4. Neuro-Ophthalmology and Seventh Nerve Paresis
Seventh nerve paresis - facial weakness
Definition: Seventh nerve paresis refers to weakness in the muscles controlled by the facial nerve (Cranial Nerve VII).
It is also known as facial weakness.
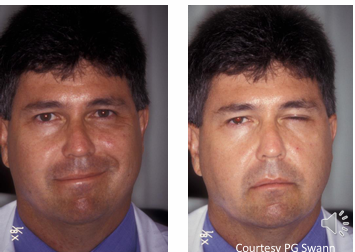
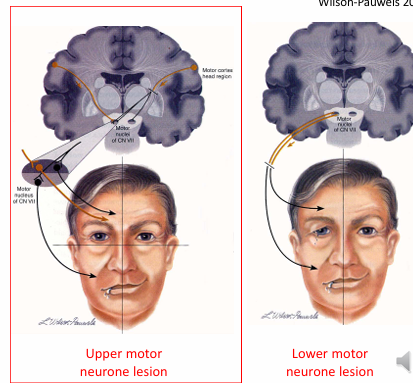
interruption of the seventh nerve itself (lower motor neurone paresis)
Involvement of all facial muscles on the affected side due to direct interruption of the seventh nerve.
Potential Causes:
Vascular Problems: Often associated with conditions like diabetes.
Trauma: Any injury that impacts the facial nerve.
Tumours: Growths that can compress the nerve.
Inflammation:
Viral Infections: Such as varicella zoster virus leading to Ramsay–Hunt syndrome.
Sarcoidosis.
Bell’s Palsy:
Diagnosis of exclusion.
Commonly idiopathic in nature
Clinical Considerations:
Ask the patient when symptoms began; rapid onset may suggest Bell’s palsy.
Evaluate for slow development of symptoms as it can indicate other, more serious issues.
Check the region of the ear for associated rashes or vesicles.
Symptoms and Signs
Ophthalmic:
Sore and/or watery eye
Blurred vision (corneal exposure)
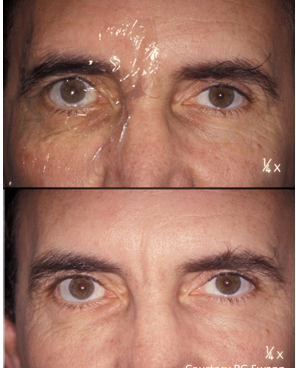
Incomplete eyelid closure
Lower lid paralytic ectropion
Cornea: punctate epithelial loss
Reduced tear film (if lacrimal gland affected)
Epiphora (lacrimal pump mechanism failure)
Other Symptoms
Problems with speech, eating, and drinking.
Drooping of the outer angle of the mouth.
Inability to purse lips or puff out cheeks.
Changes in taste perception.
Upper Motor Neuron Paresis: Seventh nerve paresis
Pathophysiology: Compromise of input from higher centres to the facial nerve nuclei leads to weakness of lower facial muscles on the contralateral side.
Common Cause: Most frequently caused by a stroke.
Key Distinction: The eye is not involved as the upper facial muscles, including the orbicularis oculi, receive bilateral innervation from the brainstem.
unlikely to present to optometrist as eye is not commonly affected.
Management of Seventh Nerve Paresis
Referral: All patients with new-onset facial nerve weakness should be assessed to identify the underlying cause.
Corneal Protection: Essential due to risk of exposure:
Possible methods include:
Wearing a patch.
Taping the eyelids closed at night.
Using copious lubricating eye drops.
Scleral contact lenses.
Surgical option: Tarsorrhaphy (surgical eyelid closure).
Bell’s Palsy
Description: Most common cause of facial nerve paresis, characterized by acute onset unilateral weakness.
Diagnosis: Considered idiopathic, making it a diagnosis of exclusion. Possibly due to viral or inflammatory conditions.
Typical Onset: Facial droop occurs within 72 hours.
Demographics: Most common between ages 15 and 60, affecting both sexes equally.
Prognosis: Approximately 70% of patients regain full facial function within three weeks.
Treatment Options:
Systemic steroids, usually prednisone.
Antivirals (e.g., acyclovir) may be prescribed, often in combination with steroids.

Acoustic Neuromas
Impact on Facial Nerve: Can lead to weakness in the facial nerve,
can affect CN V (trigeminal nerve), CN VI (abducens nerve), and CN VIII (vestibulocochlear nerve).
Symptoms Associated with Acoustic Neuromas: in addition to 7th nerve palsy patients
Tinnitus (ringing in the ears).
Hearing loss.
Diminished corneal sensitivity.
Diplopia (double vision).
Papilledema (swelling of optic nerve head).
Clinical Consideration: In patients with sixth and seventh nerve paresis, always check corneal sensitivity on both sides.