Saliva
There are 3 pairs of salivary glands
Parotid (largest) - serous saliva
Sublingual - mucous saliva
Submandibular - mixed saliva
Each produces saliva but of a different consistency
There is also minor glands in the palates and lips - mucous
Serous = watery. This is because it doesn’t have much mucous in it.
All the salivary glands secrete both protein and fluid. The consistency of saliva is determined by the nature of the secreted protein.
Acinar = grape-like
Mucous acinus will secrete mucous. Serous acinus does not.
With a stain, the serous acinus will stain darker and mucous acinus will stain lighter.
The acinus produces the fluid which flows through the ducts and makes it way down to the mouth.
→ Intercalated ducts: come straight off the acini. Duct cells are similar to acinar cells but don’t secrete protein (they may secrete fluid)
→ Striated ducts: ‘stripey’ ducts
→ Excretory ducts: carry the saliva down into the mouth
Acinus Cell
Polarised cells so have a basolateral (blood) side and an apical (lumenal) side
At the basolateral pole, there is a nucleus, lots of membrane-bound structures (ER, golgi, etc)
Is a protein-producing cell, as proteins are made inside the ER
The Production of Saliva
It is regulated via the process stimulus secretion coupling
→ saliva must contain protein and fluid
Protein secretion is regulated by the second messenger cycle adenosine monophosphate (CAMP)
Fluid secretion is regulated by changes in intracellular calcium
CAMP are regulated by noradrenaline binding to beta-adrenergic receptors (noradrenaline comes from the sympathetic nervous system)
Intracellular calcium is regulated by acetylcholine binding to muscarinic receptors (acetylcholine comes from the parasympathetic nervous system)
→ These two are working collaboratively
CAMP Regulation
The beta-adrenergic receptor (G protein coupled receptor) is coupled to a heterotrimeric protein which has 3 subunits of alpha, beta and gamma. There is also a target enzyme which is the target for the activated G protein.
Noradrenaline binds to the receptor and activates it. This activates the G protein and the alpha subunit detaches from the beta gamma units
The alpha subunit will float away in the cytoplasm and come into contact with the enzyme adenylate cyclase, which then turns ATP into CAMP
→ CAMP goes into the nucleus where there’s CAMP-dependent transcription factors for protein production
→ CAMP goes into the ER/golgi where it stimulates glycosylation (adding a carbohydrate group to the protein)
→ CAMP also stimulates the formation and maturation of secretory vesicles
→ In salivary acinar cells, CAMP stimulates exocytosis
CAMP regulates all processes of protein secretion from scratch
CAMP-mediated processes
→ a process regulated by CAMP will have lots of things happening at the same time
Not all proteins found in saliva have been made by the salivary gland cells. IgA in saliva is from the bloodstream.
On the basolateral border of salivary gland acinar cells are receptors (for IgA)
IgA will bind to receptors and will then be stimulated to be internalised by endocytosis
It will cross the cell by transcytosis and release the iGA on the other side by exocytosis
→ If it has been secreted, a tiny bit of receptor is stuck onto it (secretory fragment)
The name of the receptor is polymeric immunoglobulin receptor
Fluid Secretion
M3 muscarinic receptor is similar to the beta-adrenergic receptor, as they are both G protein-coupled super family of receptors
- The agonist for this receptor is acetylcholine
Acetylcholine binds to and activates M3 muscarinic receptor
The G protein becomes activated and the alpha subunit dissociates and binds to its target enzyme (phospholipase C)
- Phospholipase C takes phosphatidylinositol-4,5-biphosphate into diacylglycerol and inositol-1,4,5-triphosphate (IP3)
- IP3 binds to IP3 receptors on the ER, opening the calcium channels and causes calcium release into the cytoplasm, increasing the intracellular calcium
The calcium-dependent chloride channel on the apical membrane of the acinar cells opens and activates. This allows chloride to leave the cell
(Both IP3 and increased calcium are secondary messengers)
→ Acetylcholine is a first messenger
A basolateral potassium channel is activated by calcium and releases K+ on the other side of the cell. Now there’s charge separation.
Negative charge → out of the apical side
Positive charge → out the basolateral
- The negative charge attracts cations across the tissue and Na+ can pass freely between the cells by the electrochemical potential that has been created
→ This is unidirectional salt transport (NaCl) which increases the strength of solution on the apical side which cconstitues an osmotic gradient which moves water
Whenever you see secretion, you are extrenely likely to see the actiavtion of a chloride channel (on the apical side)
Outside the cell = first messengers
Inside the cell = second messenger
→ the production of secondary messengers is what actually gets the information across the membrane/barrier)
INconstistency
Fluid secretion is led by ion transport
The secretion must be isotonic
Resting saliva is hypertonic
Striated ducts remove salts from the saliva as it passes through so that it gets weaker and weaker. This is called the two-stage hypothesis.
1st stage = production of an isotonic saliva
2nd stage = modified
The acinus cells are much better at producing fluid secretion than the ducts are at absorbing - therefore, the composition of saliva depends on the salivary flow rate
Low = hypotonic (as ducts have time to absorb salt)
High = lots of bicarbonate
Bicarbonate is the main acid buffer, so you want it in your saliva
Overall Regulation of Salivation
Mastication, taste, smell, anticipation → +superior (pons), salivary nuclei → (VII) submandibular, sublingual salivary glands
Fear → - inferior (medulla salivary nuclei → (IX) parotid salivary gland
Functions of Saliva
Digestive - salivary amylase, lingual lipase
Tooth maintenance
Lubrication - allows speech, mastication and deglutition
Antibacterial/antifungal - protective barrier, IgA, lysozyme
Tooth Maintenance
Dilution (of the contents of the mouth)
Clearance (swallowing)
Buffering (bicarbonate will buffer acid made by plaque bacteria)
Stephan curve:
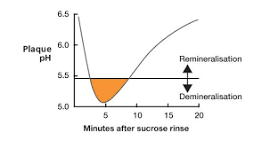
When the pH <5.5, your teeth demineralise and start to dissolve in the acid. Rampant caries occur (no saliva)
Lubrication
Salivary glycoproteins are sticky
They stick together and create a film which can slide over each other easily and protect/lubricate the whole of the inside of the mouth
→ Salivary glycoportoeins allow saliva to form a thin layer on the oral surfaces and on food, which is important for mastication (chewing) and deglutition (swallowing).
Deglutition
Oral/buccal: voluntary. The bolus is pushed to the back of the mouth by the tongue. The teeth are brought together. The soft palate elevates to close the nasal cavity. The larynx rises to close the airways.
Pharyngeal: involuntary (reflex). The cricopharyngeal sphincter relaxes to open the oesophagus. The epiglottis steers the bolus over the trachea and the peristalsis starts.
Oesophageal: peristalsis. All of the above reversed.
Antibacterial/Antifungal
Mucus layer creates a film and covers all the surfaces so that bacteria can’t access it
Lysozyme is good at getting rid of opportunistic effectors
Salivary Gland Pathology
No saliva = dry mouth
→ Dry mouth is called xerostomia
- Generally, if you lose ½ of your saliva, you will complain of a dry mouth which may take salivary flow rates down
Consequences:
Rampant caries
Opportunistic infections
Plateau stephan curve
Causes:
Analgesics (xerogenic drugs)
Antihypertensives (xerogenic drugs)
Antidepressents (xerogenic drugs)
- Ibuprofen is an analgesic
Radiotherapy
Diseases such as Sjorgen’s syndrome (an autoimmune condition that causes salivary gland dysfunction and atrophy)