Peripheral corneal changes and alterations
Dellen
Localized, saucer-like thinning (compacted stroma) of the peripheral cornea.
Due to tear film instability.
Affects the limbal cornea adjacent to a raised lesion (pingueculum, pterygium, episcleritis nodule, dermoid cyst, surgery, CL wear, dryness).
Treatment
Remove/treat the cause.
Non-preserved lubricants.
Marginal Keratitis
Common hypersensitivity to Staph toxins (usually from chronic adnexal disease).
Signs/Symptoms
Irritation/pain, redness, photophobia, lacrimation.
Peripheral, sterile sub-epithelial infiltrates with no overlying epi defect.
Circumferential spread.
Little staining.
Clear cornea to the limbus.
Vascularization across the limbus.
Treatment
Topical 0.5% chloramphenicol gutt AND 0.5% prednisolone gutt (or fluorometholone acetate 0.1%), both , should lead to a resolution within 10 days.
Stringent attention to the eyelid margin disease.
Oral doxycycline for three months.

Rosacea Keratitis
Rosacea: long-term skin condition that typically affects the face.
More common in middle-aged women (but possible at any age).
Cheek and forehead flush (masked with makeup).
Rhinophyma in men.
Worsened by spicy food, alcohol, sun, emotional stress, and hot weather.
Ocular involvement: 18% of cases (blepharoconjunctivitis and keratitis (10%)).
Signs/Symptoms
Punctate epithelial keratopathy.
Inferior peripheral neovascularization.
Recurrent erosions.
Corneal thinning and perforation (rare).
Treatment
Weak topical steroid and short course of broad-spectrum antibiotic for blepharitis.
Systemic tetracycline (doxycycline).
0.05% cyclosporine for ocular rosacea.
not curative → focused on management


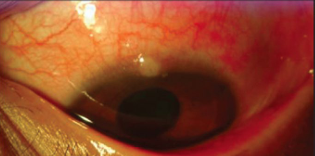
Phlyctenular Disease
Delayed hypersensitivity reaction to bacterial antigens.
Developed world: mostly in children, Staph blepharitis.
Developing world: helminth and TB.
More frequent in children and young adults.
Signs/Symptoms
Pinkish/yellow (then grey/white) inflammatory lesion just inside the limbus (or on, or outside).
Bridging localized vascularization.
Photophobia, lacrimation, irritation.
Treatment
Eradicate causative organism.
Topical steroid (FML acetate 0.1%).
Staph coverage with ciprofloxacin.
Systemic doxycycline if Staph phlyctens are persistent.
If the patient has visited an area where TB is endemic, they should be referred for a chest X-ray and Mantoux test.
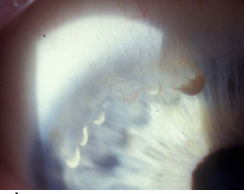
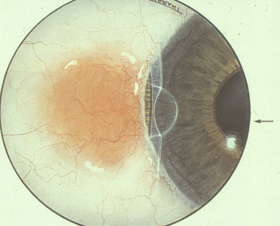
Terrien’s Marginal Degeneration
Uncommon.
Most cases are male, usually over 40.
Bilateral, slow progression.
Signs/Symptoms
Superior nasal (usual) thinning of the peripheral corneal stroma with an intact epithelium.
Upper corneal punctate stromal opacities, mild vascularization, gutter formation, circumferential spread.
Vision loss from irregular astigmatism.
Typically patients are asymptomatic.
Treatment
Rigid CLs for irregular astigmatism.
Inflammatory episodes can be managed with prednisolone acetate or lotemax (loteprednol - significant IOP rise less common).