5 ext{%}):
If disease occurs in :
Risk =
Odds =
In this case, OR () is not a good estimate of the risk ratio ().
Areas Identified by WHO for TCAM Development
Safety and Efficacy: Essential to ensure treatments are effective and do not pose risks to patients.
Education and Training of Practitioners: Crucial for maintaining high standards of care and ensuring practitioners are well-versed in safe and ethical practices.
Regulation of Practices: Necessary to establish quality control, protect the public from unqualified practitioners, and build confidence in TCAM modalities.
Intellectual Property: Important for safeguarding traditional knowledge, preventing misappropriation, and ensuring fair benefit-sharing for indigenous communities.
Research and Development: Vital for building scientific evidence, understanding the mechanisms of action, and fostering innovation in TCAM.
Integration into Health Systems: Aims to make TCAM services more accessible and to ensure they complement conventional medical approaches, enhancing overall health coverage.
Growing Economic Importance: Recognizes the significant economic contribution and market demand for TCAM products and services globally.