3.7: Homeostasis + kidney
Homeostasis
The maintenance of an organism’s internal environment, including within cells and within the body itself.
It keeps the body in a dynamic equilibrium, meaning it is constantly adjusting to changes but body systems are kept at an optimum, or set point.
This can include tissue fluids supplying nutrients and removing waste, and maintenance of pH, core temperature and solute potential.
This allows cells to function normally, despite external changes.
Negative feedback
This is the process of maintaining homeostasis, by the body reacting to a change from the set point and changing. There are five steps:
The set point, for example temperature, is changed by the cold.
The receptor detects this, including the level of the deviation. It then sends these instructions to a co-ordinator.
The co-ordinator communicates with one or more effectors to make corrective changes.
The effector can be a muscle or a gland, and brings about the change in order to return to the set point. In the case of cold temperature, this could be shivering.
The set point is achieved, and the effectors stop effectors from performing corrective changes.
Examples of negative feedback loops include:
Glucose concentration in plasma. If it is too high, insulin is secreted to convert it to glycogen and increasing its rate of respiration. If it is too low, glucagon is secreted to convert glycogen to glucose.
Core temperature. If it is too high, superficial blood vessels dilate (widen) to cause heat to radiate from the body. If it is too low, superficial blood vessels constrict and respiration increases to produce heat.
Positive feedback
The opposite of negative feedback, where an alteration from a set point is increased to further move away from the set point.
It is quite rare.
Examples of positive feedback loops include:
Oxytocin, which stimulates contractions during childbirth. More contractions produce more oxytocin, which continues to increase.
When a cut occurs, platelets adhere to the cut surface. They then secrete signals to attract more platelets to the site for clot formation.
Kidney
It has two main functions:
Excretion - the removal of nitrogenous metabolic waste from the body.
Osmoregulation - Control of the water potential of body fluids (such as plasma, tissue fluid and lymph) by regulating water content, and therefore, solute concentration.

Structure
Humans have two kidneys, located in the posterior abdomen either side of the spine.
They are around 10cm long, 5cm wide and 3cm thick.
They receive blood from the renal artery and return it to general circulation via the renal vein.
The structure from outer to inner:
A tough renal capsule protects the kidney.
The cortex is where the part of the nephron containing Bowman’s capsules is located, which filters blood.
The medulla, or renal pyramids, contain collecting ducts that carry urine to the pelvis.
The pelvis empties urine to the ureter.
The ureter carries urine to the bladder.
Urea production
Occurs in steps:
Dietary proteins are converted to amino acids.
These are transported around the liver, and then the rest of the body, in order to synthesise necessary proteins.
Excess amino acids are deaminated in the liver.
The amino acids are converted to urea, and the remaining organic acids are respired in the Krebs cycle.
Other nitrogen containing waste products can be converted to urea - a low concentration of creatinine is released in sweat and urine.
The urea is then carried in the plasma to the kidneys, where it is excreted in urine.
Nephron
Nephrons, or kidney tubules, are blood filtering units.
There are about a million in each kidney, and they are around 30mm.
Blood goes through the kidney as:
Enters through the renal artery.
An afferent arteriole - a branch of the renal artery - brings blood to the nephron.
It divides into around 50 parallel capillaries in the glomerulus, which is enclosed by the Bowman’s/renal capsule.
The filtered blood is carried out an efferent arteriole.
It then passes through a capillary network surrounding the proximal (PCT) and distal convoluted tubule (DCT).
PCT is where selective reabsorption happens.
Then it passes to a capillary network surrounding the loop of Henle, known as the vasa recta.
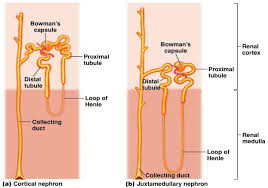
The loop of Henle has two limbs, the ascending and descending. The descending limb connects to the PCT and the ascending limb connects to the DCT.
The loop of Henle is in the medulla.
It is responsible for reabsorption of water.
Blood filtrate is diverted through the nephron, and the collecting ducts of many nephrons join to carry urine to the pelvis.
The collecting ducts are responsible for more water reabsorption, and involves hormones.

Ultrafiltration
This occurs under high pressure, as the blood comes directly from the heart. There are three levels between the glomerulus capillaries and the Bowman’s capsule, known as the Bowman’s space.
Filtrate moves through in four steps:
Blood moves into the glomerulus via the afferent arteriole, which is wider than the efferent.
Molecules must move through the capillary walls, via pores in the endothelium cells known as fenestrae. These are around 80nm in diameter.
Then it must pass through the basement membrane, which is made of protein including mainly collagen and glycoproteins. It is a molecular filter and selective barrier, acting as a sieve.
Finally is the wall of the Bowman’s capsule, made of squamous epithelial cells known as podocytes. These podocytes have projections known as pedicels, which wrap around a capillary to bring it closer to the basement membrane.
Gaps between these pedicels are known as filtration slits, filtrate moves through this.
This forces glomerular filtrate, containing water, glucose, salts, urea and amino acids.
This is because they are 30,000-68,000 RMM.
It is designed like this to prevent necessary molecules to stay in the blood including; blood cells, platelets and large proteins.
Therefore this filtrate resembles plasma, and the blood that passes through the efferent arteriole has low water potential due to the water loss.

Selective reabsorption
While the glomerular filtrate contains some molecules the body needs to excrete, it also takes some necessary molecules such as glucose, amino acids, water, sodium ions and chloride ions.
This process involves the useful nutrients being reabsorbed as the filtrate flows through the nephron.
PCT structure
The PCT has cuboidal epithelial cells in the walls that are specialised for the selective reabsorption process:
A large SA due to its length, convolution (twistiness) and the amount of nephrons in the body.
Microvilli projections on the cuboidal epithelial cell walls. They are 1um long and face the lumen where glomerular filtrate moves through.
There are invaginations (areas turned inside out or folded back on themselves) known as basal channels on the side facing the capillaries.
Tight junctions between neighbouring PCT cells. These are multi-protein complexes that encircle a cell and attach it tightly to neighbouring cells.
This is to prevent molecules from diffusing between adjacent cells or from the cell back to the filtrate.
Close contact with capillaries, to shorten diffusion distances and maintain a constant concentration gradient.
Many mitochondria for ATP production needed for active transport.
Many RER and golgi bodies for protein production needed for facilitated, active and co-transport.
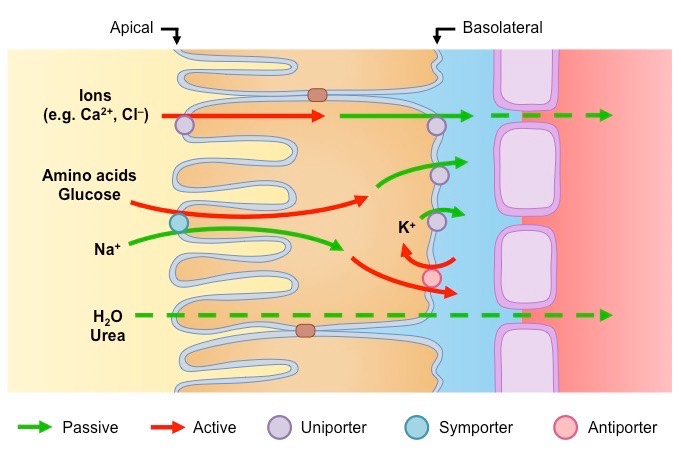
Glucose/amino acid transport
This happens via co-transport (AKA secondary active transport) and active transport:
PCT cuboidal epithelial cells actively transport sodium ions into the tissue fluid. This lowers sodium ion concentration in the cytoplasm of these cells.
Sodium ions from the glomerular filtrate can now enter these cells via facilitated diffusion. Two molecules bind to a transporter protein in the cell membrane, along with one amino acid or glucose molecule.
They then enter the cell via co-transport/facilitated diffusion. This is also known as secondary active transport.
The amino acid or glucose molecules dissociate from the transporter - sodium ions.
They then diffuse down the cell via the concentration gradient.
Glucose then moves into the capillary via facilitated diffusion.
Ion transport
Reabsorption of this can be passive diffusion, but mostly active transport.
Water transport
Water moves into the capillaries via osmosis, as the reabsorbed ions in the blood reduce its water potential.
About 90% of water is reabsorbed.
Urea/small proteins transport
Urea and small proteins diffuse into the blood.
Due to the water loss from the filtrate, this is a steep concentration gradient.
About 50% of urea and small proteins are reabsorbed.
Glucose threshold
The body is disadvantaged if any glucose is lost, as it is an important energy source.
However, if concentration is too high, there will not be enough transport molecules in the PCT to move all the glucose.
It will then pass into the loop of Henle. This can be caused by:
Too little insulin secretion by the pancreas (Type 1 diabetes).
Liver cells have a reduced response to insulin due to damage to insulin receptors in membranes (Type 2 or gestational diabetes).
Water reabsorption
To avoid dehydration, more water reabsorption is needed.
90% is reabsorbed in the PCT, and a further 5% is absorbed from the collecting duct.
Although, some water is still absorbed through the loop of Henle and DCT.
The PCT and loop of Henle have stereotyped functions, meaning these always act the same way.
The collecting duct and DCT respond to the body’s needs, allowing them to have a more fine control of the water’s body content.
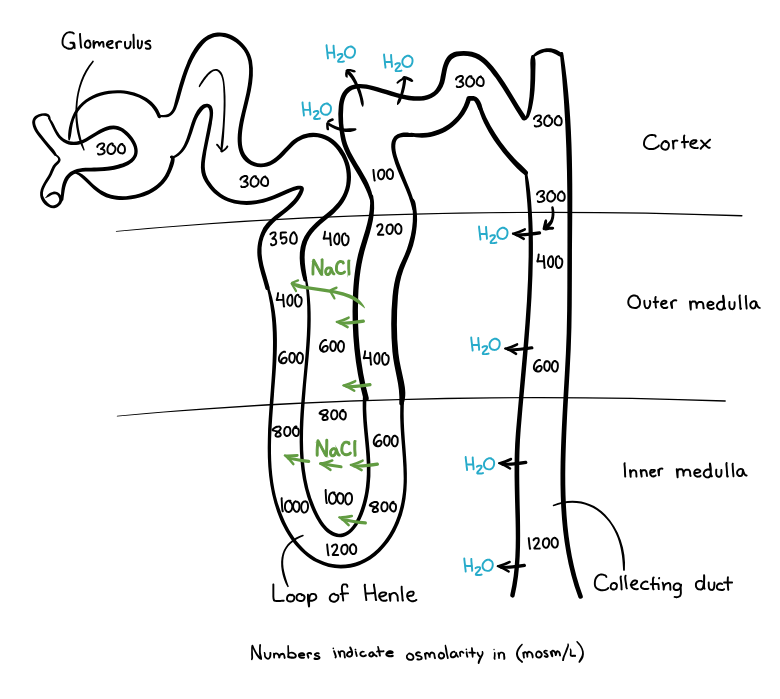
Counter current flow mechanism
This occurs in the loop of Henle, with 3 main steps:
The ascending limb, which is impermeable to water, actively transports sodium and chloride ions out of the filtrate in the tubule into the medulla tissue fluid.
This lowers the water potential in the medulla, and increases the water potential in the filtrate as it has less ions and is more dilute.
The descending limb, which is permeable to water and slightly permeable to sodium and chloride ions, has water leave via osmosis into the medulla tissue fluid.
This is due to the low water potential in the medulla, created by the ascending limb.
Some sodium and chloride ions also diffuse into the descending limb. This allows more ions to be moved out.
Due to this counter current flow, the hairpin bend at the bottom of the loop of Henle has the lowest water potential.
Overall, the loop of Henle is constructed as: descending limb - hairpin bend - ascending limb. In terms of different metrics:
Low solute concentration - highest solute concentration - low solute concentration.
High water potential - lowest water potential - high water potential.
This mechanism is called the countercurrent multiplier as:
The limbs flow in opposite directions.
This multiplies the solute concentration in the hairpin bend.
The collecting duct then utilises this high solute concentration in the medulla, in 3 steps:
The duct runs through the low water potential medulla region.
Water leaves via osmosis.
The longer the collecting duct, the lower the water potential in the medulla and the more water leaves via osmosis.
The filtrate then becomes more concentrated than the blood - hypertonic - and by the base of the collecting duct is urine.
Osmoregulation
Osmoregulation maintains the concentration of enzymes and metabolites (water) to ensure cell reactions occur at a constant and appropriate rate.
Humans gain most of our water from drinking, but around 10% is metabolic water.
It uses negative feedback, for example in the case of too low water potential:
Blood has a lower water potential, which could be caused by:
Increased sweating.
Reduced water intake.
Large salt intake
The receptor is the osmoreceptors in the hypothalamus.
They are also the coordinators, signalling the effector.
Secretory granules carry ADH along axons to the effector.
The effector is the posterior lobe of the pituitary gland, which when signalled releases stored ADH into the bloodstream.
ADH stands for antidiuretic hormone, and is secreted if there is not enough water in the blood, and is secreted less if there is too much water in the blood.
This increases the permeability of the DCT and the collecting duct to water.
More water is reabsorbed into the region of high solute concentration and low water potential.
More water is therefore absorbed by the vasa recta.
Urine produced is relatively concentrated, has a low volume and darker colour.
In the case of higher water potential:
A higher water potential is detected, likely due to water consumption.
The receptor is the osmoreceptors in the hypothalamus.
They are also the coordinators, signalling the effector.
The posterior lobe of the pituitary gland releases less ADH into the blood.
This decreases the permeability of the DCT and collecting duct.
Less water is reabsorbed into the blood.
Urine produced is less concentrated, has a high volume and lighter colour.
ADH mechanism
Aquaporins are intrinsic membrane proteins with a pore which water molecules move through.
There are 13 types, 6 of which are in the kidney. More types are suspected to exist.
They are used to increase the permeability of the DCT and collecting duct. This happens in 4 steps:
The ADH molecule binds to membrane receptors.
Adenyl cyclase then catalyses the production of cyclic AMP, the second messenger.
Vesicles containing aquaporins then fuse with the cell membrane.
Water molecules then move through the pores into the cell, down a water potential gradient.
When ADH levels fall, cyclic AMP levels fall, and aquaporins are removed from the cell membrane to accumulate again in vesicles.
Inhibitors
Diuresis is the production of a large volume of diluted urine.
Diuretics cause the production of a large volume of urine, as they inhibit the production of ADH.
This prevents the DCT and collecting ducts from becoming permeable, and therefore keeps water in the filtrate.
This causes more water to enter urine and increase its concentration, and less to enter the blood.
This can cause dehydration and crenation of cells.
Less ADH = less permeable membranes = less water in blood = more water in urine.
Examples are alcohol and coffee, which can cause dehydration.
Anti-diuretics cause the production of low amounts of urine, by increasing the production of ADH.
This prevents the DCT and collecting ducts from becoming impermeable, and therefore water leaves the filtrate.
This causes more water to leave urine and decrease it’s concentration, and more to enter the blood.
This can cause haemolysis.
More ADH = more permeable membranes = more water in blood = less water in urine.
An example is MDMA.
Kidney failure
The kidney’s major roles are osmoregulation and excretion. If it fails, this can cause:
Inability to remove urea from the body, which reaches toxic levels.
Inability to release excess water content, meaning body fluids are diluted and compromising metabolic reactions.
Causes
Diabetes - High glucose concentration in plasma causes glomeruli to lose some protein, especially albumin, into the filtrate. Some even link together.
This causes a condition known as glomerulosclerosis.
High blood pressure - Damages glomerular capillaries and prevents ultrafiltration.
Autoimmune disease - The body makes antibodies against its own tissues.
Infections.
Crushing injuries.
Treatments
Only one kidney is needed to remain healthy, although there might be some loss of kidney function in the future.
If both are damaged, treatments need to address waste production concentration and body fluid volume. There are many methods:
Reduced intake of certain nutrients, especially proteins and ions, to reduce urea formation.
Drugs to reduce blood pressure:
Angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARB) reduce the effect of angiotensin, a hormone which constricts blood vessels to increase the blood pressure.
Calcium channel blockers dilate blood vessels to reduce blood pressure.
Beta blockers reduce adrenaline effects, as this increases heart rate.
Monitoring of both potassium and calcium ion concentrations as they are maintained by absorption in the small intestine and selective reabsorption in the kidneys.
High potassium is treated by a combination of glucose and insulin.
Untreated, this causes heart arrhythmias, so intravenous calcium is used to stabilise heart muscle membranes.
High calcium can cause heart disease, kidney stones and osteoporosis. It is treated by bisphosphonates.
This decreases the activity of osteoclasts, the cells that break down bone to recycle. Calcium therefore accumulates in bone, instead of in the blood.
Dialysis is where the blood is cleaned using a selectively permeable membrane and dialysis fluid.
Dialysis fluid has equal water potential to blood, but low iron and no urea. This allows for inorganic ions, water and urea to diffuse down their concentration gradients. Glucose is at a normal concentration, so none should diffuse out.
There are two types:
Haemodialysis, where blood is pumped out to a machine.
Continuous ambulatory peritoneal dialysis (CAPD) where capillaries in the stomach are utilised to perform dialysis inside the body.
Kidney transplant is offered to those with end stage renal disease.
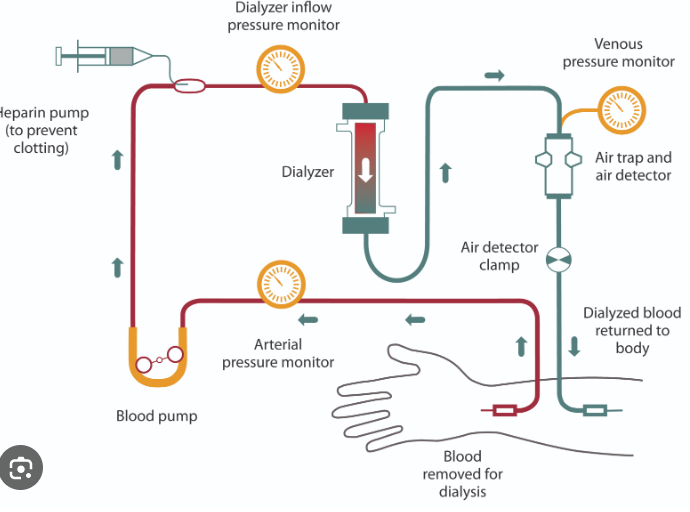
Haemodialysis
A dialysis machine is used, and the blood is cleaned in 3 steps:
Blood is taken from an artery, normally in the arm, into the dialysis machine.
It is then run through thousands of long, narrow fibres made from selectively permeable dialysis tubing.
The pores of the tubing allow small molecules into the dialysis fluid, but not larger proteins (similar to ultrafiltration).
Blood and dialysis fluid move through the machine in opposite directions to maintain a parallel flow (similar to water reabsorption).
The blood is then returned to a vein, and the dialysis fluid is drained to maintain normal concentrations.
Heparin is added to thin blood and prevent clotting.
There is a sensor in the dialysis fluid to detect haemoglobin that would diffuse through if red blood cells were damaged.
This machine is used several days a week, for hours at a time.
Continuous ambulatory peritoneal dialysis (CAPD)
This can be done while a patient performs everyday activities, and happens in 3 steps:
A patient drains a 1-3dm3 bag of dialysis fluid through a catheter in the abdomen into the body cavity.
There is the peritoneum, a membrane lining the body cavity with a rich capillary supply. This acts as the dialysis membrane.
Materials are removed from the capillaries and into the dialysis fluid.
After 40 minutes, the fluid is drained from the abdomen, using gravity, into an empty bag.
This happens 4 times a day.
Oedema is common and potassium ions can accumulate in the blood.
Liquid intake is therefore limited, and so is consumption of foods high in potassium.
Transplant
Kidney are placed in the lower abdomen in the groin, and the renal blood vessels are attached to the iliac blood vessels.
The ureter is then joined to the bladder once the kidney returns to a pink colour and urine is seen emerging from the ureter.
Donors and recipients
Donors can be living or be suffering from brain stem or circulatory death.
Live donor kidneys work immediately and last longer.
Deceased donor kidneys can take a few days or weeks to work and dialysis is used meanwhile.
Cytomegalovirus has infected 50% of the UK, and therefore a donor can infect a recipient.
Antivirals are often administered to avoid complications such as these.
Transplanted kidneys eventually fail, and the patient returns to dialysis.
Donors and recipients must have compatible ABO blood groups and in most of their HLA (human leukocyte antigens).
Higher risk donors are those over 50, or with high blood pressure or diabetes.
They have a higher failure rate.
Immunosuppressants
Transplant recipients must take immunosuppressive drugs for the rest of their life, and rejection can still occur. It is most common within the first 6 weeks.
Patients are more susceptible to infection, usually of urinary tracts.
As this can damage the kidney, low dose antibiotics can be used.
These can also increase risks of some cancers, such as skin cancer and lymphoma.
Adaptations for excretion and osmoregulation
Plants
They are producers, making all the protein they need and only synthesising amino acids and protein they need.
Active transport and facilitated diffusion allow them to take up all the necessary nitrate and ammonium ions from soil.
Ammonium ions are combined with a-ketoglutarate to make the amino acid glutamate.
This can be made into any amino acid by transanimating (an enzyme catalysed reaction that transfers an amino group to a-keto acid, making an amino acid) other a-keto acids.
Animals
As they are less efficient transanimators, excess amino acids are converted to a waste product as they cannot be stored.
Aquatic organisms
Freshwater fish and small organisms such as amoeba excrete ammonia.
It is highly toxic and highly soluble in water.
Due to the high SA of fish gills and amoeba ammonia diffuses out rapidly and diluted by water to below toxic concentrations.
Birds, reptiles and insects
Excess water is not carried, and they excrete uric acid.
It is almost insoluble in water and non-toxic.
It requires high energy to produce, but little water, which is necessary to conserve for animals who need to be light enough for flight or consume limited amounts of water.
Mammals
Urea is excreted, which requires energy but is less toxic than ammonia. It is soluble.
This allows tissues and bodily fluids to dilute it below toxic concentrations and briefly tolerate it.
Mammals in different conditions have additional adaptations.
Xerocoles
These are desert animals, which means they have very little water to consume.
Some live entirely on metabolic water produced during food breakdown and respiration.
Most are nocturnal, hiding in burrows or crevices during the day to avoid water loss via evaporation.
Loop of Henle adaptations
The longer the loop of Henle, the more opportunity for ions to be pumped into the medulla tissue fluid and therefore more water to be absorbed by the capillaries from the collecting duct and descending limb.
Cortical
These nephrons have the glomerulus in the outer cortex, and a short loop of Henle which just penetrates the medulla.
Most nephrons in humans are these.
Other animals that have these are beavers and muskrats as they have access to a lot of water.
They produce dilute urine.
Juxtamedullary
These nephrons have the glomerulus close to the cortex-medulla boundary, and a long loop of Henle which penetrates deep in the medulla.
Mammals in dry habitats have lots of these.
This allows them to conserve more water, and therefore produce extremely concentrated urine.