Reproductive Pathophysiology
1. Female Reproductive System Overview
Anatomy and Structure
The female reproductive system includes internal organs (ovaries, fallopian tubes, uterus, cervix, vagina) and external genitalia (vulva). The system is divided into:
Upper tract: Ovaries, fallopian tubes, uterus
Lower tract: Cervix, vagina, vulva
![Female Reproductive Anatomy]

Diagram of the internal female reproductive organs including fallopian tubes, ovaries, uterus, cervix, vagina, and hymen
Menstrual Cycle and Hormonal Control
The menstrual cycle is controlled by hormonal feedback between the hypothalamus, pituitary, and ovaries.
Ovarian Cycle Phase | What Happens in Ovary | Uterine Cycle Phase | What Happens in Uterus | Dominant Hormones | If No Pregnancy |
|---|---|---|---|---|---|
Follicular (Days 1-14) | FSH stimulates follicle development | Menstruation (Days 1-5) + Proliferative (Days 6-14) | Shedding then rebuilding of endometrium | FSH, Estrogen | FSH/estrogen prepare for ovulation |
Ovulation (Day 14) | LH surge releases mature egg | N/A | N/A | LH surge | Egg released |
Luteal (Days 15-28) | Corpus luteum produces progesterone | Secretory Phase (Days 15-28) | Endometrium becomes thick, vascular | Progesterone, Estrogen | Corpus luteum degenerates → hormone drop → menstruation |
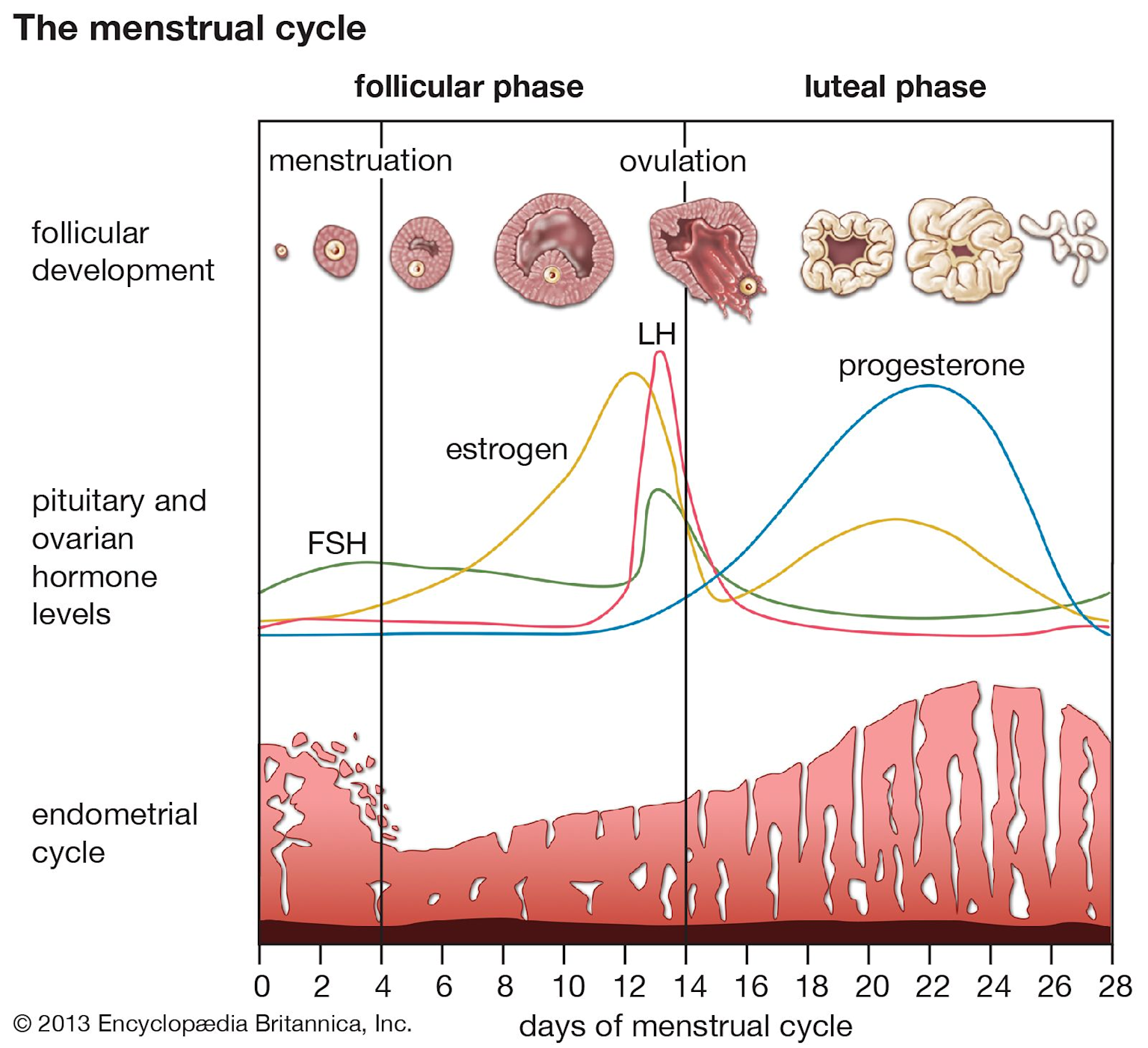
Diagram of the menstrual cycle phases showing hormone levels, follicular development, ovulation, and endometrial changes over 28 days
2. Sexually Transmitted Infections (STIs)
Bacterial STIs
STI | Organism | Symptoms (Females) | Symptoms (Males) | Neonatal Effects | Treatment |
|---|---|---|---|---|---|
Chlamydia | Chlamydia trachomatis | Often asymptomatic; discharge, bleeding, pain | Often asymptomatic; dysuria, discharge | Conjunctivitis, pneumonia (2/3 exposed) | Azithromycin or doxycycline |
Gonorrhea | Neisseria gonorrhoeae | Dysuria, discharge, pain; often asymptomatic | Dysuria, purulent discharge | Conjunctivitis (prevented by erythromycin ointment) | Ceftriaxone + azithromycin |
Syphilis | Treponema pallidum | Stage 1: Painless chancre; Stage 2: Rash; Stage 3: Organ damage | Same as females | Congenital syphilis | Penicillin G |
Viral STIs
Viral STI | Type | Transmission | Symptoms/Complications | Prevention | Treatment |
|---|---|---|---|---|---|
HSV | HSV-1 (oral), HSV-2 (genital) | Skin contact, vertical | Vesicular lesions, lifelong latent infection | Condoms, avoid outbreaks | Antivirals; no cure |
HPV | DNA virus (70+ types) | Sexual, skin-to-skin | Warts, cancers (cervical 95%, anal, oropharyngeal) | HPV vaccine(nearly 100% effective) | No cure; treat warts |
Hepatitis B/C | Bloodborne viruses | Blood, sexual fluids | Liver damage, cirrhosis, cancer | Hep B vaccine, safe sex | Antivirals |
HIV/AIDS | Retrovirus | Sexual, blood, vertical | Immune destruction, opportunistic infections | PrEP, condoms | ART; no cure |
Zika | Flavivirus | Mosquito, sexual, vertical | Fetal microcephaly, neurological complications | Condoms 6 mo. post-infection | Supportive only |
3. Pelvic Inflammatory Disease (PID)
Definition: Infection of upper female reproductive tract (uterus, fallopian tubes, ovaries)
Common Causes: Chlamydia trachomatis (most common), Neisseria gonorrhoeae, polymicrobial
Pathophysiology: Ascending infection from lower tract → inflammation → scarring of fallopian tubes
PID Diagnostic Criteria
Pelvic/lower abdominal pain PLUS:
Fever >101°F
Purulent vaginal/cervical discharge
Elevated WBC, ESR, or CRP
Cervical motion tenderness
Complications
Infertility (tubal scarring)
Ectopic pregnancy (scarred tubes)
Chronic pelvic pain
Tubo-ovarian abscess
Treatment
Antibiotics: Ceftriaxone + doxycycline ± metronidazole
Treat sexual partners
PID Pathophysiology Flowchart

Pelvic Inflammatory Disease (PID) Pathophysiology and Complications
4. Female Sexual Dysfunction and Infertility
Condition | Definition/Cause | Symptoms | Treatment |
|---|---|---|---|
Sexual Dysfunction | Persistent difficulty with desire, arousal, orgasm, or pain | Low libido, arousal difficulty, painful intercourse | Hormone therapy, counseling, treat underlying causes |
Infertility | Failure to conceive after 1 year (35% female factors) | Inability to conceive, irregular periods | Treat underlying cause, IVF, surgery |
5. Endometriosis vs Adenomyosis
Feature | Endometriosis | Adenomyosis |
|---|---|---|
Tissue Location | OUTSIDE uterus (ovaries, pelvis, bladder) | INSIDE uterine muscle wall (myometrium) |
Tissue Type | Endometrial-like tissue | Actual endometrial tissue |
Beyond Uterus | Yes | No (confined to uterus) |
Uterine Enlargement | No (usually) | Yes (thickened, enlarged) |
Symptoms | Painful periods, sex, bowel movements; infertility | Heavy/painful periods, enlarged uterus, chronic pain |
Diagnosis | Laparoscopy with biopsy | MRI, ultrasound, physical exam |
Treatment | Hormonal therapy, NSAIDs, surgical excision | Hormonal birth control, NSAIDs, hysterectomy |
6. Polycystic Ovary Syndrome (PCOS)
Definition: Hormonal disorder characterized by hyperandrogenism and ovulatory dysfunction
Pathophysiology:
↑ GnRH pulse frequency
↑ LH:FSH ratio
↑ LH → Theca cells produce excess androgens
↓ FSH → Follicular arrest → polycystic ovaries (multiple small follicles)
Insulin resistance → ↑ insulin → ↑ androgens (vicious cycle)
Symptoms:
Irregular/absent periods (oligomenorrhea, amenorrhea)
Hirsutism (male-pattern hair growth - 60%)
Acne (severe, persistent)
Obesity (but can occur in lean women)
Infertility (leading cause)
Acanthosis nigricans (dark, thick skin patches from insulin resistance)
Treatment:
Lifestyle modifications (weight loss, exercise)
Metformin (insulin sensitizer)
Oral contraceptives (regulate cycles, reduce androgens)
Ovulation induction (for fertility)
PCOS Pathophysiology Diagram

PCOS Pathophysiology and Clinical Manifestations
7. Female Reproductive Cancers
Cancer Type | Risk Factors | Symptoms | Screening | Why Often Detected Late | Treatment |
|---|---|---|---|---|---|
Cervical | HPV (95%+) , smoking | Abnormal bleeding, discharge | Pap smear, HPV test, vaccine | Often asymptomatic early | Surgery, radiation, chemo |
Endometrial | Obesity, unopposed estrogen, PCOS | Postmenopausal bleeding | No routine screening | Symptoms appear later | Hysterectomy, radiation |
Ovarian | BRCA, family history, age | Bloating, pelvic pain, early satiety | No routine screening | Deep location, vague symptoms | Surgery, platinum-based chemo |
Breast (Triple-Negative) | BRCA mutations | Lump, nipple changes | Mammography, MRI | Usually detected via screening | Chemotherapy(mainstay) , surgery,immunotherapy (pembrolizumab) |
Triple-Negative Breast Cancer (TNBC):
Lacks estrogen receptors, progesterone receptors, and HER2 protein
Cannot use hormone therapy or HER2-targeted therapy
Chemotherapy is main treatment (anthracyclines, taxanes, alkylating agents)
Immunotherapy (pembrolizumab) approved for TNBC
Often treated with neoadjuvant chemotherapy (before surgery)
Tends to respond well to chemo but higher recurrence rate
8. Male Reproductive System Overview
Anatomy and Function
The male reproductive system includes testes, epididymis, vas deferens, seminal vesicles, prostate, and penis.
![Male Reproductive Anatomy]
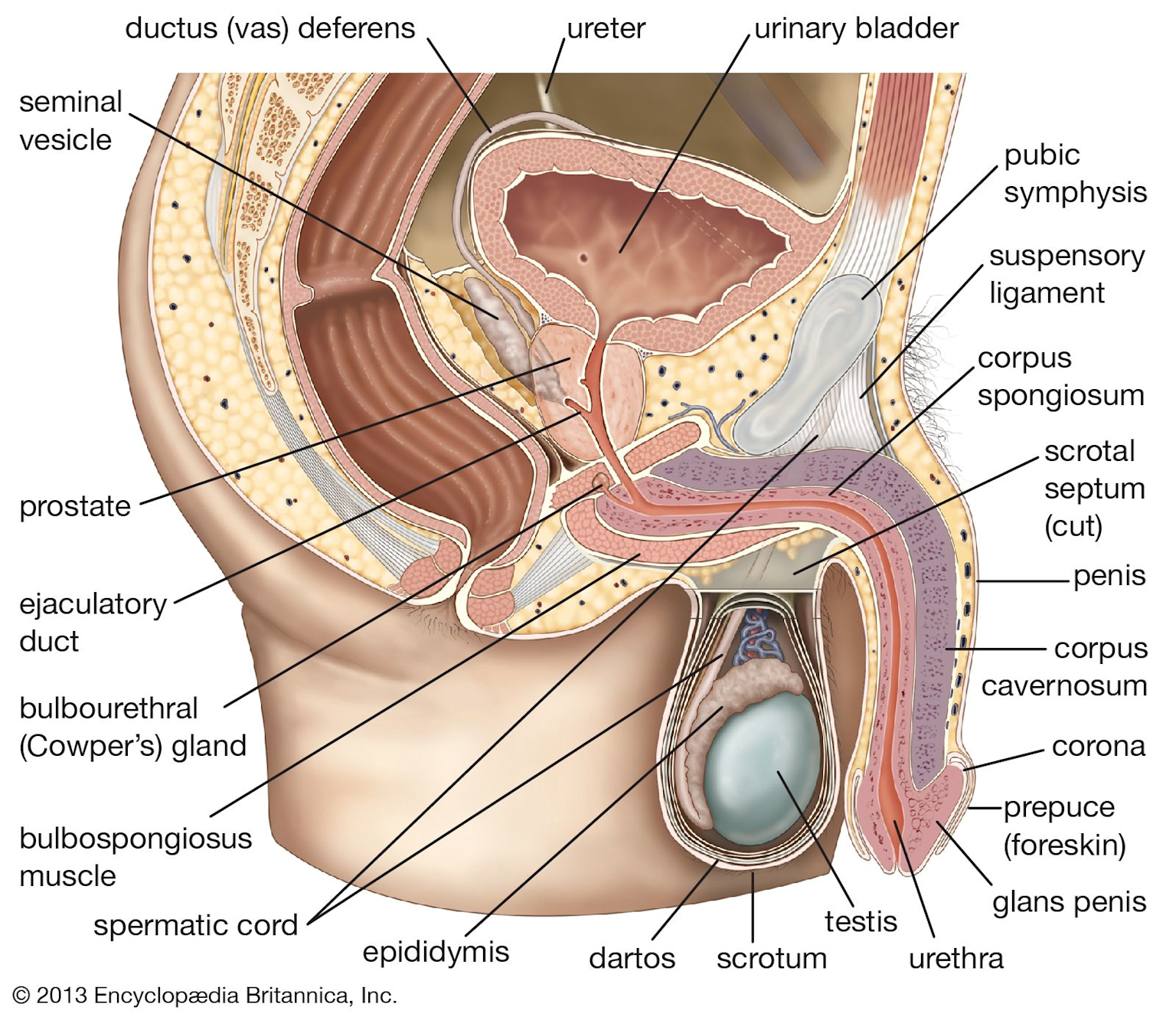
Anatomical labeled diagram of the male reproductive system showing internal and external structures relevant to reproductive pathophysiology
Testosterone and Spermatogenesis
Leydig cells: Produce testosterone (stimulated by LH)
Sertoli cells: Support sperm development, provide nutrients
Testosterone: Stimulates spermatogenesis, secondary sex characteristics
9. Male Sexual Dysfunction and Infertility
Condition | Definition | Causes | Symptoms | Treatment |
|---|---|---|---|---|
Erectile Dysfunction | Inability to achieve/maintain erection | Vascular disease, diabetes, medications, psychological | Difficulty with erection, reduced desire | PDE5 inhibitors (sildenafil), lifestyle changes |
Male Infertility | Failure to conceive (30% male factors) | Low sperm count, abnormal sperm, varicocele, hormonal issues | Inability to conceive, abnormal semen analysis | Treat cause, hormonal therapy, IVF |
Varicocele | Enlarged scrotal veins | Valvular incompetence | Scrotal pain, "bag of worms", testicular atrophy | Surgical repair if symptomatic |
Cryptorchidism | Undescended testicle | Developmental failure | Empty scrotum, ↑ cancer risk, infertility | Surgical correction (orchiopexy) |
Male Infertility Causes Diagram

Causes of Male Infertility - Four Main Categories
10. Benign Prostatic Hyperplasia (BPH) vs Prostate Cancer
Feature | BPH | Prostate Cancer |
|---|---|---|
Definition | Non-cancerous prostate enlargement | Malignant tumor of prostate |
Nature | Benign | Malignant |
Age | Usually >50 years | Usually >65 years |
PSA Level | May be elevated but usually <10 ng/mL | Often >10 ng/mL |
DRE | Smooth, symmetrically enlarged | Hard, irregular nodules |
Symptoms | Frequency, urgency, weak stream, nocturia, incomplete emptying | Often asymptomatic early; later same as BPH + bone pain |
Complications | Acute retention, UTIs, bladder stones, hydronephrosis | Metastasis (bones, lymph nodes), pain |
Treatment | Alpha-blockers, 5-alpha reductase inhibitors, TURP | Surgery, radiation,hormone therapy (ADT) |
BPH Comorbidities: Metabolic syndrome, diabetes, obesity, cardiovascular disease
11. Male Reproductive Cancers
Prostate Cancer
Screening: PSA blood test + digital rectal exam (DRE)
Treatment Options:
Localized: Active surveillance, radical prostatectomy, radiation
Advanced/Metastatic: Hormone therapy (Androgen Deprivation Therapy - ADT)
Hormone Therapy for Prostate Cancer:
Goal: Lower testosterone levels or block testosterone action
Types:
LHRH agonists/antagonists: Block testosterone production
Anti-androgens: Block testosterone from reaching cancer cells
Androgen synthesis inhibitors (abiraterone): Drop testosterone lower than other treatments
Orchiectomy: Surgical removal of testicles (less common)
Use: Shrink prostate before radiation, treat metastatic disease, relieve pain
Castration-resistant prostate cancer: Cancer becomes resistant to hormone therapy after months/years; requires additional treatments
Testicular Cancer
Most Common in Ages 15-35
Cell Types:
Seminoma (40%): Pure seminomatous germ cell tumor
Non-seminoma (60%): Embryonal, teratoma, choriocarcinoma, yolk sac tumor
Diagnosis:
Physical exam, scrotal ultrasound
Tumor markers: AFP, β-hCG, LDH
Radical inguinal orchiectomy: Removes affected testicle (diagnostic + therapeutic)
Treatment:
Stage I Seminoma:
Surveillance (preferred)
OR Single-agent carboplatin
OR Radiotherapy
Stage II-III Seminoma:
Chemotherapy: BEP (bleomycin, etoposide, cisplatin) or EP (etoposide, cisplatin)
Radiotherapy (select cases)
Non-seminoma: Chemotherapy (BEP) ± surgery
Prognosis: Excellent; 5-year survival ~97% overall; >95% for stage I seminoma
Cancer Treatment Pathways Comparison

Treatment Pathways: Prostate Cancer vs Testicular Cancer
12. Case Study Applications
Jennifer's PID Evaluation and Treatment
Evaluation for PID:
Pelvic exam (cervical motion tenderness)
Laboratory: WBC count, ESR, CRP
NAAT testing for chlamydia/gonorrhea
Pregnancy test (rule out ectopic)
Pelvic ultrasound (if abscess suspected)
Treatment if PID confirmed:
Antibiotics: Ceftriaxone IM + doxycycline PO ± metronidazole
Treat sexual partners
Hospitalization if severe, pregnant, or tubo-ovarian abscess suspected
Lily's PCOS Effects
Menstrual Cycles:
Irregular or absent periods (oligomenorrhea/amenorrhea)
Anovulation (no ovulation) or infrequent ovulation
Androgen Levels:
Elevated testosterone (1.5x higher than normal)
Causes hirsutism, acne, male-pattern baldness
Fertility:
Leading cause of female infertility
Lack of ovulation prevents conception
Can be treated with ovulation-inducing medications
Daniel's BPH vs Prostate Cancer
If BPH Instead of Prostate Cancer:
Symptom Differences:
BPH: Urinary symptoms (frequency, urgency, weak stream, nocturia, incomplete emptying)
Prostate cancer (early): Often asymptomatic; detected via elevated PSA or abnormal DRE
No bone pain, weight loss, or metastatic symptoms with BPH
Treatment Options for BPH:
Watchful waiting (mild symptoms)
Medications:
Alpha-blockers (e.g., tamsulosin, doxazosin): Help relax the muscles in the prostate and bladder neck.
5-alpha-reductase inhibitors (e.g., finasteride, dutasteride): Reduce prostate size and lower levels of dihydrotestosterone (DHT).
Combination therapy
Minimally invasive procedures: Prostate artery embolization (PAE), prostatic urethral lift
Surgery: TURP (transurethral resection of prostate), laser procedures
13. Key Takeaways for ADHD Learners
✓ STIs: Know the Big 3 bacterial (chlamydia, gonorrhea, syphilis) and viral (HSV, HPV, HIV)
✓ PID: Ascending infection → scarring → infertility/ectopic pregnancy
✓ Endometriosis vs Adenomyosis: OUTSIDE uterus vs INSIDE uterine muscle
✓ PCOS: High LH:FSH ratio → excess androgens → no ovulation → infertility + hirsutism
✓ Female cancers: HPV causes cervical cancer (95%+); screening saves lives
✓ Male infertility: 4 categories - sperm production, delivery, lifestyle, medical conditions
✓ BPH vs Prostate Cancer: BPH = benign, urinary symptoms; Cancer = malignant, often asymptomatic early
✓ Prostate cancer treatment: Hormone therapy (ADT) blocks testosterone to slow growth
✓ Testicular cancer: Orchiectomy first, then chemo (BEP/EP for seminoma); excellent prognosis