Scleritis and Episcleritis Notes
Scleritis
Definition: A rare but serious condition characterized by inflammation of the sclera that can lead to sight-threatening complications like uveitis, keratitis, and secondary glaucoma.
Demographics: Predominantly affects elderly patients, with a higher prevalence in females.
Associations: frequently linked to systemic diseases:
Connective tissue diseases such as rheumatoid arthritis, systemic lupus erythematosus (SLE), and systemic vasculitis (e.g., polyarteritis nodosa).
Local causes such as herpes zoster.
Classification of Scleritis
Anterior Scleritis (~98%)
Common Symptoms:
Red, inflamed eye, often unilateral.
Severe pain described as deep and boring, along with slight photophobia.
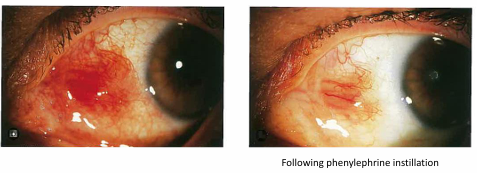
2.5% phenylephrine: non blanching evident.
Management: Refer urgently
oral NSAIDS
oral steroids, topical steroids.
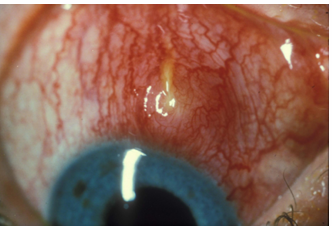
Types:
Diffuse: Most common & benign form
Widespread redness and inflammation
Distortion of normal radial vessel pattern
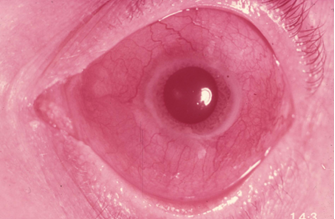
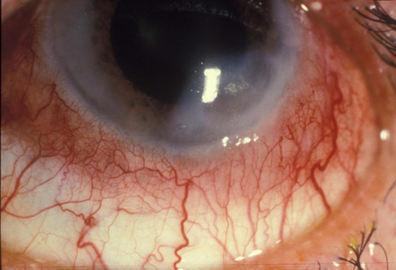
Nodular: Appears similar to nodular episcleritis
deep red immobile nodules (may be multiple)
very painful
Can be associated with uveitis
can get purulent discharge
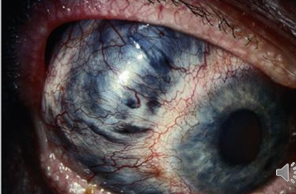
Necrotizing (with inflammation): The most severe form
Deep redness and inflammation, vascular distortion
Blood vessel occlusion and dropout can occur, resulting in white avascular patches
Results in scleral necrosis and thinning, and exposure of underlying uveal tract
Frequently associated with uveitis
Can be associated with keratitis (sclerosing keratitis), 2° Glaucoma, cataract
Sclerosing keratitis: opacity and thinning of the peripheral cornea adjacent to the site of scleritis.
Prognosis is generally poor
management: urgent referral. Oral Prednisolone and immunosuppressive agent.

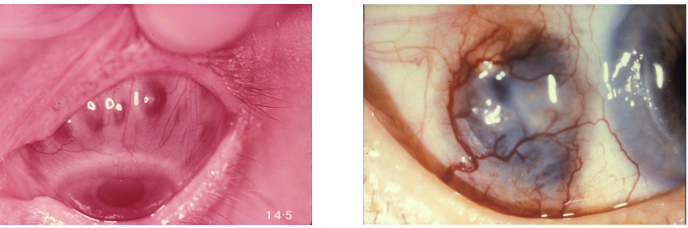
Necrotizing Anterior Scleritis Without Inflammation (scleromalacia perforans):
Characterized by progressive, non-inflammatory scleral thinning with blood vessel dropout and exposure of the underlying uveal tissue
Typically observed in longstanding rheumatoid arthritis, especially in elderly female patients.
Scleral necrosis can also occur following beta radiation therapy, particularly after pterygium surgery.
Can be asymptomatic or present with mild, non-specific irritation.
Overlying epithelium may ulcerate, leading to infection or chronic ulceration.
Urgent referral generally warranted: Aggressive treatment of the systemic disease is often required.
Protect eyes from trauma.
Posterior Scleritis (~2%)
Description: Inflammation of the posterior sclera. It may occur independently or alongside anterior scleritis but is often misdiagnosed due to similarities with other conditions (inflammatory or neoplastic).
Diagnosis: CT scan needed
May simulate tumour and cause choroidal effusions, (fluid collects in suprachoroidal space), angle closure glaucoma due to forward movement of the lens-iris diaphragm.
Symptoms: Variable presentation including pain and visual impairment.
Signs: Lid oedema, proptosis, ophthalmoplegia (restriction in eye movements), disc swelling, choroidal folds, exudative RD, choroidal detachment, subretinal lipid exudate.
associated with anterior scleritis ~ 30%
Management: Urgent referral is necessary.

Comparison: Episcleritis vs. Scleritis
Episcleritis:
Common (20-40 years), mainly females, mild pain (tenderness).
Excellent prognosis, with rare complications.
occasional systemic associations.
Scleritis:
Rare (20-60 years), mainly females, real pain.
Variable prognosis with common complications; systemic disease association, especially rheumatoid arthritis.
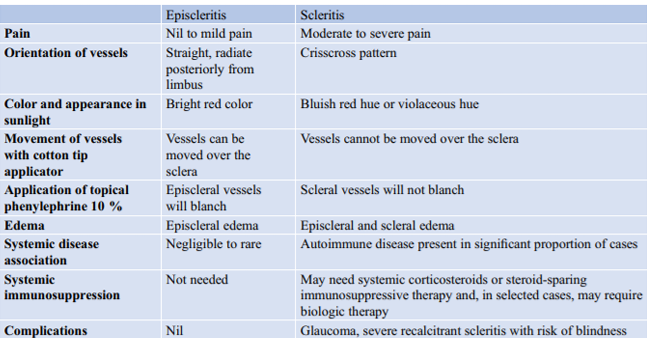
Key Features for Differentiation:
Pain Level: Episcleritis (nil to mild), Scleritis (moderate to severe).
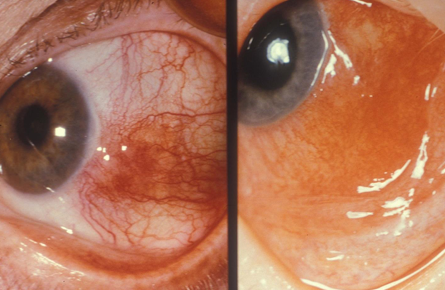
Vessel Orientation: Episcleritis (straight radiate), Scleritis (crisscross pattern).
Response to Phenylephrine: Episcleritis vessels blanch, scleritis vessels do not.
Systemic Disease Association: More common and severe in scleritis, often requiring systemic treatment.