all compiled notes for PSCY 350 FINAL.docx
Chapter 1:
The three key sources of misinformation in media are Religion/culture, Media, and the Internet
Ethnocentrism in sexual messaging: the issue in Western worlds where there is a disregard for diversity as we only view our vantage point as normal
- There is an issue with heterosexual frameworks as compulsory
- Issues with there being religious overtones to our gender expression and sexual experiences have the potential to impact real-world experiences amongst individuals who ARE diverse in sexuality and expression
- ALL societies regulate sexuality to some degree, whether it is positive or not
Two Spirit is a term to reclaim an identity stolen and watered down through colonization: there is a problem with naming and boundaries in Western labeling, the term two Spirit captures how all life is sacred. It is a term that not only describes gender or attraction but also their intersections. A return to two-spiritedness = a return from a harmful and violent Western violence
- Two spirited individuals were well-respected warriors and leaders; it wasn’t until colonization that these aspects of their identity became labeled a certain way
Indian Act was an effort to make heterosexuality compulsory in Indigenous communities; there was an imposition of Western values on groups of people who had previously shown lots of diversity in their identity
When referencing culture and sexuality, it is important to know that many cultures differ in the presentation and practices of gender and sexual practices
- Cook Islands: girls are encouraged to experiment and explore sexuality, and boys are taught to prioritize female pleasure
- India: a celebration of the positive aspects of sex (there are festivals) eg. while western worlds may see India as more conservative, these beliefs are also an example of the influence of ethnocentrism
- Nepal/India/Himalayas: presence of unique constellations and polyandry
- Understandings of sex is unique amongst every group of people; in the sambia tribe, young boys have to give fellatio to older men as part of a ritual that makes them into strong men. In indonesia, some islamic groups were pilgrams to have sex with a stranger which would bring them luck. In some places, kissing on the lips does not occur.
RESEARCH STUDY FINDING: what are the general trends of attitude shifts within culture over time? Findings of this study: attitudes toward sex before marriage became more positive over time, attitudes about same-sex marriage became more positive over time, attitudes about sex between teens became slightly more positive over time, attitudes about extramarital non-consensual non-monogamy were slightly negative however not significant (did not shift much). OVERALL: The findings of this study showed that while some trends shift, not all do.
What is religion’s impact on sexual messaging?
Under Christianity, women experience less sexual freedom as they are seen as responsible for the origination of sin, there is an understanding of Eve as the initiator of temptation, hence, under Christianity, purity is emphasized, and women should not be interested in casual sex, “your purity is attached to your worth” + strong negative views to contraception + dichotomization of women’s sexuality; you only have the pure madonna and the whore
- The concept of the missionary face-to-face position was rooted in acknowledging a man's superiority to women.
- Sex is to procreate, as such abortion is bad as it is a waste of seed and it would then entail that sex was a product of lust
Under Judaism, there are more positive views surrounding sexuality, it is part of God's creation. There is more understanding that sex is for pleasure however there are still certain contradictory beliefs: no incest, no bestiality, no men on men, no adultery (all of these are punishable by death) however, women are allowed to have sex with women. There is also an understanding that wet dreams and menstruation are all behaviours that require spiritual cleansing. In the present time, Judaism is practiced to reinforce the marital bond, it is permitted while pregnant, or after menopause
Under Islam: there was a promotion of sex provided that it occurs within a marriage except during the time of menstruation. There is emphasis on foreplay and emphasis on pleasure being between men and women, there should be a focus on providing orgasm to a man’s wife or wives. Birth control is acceptable but only with the permission of his wife, and so that her pleasure is not reduced. Despite how many Muslims condemn the same gender-sex sexual activity, many still hold the belief that it is not unlawful and should not be punished by death. Islam viewed adam and eve as equally being responsible, however this shift also led to the interpretation of eve as the source of sin over time.
Under Hinduism: Sex is viewed as the basis of life, however, it must occur under religious duty and context (which was commonly believed to be under marriage). Sex outside of marriage is condemned and understandings of masturbation depend on the context. Marriage is considered sacred, women should not have sex during their periods (as this is not pure). There is descriptions of same gender sex orientation as natural, however also statements that should avoided. A unique view under Hinduism is there being a space for heterosexual men to have sexual relations with those that identified as a third gender known as the Hijra; Hijra → Hindu faith!
RESEARCH STUDY FINDING: how does sex guilt shape sexual activity? The findings of this study show that the more sex guilt an individual has, the less sexual experience they have, the less they feel arousal to porn, the less they have positive emotional experiences to porn, the less knowledge they have around sex, the less positive attitude they have to when they feel sex is ok. The higher their levels of religiosity are!!! OVERALL: it seems that religion is a factor that impacts how we understand sex + there is an association between sex guilt and religiosity
How does Media influence sexuality?
Media allows us to see what is normal, what we think of as “good” or “bad” often stems from what we see within media. It influences what we believe we should and shouldn't desire
- Advertising: historically, media focused on sexuality was heavily censored in Western (us) societies, there was a strong maintenance of the double standard: women’s sexuality was often controlled by men, and sex toys and other objects that were used sexually were advertised to men
- Double standard: men were allowed to express themselves more than women, and they had more freedom, → this has an impact on how people view sex + tied to the presence of sex guilt
Media and sex within media: There is a portrayal of a fantasy model of sex in which sex appears sti and pregnancy risk-free – VERY HARMFUL. Throughout history, gender roles and sexuality were able to be explored much more in anime for example than on film and television in NA. NA historically had more censorship and less nudity of men, however, this same nudity did not apply to women. There is also a focus in Hollywood even today, on white characters.
Kinsey and the beginning of sex research in the 1950s: his research was focused on interview-styled approaches that viewed sex from a more diverse lens than ever before. His work increased the understanding and acceptance of diversity in human sexuality. Gathered 18,000 reports (8000 himself), “We are recorders and reporters, not judges…”, he was openly bisexual.
- Kinsey studied the sexual behaviour of the males and sexual behaviour of the female
- Kinsey created an attraction scale “Kinsey Scale”
- He also documented and normalized various sexual behaviors and attractions
Understandings of sex and the internet have many positives and negatives:
Positives: more information in a search, normalization of diversity, more ways to meet new people
Negatives: misinformation/unrealistic scripts, stereotypes of sex, access to vulnerable people (risk for sexual assault)
An issue with the internet and the depiction of sex within it is that there is the issue of removal and shadowbanning, which typically affects marginalized communities more than not. (this also adds to the idea of sti-free unplanned pregnancy-risk free sex due to lack of education)
Teens in the united states are twice as likely to get pregnant as teens in Canada
In terms of viewing sexually explicit media on the internet, there are a few variations: erotica vs pornography. While erotica is more equal (women’s pleasure is prioritized just as much as men’s pleasure is), pornography is more centered on men’s pleasure (inequality, violence)
META ANALYSIS RESEARCH STUDY FINDING: what are the effects of sexually explicit media on the sexual/relational satisfaction of individuals? Findings: sexual media has a small negative effect on the satisfaction of individuals however this was ONLY significant for men (men r= -.13, women r= -.01)
RESEARCH STUDY FINDING: is there a link between Sexually explicit messages and actual sexual behavior? Findings: The frequency of consuming SEM is very small in its association with adventurous sexual behavior → there is more variance in other factors. However, there was more effect on women than men.
Sexual health is so fundamentally important as it ties to aspects of physical and mental health as well. Good sexual health = good building blocks to healthy and strong relationships
In reference to sexual diversity, there has been an ongoing fight in Canada to emphasize queer folks. The Canadian Syrian Refugee policy was revised to emphasize gay men in addition to women, young children, and families.
Chapter 2:
There are three major theoretical approaches to sex: learning, cognitive, and evolutionary however no one of these theories can explain every phenomenon.
A scientific theory is an intellectual framework from former observations and evidence about a phenomenon; within the field of sexual psychology, theories help us organize, generate, and communicate truths about sexuality. They are still able to be changed and refined
A good theory should be: testable, coherent, generalizable
- Theories allow us to test a hypothesis
- Theories → predictions → designed study/experiment to test it → results/observation → modification of the theory
- Theories take on a circular-like structure
Psychological theories and Freud (id, ego, superego; psychoanalysis can bring out parts of someone’s subconscious)
Learning theories: explain how sexual behaviour can be affected by basic learning
Classical conditioning: stimuli get paired in a certain way that makes it so there's a conditioned reaction to a neutral object
- Unconditioned stimulus (meat), unconditioned response (salivation)
- Meat is paired with a neutral stimulus (bell), conditioned response (salivation)
- The act of neutral stimulus eliciting a conditioned response
- Bem’s understanding of classical condition and gender/sexuality (which was highly problematic) was how he understood gender non-conformity or sexuality amongst children to be the outcome of them partaking in certain activities which would then classically condition them to think a certain way.
Classical conditioning in a shoe fetish:
- Unconditioned stimulus (woman), unconditioned response (arousal)
- Neutral stimulus (shoe), conditioned response (arousal)
There is an arousal to a shoe, it gains a level of arousal capacity, preferences for specific objects can work through this way
Operant conditioning is all about how a behavior can be changed based on reinforcement and punishment: reinforcement (increase behavior), punishment (less behavior)
Positive reinforcement: the more something is done, the more rewarded it is
Negative reinforcement: something unpleasant is removed which increases a specific behavior as it feels good to have smth removed
Punishment; something is added but is negative
Primary reinforcers are intrinsic, sex and orgasm a powerful primary reinforcers and sex is also something that can be shaped by reward and punishment; this implies that sex is both innate and learned
Operant conditioning example in sexuality: If someone were to masturbate every time he gets stressed from work to remove his stress, the masturbation removes stress hence it is a negative reinforcer for that behavior.
Example of an if-then hypothesis statement for classical conditioning: If a cisgender heterosexual man who is attracted to women is repeatedly introduced to the smell of steak while undergoing intercourse, then the smell of steak will, through classical conditioning, eventually elicit similar feelings of arousal or sexual excitement even in the absence of sexual activity.
Example of an if-then hypothesis statement for operant conditioning: If a cisgender heterosexual man who is attracted to women is greeted by a blaring horn that honks at him telling him he is gay every time he attempts to enter a specific club, then entering this club will, through positive punishment, operantly condition him to go to this club less.
Social Learning theory: Social learning theory posits that human behaviour is learned by observing other people’s behaviours, attitudes, and outcomes. When it comes to choosing one learned behaviour over another, we do so based on our individual expectations about rewards or punishments. These are the basis for promoting healthy behaviour. If a person performs a specific behaviour will experience a sense of competence, or self-efficacy. In the sexual context, high levels of sexual self-efficacy, the belief that one is sexually competent and capable, have been associated with positive sexual adjustment and sexual satisfaction.
Social exchange theory: describes how in any relationship, individuals try to minimize cost and maximize rewards. comparison level refers to what a person expects to get out of the relationship in comparison to what they put into it, and comparison level for alternatives refers to how a person feels that the current relationship compares to other available options. People are more likely to be satisfied and to stay in the relationship if their expectations, or comparison levels, of what they should contribute to and receive from a relationship are being met.
Cognitive theories: thoughts, an attempt to understand human behavior by understanding an individual's thoughts regarding sex; it is attempting to understand our emotions in the context of sex. (when something is inaccurate, it can affect our understanding of sex)
- Dyspareunia: Genital and/or pelvic pain during or after sexual activity involving penetration. May have a woman feeling like she is incapable/ a bad partner as she is unable to orgasm due to pain→ negative thoughts → feedback loop that makes her even more incapable as she only allows herself partake in penetration
RESEARCH STUDY RESULTS about the cognitive theoretical approach in sexual behaviour: how does what we believe about sex and our sexual response during sex be affected by our level of distraction during sex “What's for dinner, how does my body look…”. Findings: there was not a major cognitive distraction difference between men and women, sexual beliefs were significantly negatively associated with good sexual functioning in both women and men, higher levels of cognitive distraction was significantly negatively associated with good sexual functioning in both women and men, cognitive distraction only mediated the path between sexual beliefs and sexual functioning in women (men werent influenced by this tie); this implies that there may be different pathways between sexes or different factors
Cognitive behavioural therapy focuses on evaluating and testing unhelpful thoughts that influence behaviour. EG. an individual has the belief that you should only come from penetrative sex → behaviour: they only partake in penetrative sex → thoughts: why am i not reaching an orgasm??? → behaviour: avoids all other behaviour that may lead to an orgasm → Outcome: no orgasm from PVI: if you dont do other behaviours, overthink beliefs based off lack of knowledge and porn, etc.
- To treat patients that come in from this form of sexual dysfunction
- challenging unhelpful thoughts and making room for flexibility
- Trying new things may reinforce new beliefs if they are able to try novel things that allow sex to feel more novel, special, and intimate.
If then hypothesis statement for cognitive theories: If an individual harbors negative beliefs regarding previous sexual encounters, then sex will reflect negative sexual functioning.
Genetic theory: explains how our genetics plays a large part in regulating hormone production, reproductive cycles, ovulation, ejaculation, conception, and pregnancy. According to this theory, genetics can also explain sexual orientation and gender identity. Studies have shown that identical twins have higher concordance rates for having the same sexual identity/gender identtiy + there is recent evidence suggesting that a specific gene on chromosome 8 is more likely to make men gay (not solidified)
Evolutionary theories: describe how all living things have evolved over our history and how these evolved characteristics have shifted based on how adaptive they are for our reproduction and survival
Sexual selection is when traits evolve as they increase the success in mating; it is a component of natural selection + its responsible for our conspicuous sex differences (height, muscle, weight, etc)
- There are two types of sexual selection: intersexual selection and intrasexual selection
- Intrasexual selection helps individuals vanquish same-sex rivals that are going for the same mates, any trait that offers an advantage in direct competition → in humans these could be how deep our voices are, and the display of money or other resources; this could be elephant seals and their sizes
- Intersexual selection is any trait that evolves because it helps individuals attract members of the opposite sex as mates → this could be having a symmetrical face shape; this could be birds of paradise and their energy-consuming dance
Sociobiological theory recognizes that, generally speaking, reproduction takes a greater investment of time and effort from a female than from a male. After all, it is the female who becomes pregnant and gives birth, and in many species the female is most responsible for the care of the offspring. When choosing a mate, therefore, a female should look for a male who will contribute good genes and can provide useful resources and protection to make sure her offspring will survive and reproduce in turn.
Parental investment theory emphasizes how decisions are influenced by how much these individuals have on the line in relation to mating
- The fastest (sex with the lower minimum necessary investment) sex will have the heaviest sexual selection pressure → reflects the male body as they have a smaller gamete to offer
- The slower sex (sex with a higher minimum necessary investment will be CHOOSIER) will have more intersexual selection pressure → reflects the female body as they have larger gametes, 9 months of pregnancy, lactation
Sexual strategies theory incorporates how mating strategies have evolved to overcome mating problems faced by ancestors → problems in males with paternity certainty (how to know how much resources to invest when there isn't a 100% certainty → establishment of longer partnerships); for females: assessing quality within a framework to see who is a long-term vs short -term partner.
- This also suggests that people pursue short and long-term mating strategies because of asymmetries in investment
- Eg. faster sex will dedicate more time to short-term mating; men: more casual sex = most chance of high output with little investment; MEN ARE MOST INTERESTED IN CASUAL SEX, men are much more likely to consent to intercourse than women are even after short term meetings; consistently, men desire more partners than women
- Shaped by asymmetries and differences in parental investment
CLASSIC STUDY EXPERIMENT: would strangers be willing to have sex casually? Findings: a much higher degree of men were down for casual sex than women; men have a greater openness to casual sex encounters → men are more likely to take the opportunity
- Women discriminate more as short-term sexual experiences only allow them to gain good genes in exchange for all else.
dual control model of sexuality: each person’s sexual responses involve an interaction between sexual excitatory and sexual inhibitory neurobiological processes. This understanding suggests that in times of war and famine, people suppress mating tendencies, while in other times, they may exhibit it. Also suggests that every individual has unique factors that excite/inhibit them.
Sociological theory highlights the importance of social institutions, such as family and religion, in regulating sexuality. Sexuality is linked to societal structures of power, kinship, and ideology, and these structures determine, to a large degree, how sexuality is defined, expressed, and regulated within a certain culture or community.
social script theory: suggests that there are specific sequences of behaviours, based on societal beliefs and values, that individuals consider appropriate for particular sexual situations. When a sexual encounter occurs between people of the same societal background, the individuals involved can use these scripts to interpret the sexual situation.
- When couples have a genera; understanding that they will progress from kissing to touching to oral sex and then to sexual intercourse, not necessarily all in one evening but generally in that order. When the partners follow the sexual script, they generally know what to expect and can be assured that their date and/or relationship is progressing well.
Ecological theory: each individual has 4 factors (with them at the center) that influence their decisions. At the microsystem level, an individual’s psychological well-being and sexual satisfaction can influence their sexual function. If we consider partner characteristics at the mesosystem level, relationship status (e.g., being married or in a committed relationship) and relationship satisfaction can affect sexual function. At the exosystem level, social support of the relationship can influence sexual function, which may be especially relevant for same-gender/sex couples. Finally, at the macrosystem level, the dominant culture, including largely held religious beliefs and cultural norms about “appropriate” sexual behaviour, may affect one’s sexual function
Feminist theory: examine the inequalities of relationships between men and women and their effects on women’s sexuality, there is an understanding that sex fundamentally prioritizes men over women
Queer theory: challenges all notions of gender, sexual orientation, and sexual behaviour as being socially constructed and embedded within societies and offers a framework to critically examine research and ideas by highlighting that identities and experiences are not fixed and categorical. Queer theory can assist in clarifying notions of nonconformity and diversity
Motivation theory: People engage in a behaviour for self-determined, autonomous reasons: the behaviour is fun, congruent with their values, and personally important. On the other hand, people also engage in activities from controlled motives; they feel external pressures such as promised rewards or avoidance of negative consequences. They might also feel internal pressures such as a need for self-validation or to avoid shame and guilt. Embedding our autonomous power into our actions!!!
Chapter 3:
There are three different types of sex research design methods: Descriptive, Correlational, and Experimental
Descriptive sex research design includes interviews, direct observation, and case studies
Correlational sex research designs include surveys
Experimental sex research design includes sexual psychophysiology, brain imaging
The interview method of descriptive research design is meant to collect detailed self-reported data. It holds the advantage of being able to ask additional questions in order to better summarize, however, it is limited by recall and memory bias (there are perhaps instances where interviewees will be unable to recall a specific experience), there is also risk for responder bias (social desirability/answering what interviewer wants to hear)
- The Kinsey scale was a descriptive scale that asked questions about marriage, sexual health, sexual orientation, sexual behaviour, it was based on both qualitative and quantitative methodologies; it worked from the assumption that everyone engaged in a wide variety of sexual behaviour
- Criticisms of the kinsey scale were that it oversampled white men and women, there was outdated language, it described attraction as behaviour (which we know is not true), and it assigned asexuality as X (and was single axis)
The direct observation method of descriptive research design is the most basic and non-intrusive descriptive method. It involves monitoring and recording patterns of sexual behaviour. It is strong as it is highly ecologically valid, can code behaviours, reduces bias, however it is also weak in how the research cannot manipulate behaviours and how knowing one is being watched can also shift the observation of the participants being watched
- Be careful for interpretation bias, all actions should be operationalized still
- Observational methods were utilized by Masters and Johnson were they empirically observed 700 people masturbate and have sexual interaction to speculate patterns about sexual response and abnormal sexual function + measured physiology; some critiques of this included the oversampling of white individuals, the focus of orgasm over sex, the emphasis of physiological aspects of sex and the pathologizing variation in sexual behaviour (critique and classification of things as abnormal)
- The 3 resolution graph for female orgasms and the 1-2 orgasm graph for male ejaculation were general outcomes from their study
Dr Kate Frank used observational techniques in her research on sex work, stripping, non-monogamy etc. She was an erotic dancer who interacted and engaged with individuals. She was in her natural environment, she was not regarding things from an outside perspective, interactions she received were more comfortable; HOWEVER, some downsides were her ability to effectively influence responses, had to be careful about her biases, and there was a risk for memory bias
Case studies as a descriptive research design method examine a single individual, time, or event over a period of time( LONGITUDINAL) in order to provide insight on things that are rare and uncommon (that could potentially be built further within further study; they are just meant to lay down a fundamental framework for a concept)
- Criticisms of case studies involve how there a poor generalizability, there’s a lack of a control group or experimental design (we cannot establish causality), there’s interpretation bias
Content analysis, a common component of descriptive studies, allows researchers to systematically sort through the information they collect from their research in the form of observational notes, transcripts of interviews or focus group sessions, participants’ personal narratives, audio recordings, and/or video recordings.
- Content analysis can be used qualitatively to uncover patterns or themes that naturally emerge from the research and to develop new ways of describing certain phenomena. It can also be used quantitatively to sort data into predetermined categories, although much of the richness of the original descriptions can be lost in such an approach.
The importance of definition in sex research ties to how things like casual sex may mean and be defined differently amongst different groups of people. Validity is important, construct is important
In terms of surveys we have correlational (relationship establishment), standardized (meaningful, same fixed questions), validity (what are we measuring????), unstandardized (fixed questions with fixed open and fixed responses), sampling (convenience, random…)
- Surveys can be high on demand characteristics
Archival data-mining offers a window into the past, and this method can be a rich source of correlational information. Archival analysis can incorporate quantitative information (e.g., age of first diagnosis, presence of positive cultures from genital exams, number of previous sexual partners) as well as qualitative information (e.g., descriptions of interventions as “biomedical” or “behavioural” treatments), with the aim of uncovering trends in data across time, evaluating relationships between sexual health and demographic variables, and assessing the possible outcomes of a given treatment.
- E.g condom use increase
Quasi-experiments are frequently used to study many pre-existing participant characteristics, such as sex, age, behavioural history, and the presence of clinically meaningful sexual dysfunction. In such studies, researchers identify naturally occurring groups of interest within a population and assign individuals to either an experimental group or a non–randomly selected control group.
The importance of measuring through psychophysiological methods (through genital response measuring, eye tracking, and brain imaging) is how direct these measures are. If we were to alternatively measure from a heart rate, we would experience some issues with internal validity as we cannot determine that a heart rate is directly linked to arousal (there could be other reasons)
Psychophysiology is defined as the application of psychophysiological methods to study sexual arousal; there is a specific emphasis on the interplay between subjective experience and physiological determinants of sexual arousal.
- Some ways we can measure genital response:
- Vaginal only: vaginal/clitoral photoplethysmography, vaginal lubrication
- Penile only: penile strain gauge
- vaginal/vulvar and penile: thermography and laser doppler imaging (non-contact)
Vaginal only:
- Vaginal/clitoral photoplethysmography: widely used as an indirect measure to measure sexual response to stimuli as an on/off switch, it is a good indicator of the presence of arousal but not a good indicator of the level/ degree of it. Vaginal walls change during arousal, this measures blood flow. WEAK CORRELATION TO SELF REPORTED AROUSAL
- Vaginal Lubrication: degree of colour change on the test strip shows amount of lubrication, it could be recorded pre and post exposure to sexual stimuli. WEAKNESSES however are how this vaginal lubrication can be recorded ONCE, it is no continuous. STRONG POSITIVE CORRELATION TO SELF REPORT
Penis only:
- Penile Strain Gauge: Widely used to measure the change in circumference during an erection. It does NOT PROVIDE INFORMATION ON HARDNESS OR HOW RIGID THE PENIS GETS. the calibration reflects girth change.. STRONG POSITIVE CORRELATION TO SELF REPORT
- Penile volume plethysmography: The penis is inserted into a container; as penis volume increases, the amount of “free” space in the container decreases. As arousal-related blood flow increases, the penis increases in size, Reliable; accounts for arousal-related changes in penile length and girth but not firmness
BOTH:
- Thermography: infrared heat sensing camera records the shifts in genital temperature. During arousal, genital changes (a couple degrees) based off of arousal. WEAKNESS IS that these changes can be very slow and are limited in range of what can be recorded + STRONG POSITIVE CORRELATION TO SELF-REPORT
- Laser Doppler imaging: low power infrared laser beam that images blood 2-3mm below skin surface, it can detect the blood flow and has a STRONG POSITIVE CORRELATION TO SELF-REPORT. This measure allows us to measure change over time however a key weakness is its inability to measure CONTINUOUSLY. There will be instances in which the penis moves, and there will be minutes between image recording (90 seconds) in which degree of change is not recorded through the machine
- Quantitative sensory testing (QST) requires that an individual make perceptual judgments on whether a stimulus is detectable, whether the stimulus is more or less intense than a previous sensation, and in some cases whether the stimulus is painful. Genital QST provides information about how the body processes sensations at rest and during a sexually aroused state, which can vary based on the type of stimulus (e.g., pressure, heat, vibration) and the characteristics of the examined skin (e.g., external or mucosal). Notably, the perception of sensation can be influenced by psychological factors that also influence sexuality, including attention, distraction, and mood. It is known that more pressure is needed for men to detect, while less is needed for women
Bouchard RESEARCH STUDY RESULT: Can we detect bisexual patterns in cis women? Findings: When using audio stimuli, researchers are able to have more control of the respective recordings; it was discovered that bisexuality is a spectrum and there was some level of alignment in fantasy, behavior, and orientation, MOREOVER… genital response to female stimuli (recordings featuring women) elicited more response
RESEARCH STUDY RESULT: bisexual orientation among men using a penile string gage and an updated version of the Kinsey scale? Findings: there was a pretty good indication of 3 on a Kinsey scale reflecting equal attraction amongst bisexual men. A unique finding was that even for those that reported being a 0 or a 6, there was still some slight attraction to the contrary of what they reported within the data itself; sexuality doesn't seem to be an all-or-nothing
RESEARCH STUDY RESULT: eyetracking as a means of measuring bisexuality in both men and women. Findings: In eye tracking and pupil dilation, the same measure was used for everyone and there was signs that self-reported bisexuality corresponded to the 3 on the kinsey scale (0-6)
RESEARCH STUDY RESULTS: using the fMRI to understand sexual patterns. Findings: in men, those who reported as heterosexual responded to female stimuli… bisexual men responded with both, and gay men responded more to men; however, in women, the fMRI showed that women showed more arousal to female stimuli. While bisexual men showed an equal response, bisexual women showed more reaction to female stimuli
Vaginal photoplethysmography/penile strain gauge: women show arousal to both male/female stimuli but greater to women; men show bisexual patterns of arousal. not measured on the same structure
Eye tracking: evidence of bisexual patterns of pupil dilation, same measure and homologous structure
Brain imaging: evidence of bisexual activation patterns in men but women had greater activation to female stimuli, same measure used
Chapter 4:
Masters and Johnson - 4 phase model Human sexual response model: excitement, plateau, orgasm, resolution.
myotonia (general muscle tension increase in both sexes during the excitement stage) and vasocongestion. Myotonia and vasocongestion were the two fundamental processes
- Their work was unique as it was measurable, empirical
- Myotonia= muscle spasms
Kaplan- 3 stage model: desire, excitement, orgasm; this incorporated psychological processes.
Basson’s circular model: Sexual arousal can start anywhere; there is a fundamental understanding that there can be spontaneous innate desire, they can have an intimate connection, they can feel obligated to do so, there can be distraction from stress → there may be a want to experiment and explore. Basson’s circular model was special as it incorporated NON-SEXUAL reasons for engaging in sexual activity.
- Your actions are motive-driven
- Key strength: desire can emerge from sexual arousal. RESPONSIVE DESIRE MODEL: Once you are turned on, you can feel the emergence of physical or psychological arousal
- This model highlights how there is a need for sexual arousal, there needs to be something there that sexual arousal can emerge from
- Sexual response involves both physiological processes like vasocongestion (increased blood flow) and myotonia (muscle tension), as well as psychological, cognitive, emotional, and experiential processes.
The other model’s weaknesses tie to how they follow a script regarding what should happen following something else
RESEARCH STUDY RESULTS: what does the endorsement of the models look like amongst individuals? Findings: Many more women endorsed the Basson model than others, however, there were more results endorsing the M&J and the Kapplan models. Compared to our class sample (most of us endorsed the Basson model), the sample within this survey study likely had more people of older ages (20-60), age is a big mediator, education is a big mediator, cultural differences, etc.
The external female genitals are called the VULVA, the internal is called the vagina
What are the three theories of the mon pubis (pubic hair) existence: used to communicate pheromones, used as padding, used to communicate sexual maturity
The clitoris: it is a complex structure that is mostly internal, it is externally visible only at the clitoris and it takes on a wishbone structure. The clitoris contains erectile tissue (it gets larger during vasocongestion, it has far more nerve endings than the vagina (More sensitive, a better source of pleasure), and the clitoris’s only function is pleasure.
Smegma sometimes accumulates under the clitoral hood; this buildup can be prevented by pulling back on the hood when washing the genital area.
Labia majora: the outer lips of the vagina, protects the sensitive clitoris, labia minora, the opening to the vagina (vulva vestibule).
Labia minora: there is a lot of variability. They are hairless folds of skin between the labia majora. They are important in sexual stimulation and arousal
Vulva vestibule: the region that is within the labia minora (loose diamond shape inside the labia majora), has a lot of nerve endings and blood vessel
The Bartholin Glands: small glands that are beside the left and right sides of the vagina, their function is unknown however they MAY contribute to the lubrication of the vagina
The skene’s gland: is known to perhaps contribute to the arousal of the vagina→it contributes to the sensitivity of the G spot; it MAY be the equivalent of THE FEMALE PROSTATE (it is included in the G spot)
The cervix is the opening to the uterus
The uterus is located at the top of the vagina and contains mucus-secreting glands. Sperm travel from the vagina into the uterus through the os (the opening in the centre of the cervix). The upper two-thirds of the uterus is the fundus, or body. The major function of the uterus is to hold and nourish a developing fetus during pregnancy.
Cervical cancer: one of the first signs is cervical dysplasia in which there abnormal cell growth in the cervix, this is discovered through pap smears
Ovaries: Females usually have two ovaries, one on each side of their uterus (Figure 4.5). The ovaries are endocrine glands that produce estrogens, most notably estradiol, and progestins, mainly progesterone.
The fallopian tubes, also called the oviducts or the uterine tubes, transport the ova from the ovaries to the uterus. They are about 10 centimeters long, with one located on each side of the pelvic cavity; they are most likely where the sperm fertilizes the egg
What is douching: douching is the cleaning of the vagina; it attempts to remove the bacteria inside the vagina (this bacteria actually helps prevent infection. douching increases risk of endometriosis, increased risk of sti
labiaplasty. This surgery encompasses a variety of procedures, and it is usually done to make the labia minora plumper, more symmetrical, and/or smaller. Risks associated with labiaplasty include infection, decrease in pleasurable sensations, scarring, and unpleasant hypersensitivity in the area; usually done out of concern for appearance of labia minora / or due to the part bothering an individual during non-sexual activity
The hymen is a thin membrane that partially covers the vaginal opening. It is believed to protect the vaginal tissues early in life. It is usually present at birth, and it generally remains intact until first intercourse, when it is commonly torn. Some people, however, are born without a hymen, and some who are born with one may unknowingly tear it during sporting or other nonsexual activities. Thus, the assumption that a person without an intact hymen is not a “virgin” is not always correct.
The vagina consists of three layers of tissue. The outermost layer is the vaginal mucosa, which is similar in texture to the tissue inside the mouth. The rugae (ridged walls) of this layer are soft and moist. These walls release secretions to maintain a healthy, slightly acidic chemical balance. Other than regularly washing between the vulvar folds, nothing needs to be done to keep this balance.
The penis: the male external organ is made up of the penis and scrotum (has testes inside) has 3 functions: reproduction, pleasure, urination. The glans of the penis are the most sensitive (the tip) to stimulation, the entire shaft is very sensitive. The average penis size is 9.2 cm flaccid and 13 cm erect; the angle of erection is 10 degrees above horizontal when standing, when not fully erect this could be less (and also a sign of erectile dysfunction if not consistent)
Many neurotransmitters are involved in the process of an erection (vasocongestion), the main one being nitric oxide, which causes the smooth muscles in the walls of the arteries to dilate.
Corpora Cavernosa versus Corpus Spongiosum: cavernosa maintains rigidity + hardness during vasocongestion while the spongiosum remains soft when filled with blood. The combination of the two is important as it keeps it so that the semen is able to leave the penis (without the sponge, it would be too hard and rigid)
How erect should a penis be? If standing upright with a full erection, the average angle is only about 10 degrees above horizontal, but this angle commonly ranges from 0 degrees to 40 degrees.
dartos. The dartos muscle responds to temperature and contracts if the testes are cold. This contraction causes the testes to rise, the scrotum to look smaller, and the skin of the scrotum to wrinkle.
Castration and Eunichs: They did not develop secondary sexual characteristics, such as a deep voice or facial hair, and they grew to be taller than noncastrated males. Because of their large size and high-pitched voices, they often had dramatic stage presence and voices. For this reason, eunuchs were a part of many European choirs, including the Vatican’s choir beginning around 1550.
- Prostate cancer patients use chemical castration as a method to aid in their treatment and extend their lives
The glans: the most sensitive part of the penis
Scrotum and testes: the scrotum is a loose pouch of skin that hangs under the base of the penis, it contains the testes.
- Seminiferous Tubules produces testosterone, immature sperm produced in seminiferous tubules travels to epididymous where they are stored and kept till mature
The vas deferens: it carries sperm to the prostate to enter the urethra. Sperm moves through contractions, sperm can not swim
The seminal Vesicles: two tubular glands next to the prostate near the ends of the vas deferens contribute a sugary liquid that makes up 70% of secretion liquid (alkaline)
The prostate gland: lies below the bladder; and secretes a thin, milky, alkaline fluid that results in a liquid that is a safe environment for sperm. It counteracts the harmful acidic environment of the urethra and vagina; it surrounds the urethra
The Copwers gland consists of small pea-sized structures on each side of the urethra that secrete pre-cum. This precum may contain active and healthy sperm. – the small alkaline liquid…
Cremaster muscle: contracts/causes the testes to contract to maintain sperm health + maintains a good temperature for sperm
Prostate cancer: If the cancer is caught early and is still localized within the prostate gland, it can be treated in various ways—for example, through radiation therapy or surgical prostatectomy. But if it has spread to other parts of the body, curative treatments are no longer an option. Instead, it is treated first with androgen deprivation therapy and then with various chemotherapeutic agents.
Semen is made up mostly of fluid from the seminal vesicles and the prostate gland.
The vas deferens and the ducts from the seminal vesicles share a common ejaculatory duct into the urethra. This means the vas and the seminal vesicles secrete their products together into the prostatic portion of the urethra.
- the seminal vesicles and the prostate gland produce proteins with opposing functions
Order of semen: seminiferous tubules, epididymis, vas deferens, urethra
Baculuum: penis bone (these do not exist)
Testes are analogous to ovaries
Skenes gland is analogous to the prostate
The process whereby sperm loses its outer plasma membrane to enable possible binding with an ovum is called capacitation
There are age related decreases in sexual response !!! less lubrication, longer time for arousal; types of stimulation and needs vary between sex and between age
Several studies have indicated that men and women—regardless of sexual orientation—show a similar pattern of activation in cortical and subcortical areas in response to sexual stimuli, sexual arousal, and orgasm in fMRI studies
Chapter 10 - GENDERSEX
__________________________________________________________
Sexual configurations theory***
Biological sex is described as the biological traits that are related to maleness or femaleness through genes (xy,xx,x,xxy…), hormones (testosterone), and physiology (phenotype/the physical experience, the development of the genitals, breast development, shoulder to hip, waist to hip ratio)
Gender is a psychological experience of femaleness or maleness; it can emerge from biological factors and sociocultural factors, there may be an alignment and there may not be. Gender is not a fixed thing, it varies and is malleable by sociocultural context and culture. Expression can differ based on sociocultural aspects.
Gendersex: they likely influence each other in bidirectional ways making it hard to separate how individuals identify and describe their sex; for the vast majority of phenomena, it is hard to detangle
Development of sex and gender: Fetuses (genotypes) can develop into either phenotype. Gonads are undifferentiated and become differentiated through the X & Y chromosomes.
Chromosomal sex: XY and XX
Gonadal sex: the type of gonads
SRY gene: usually present in XY embryos only, it is linked to the Y chromosome, when this gene is present, there is the testis-determining gene; Depending on the presence or absence of a gene, the sry gene activates testosterone and prevents the development of the female-typical phenotype
- The presence of testosterone boosts the development
- The SRY inhibits the default
- The female body does not require the presence of any additional hormones.
Gender binary in cisnormative research and their harm: there was a lot of belief in research that gender is dichotomous and two-variables; there was a lot of belief that it was biologically determined and stable over time which is not true. Gender binaries silence gender-diverse people, pathologize variation, and contribute to invisibility in science
- If you do not ask the correct questions, you are not going to be able to lead to proper conclusions that accurately reflect people's experiences
- Gender binaries lead to problematic beliefs that misrepresent the variability in human gender/sex
Sexual Configurations Theory: it captures the wholeness of people’s actual experience of gender/sex and sexuality, Sari uses queer and feminist theory to account for the full and whole range of gender and sexual diversity. She felt as though these understandings of gender, sexuality, and gender sex were very limited and waited to encapsulate room for sexual expression now and all sexual expression over time.
- The sexual configurations theory makes room for other aspects of sexuality by de-centering ideas of gender/sex – partner number, activity preference, etc.
What we see as gender/sex is capable of influencing an individual’s behavior and attitudes
- Attractiveness as seen through social media
- Dating scene
- Our understanding of what is ok for a particular gender sex/ if something does not fit into a specific schema
Gender role theory
Gender role schema
RESEARCH STUDY RESULTS: meta-analysis on gender differences in sexuality: the gender similarities hypothesis. 1st meta-analysis: looked at gender differences and sexual attitudes while looking at the size of gender-sex differences. Follow-up meta-analysis (2): of these 30 behaviors originally tested, how have they shifted over time as our society influences how gender is expressed → are gender differences getting bigger over time???
Findings: we are seeing intercourse frequency in men where men have more intercourse than women (d=0.16), men report greater interest in casual sex than women (d= 0.38), men more than women are reporting more masturbation (d=0.53), use of erotica is more used by men than women (d=0.68), women reported having more same gender sex experience (d=0.05, no effect), interest in sex with commitment was reported more by women ( d=0.18)
Overall there were no extremely large differences!!! – the degree to which men and women differ is actually way more similar than it is different.
- Effect sizes in meta-analysis: it is not rare that we find a significant difference (p<0.05) but is that difference characterized by differences???
- Cohens d: how different, is the amount of standard deviations between two means significant, how much overlap is there?
Large effect size: d=0.80 is considered a large effect, 0.2 is small, 0.5 is medium
Reporting bias and adherence to gender norms:
- The degree of difference may depend on shared expectations of people’s behaviors, People tend to be aware of gender norms; this awareness is capable of influencing the reporting of attitudes and behaviors usually in the direction of adhering to the gender norm
Among Cishet men and women – presumably having sex with each other, men report having more sexual partners than women.
- Using something called a bogus pipeline group (Fisher), where individuals are brought to a lab and hooked to a “lie detector” called the bogus pipeline – using these paradigms helps limit the gender-reported differences. Normally, men report fewer if they thought they were being recorded for lying; women would report higher…but when utilizing the bogus pipeline condition, this effect becomes narrower
- Reporting bias does influence men and women in their reporting behaviors
2 gender/sexual differences that are large in magnitude and have to do with patterns of genital arousal: Sexual concordance, Specifity of genital response
- Sexual concordance: the level of agreement between mind and body connection
- Sexual concordance in mind and body connection across various measurements: men on average have a relatively stronger concordance between mind-body connection (d=.66), cis women have lower (d= .26), transwomen have a stronger mind-body connection (d=.67) → gender sex and sex → aspects of their own experience and understandings of gender norm can influence their experience within a norm.
- Experiences can be in part biological, however, their understanding of their own gender can also impact their identity
- Specificity of genital response: what kind of factors influence genital response??
Chivers:
CISHET Men’s genital arousal is category-specific– men only show a genital response to things that they say they’re interested in.
- If straight men report being attracted to women, they will show the strongest response to stimuli that depict women.
- If gay men report being attracted to men, this will also match their response to stimuli
- Men and transwomen respond to stimuli that match their sexual preferences
Cisgender women’s genital arousal is category-nonspecific
- Regardless of the gender sex, women show very very similar responses for consent / non-consent and show responses to sexual activity cues (men and men, women and men, women and women).
- If women report any degree of attraction to women, they show similar levels of category non-specificity but more of women.
THIS IS THE LARGEST DIFFERENCE between gender sex that is recorded in research
- Perhaps this means that the sexual arousal system between women and men is different.
Diversities of sexual development is a group of congenital conditions that differ from what is expected which can capture the variability in the phenotype (an intermediate expression of the male and female phenotypes) with the inclusion of the intersex identity.
- How do these affect behaviour, sex, sexual orientation/attration, sexual function, appearance etc.
Hormone variations: androgen insensitivity syndrome, congenital adrenal hyperplasia
- Androgren insensitivity syndrome: when a body is insensitive to testosterone so you develop a female phenotype
- Congenital adrenal hyperplasia: more common where a baby is exposed to high levels of androgens in utero which can affect XX and XY fetuses differently
- 1 in 5000 to 15000
- XX fetus: enlarged clitoris, fused labia, shallow vagina, internal reproductive organs are intact
- XY fetus: genital experience is typically unaffected.
- Gender expression: children with CAH may express behavior and interests that differ from their same age/gender peers where XX may show less nurturing and more aggressive behavior, while XY may show less aggressive and more nurturing behaviors
- XX may have compromised sexual functions like pain and desire
- 1 in 5000 to 15000
Chromosomal variations: klinefelters syndrome (XXY),
- Klinefelter syndrome (XXY): 1 in 500 to 1000 males and usually diagnosed during puberty
- HPG axis influences our hormones (feedback loop between brain and gonads that regulates hormones); LOWER T and higher levels of FSH
- Individuals with this condition will change the phenotype IN PUBERTY where there will be breast development, small testes, shorter than average penises, low T, and compromised fertility.
- Can be treated with testosterone
- Individuals with this condition will change the phenotype IN PUBERTY where there will be breast development, small testes, shorter than average penises, low T, and compromised fertility.
- Sexuality and gender: individuals may have low desire, they report being attracted to women (however many dont report identifying as men/male)
- HPG axis influences our hormones (feedback loop between brain and gonads that regulates hormones); LOWER T and higher levels of FSH
- Turners (XO): missing x chromosome
- Shorter stature, broader chest
- Higher infertility
- Underdeveloped breasts
- Most identify as female or intersex
- 5 alpha reductase deficiency - 5ard : mutation that makes one have both male and female reproductive organs; male reproductive organs will descend during puberty
Gender development has three related processes: detecting, having, and doing
- Detecting gender: can you see a physiological difference? What is male/female-typical?? Emerges by age 1
- Having gender: the recognition of one's characteristics/ what you share with either girls or boys. Emerges by ages 2-3
- Doing gender: matching one’s behavior with male and female stereotypes. Happens typically by ages 5-7 (friendships, playmate preferences, etc)
Gender variation is the norm, not the expectation. It can occur in childhood to varying degrees. These could be associated with sexual attraction, sexual identity, adolescence, and adulthood (IT DOES NOT PUT YOU ON THE DEFINITIVE ROUTE FOR being gay, lesbian, trans, etc, however, it does for some folks). Can also occur within culture; non-Western cultures are much more tolerant of accepting variation within gender. Gender dysphoria does not exist the way it does in the West. Lastly, can exist within best practice – should gender-affirming intervention occur and when? We know through longitudinal research that children with stronger cross-gender identification and preferences are more likely to social transition with respect to whatever gendersex they want to transition to and would benefit from puberty blockers and hormonal treatments.
Gender variation can exist within:
- Childhood – behaviors in youth can be associated with future expressions/identities
- Culture – there is a lot more tolerance in the accepting of variation in gender. (gender dysphoria is a Western thing!!!!!)
- Best practice – when gender-affirming intervention should if it should occur at all.
Trans identities – there is a lot of variation in how people experience their gendersex, following the sexual configuration theory, this variability (in strength, what is normative in cultural norms, etc.) may influence a person’s decision to seek gender-affirming care.
- Every person engages in gender-affirming activites→ going to the gym, breast augmentation as a woman to feel more feminine, etc.
An individual's status is where they identify at a given moment, this status may or may not align with their broad identity.
Research study: understanding gender euphoria more as it is linked to a person's gendersex – what does it mean, and how is it experienced? Findings: gender euphoria is a feeling of rightness in an individual’s gendersex; can be internal, external, or social (experience of putting on a dress as a cis woman); it originates and circulates in online and in-person gendersex minority communities (perhaps it is not acceptable to adopt the term: gender euphoria, when you are in a majority group // electric feeling of happiness: expressing one’s gender as a nonbinary person in a situation in which it is marginalized and ostracized); dysphoria describes the negative feeling of conflict between gendersex aspects of self; the relationship between gender euphoria and gender dysphoria is complex (contingent on how others interact with you, extends outside of yourself).
- Why is there social stigma directed to some individuals but not others when all of us participate in this behavior to some extent?
- Dysphoria is quite a Western understanding however with colonization, there have been shifts that have spread the concept of gender dysphoria and the gender binary
Examples of gender-affirming practices
- pharm/surgery interventions
- Hormone therapy
- clothing/binder access
- therapy/counseling
There are no neat boxes, everyone's experience of gendersex is valid
Variation is the norm!!!!!!
Chapter 11 - SEXUAL ORIENTATION
__________________________________________________________
Orientation is a compass that points in the direction(s) of attraction and attachment → sexual orientation and affectional orientation, we use it as a bit of a guide
- Eroticism vs nurturance
Sexual orientation is limited: sexual orientation overemphasizes the sexual component and is usually categorized by the gender binary; it describes the interaction of “your gendersex + the gendersex of the person you find sexually attractive”
- We know that identities change so much, sexual and affectional orientation shift
- What if you're a straight woman dating a man and they come out as a trans woman, what happens to your identity?
The number of difference axes → your gendersex, the gendersex of others, what are you attracted to? (cues of masculinity, voice, etc – maybe it is not gender?), age, partner number, type of sexual activity (kinks)
Orientation – who do you think about, who are attracted to, behavior is not a good proxy. Gendersex: male/female-oriented, bisexual; partner number: non-sexual, multisexual
Status– what are you at this given moment? Not being sexually active despite having a sexual orientation…
Sexual orientation is not always sexual!!!
Affectional orientation: eroticism + nurturance ( attachment, loving, close feelings)
- SCT is comprised of two domains: partnered sexuality and solitary sexuality
- Partnered sexuality has 3 domains (eroticism & nurturance are built-in)
- Partnered sexuality is connected to identites (eg. lesbian, straight, pan, gay, poly) → identities are given to some configurations)
- Other sexual parameters may play a role as well (kinks)
- Partnered sexuality is connected to identites (eg. lesbian, straight, pan, gay, poly) → identities are given to some configurations)
- Partnered sexuality has 3 domains (eroticism & nurturance are built-in)
Gendersex Sexuality: A bisexual poly individual may experience erotic orientation to men/masculine cues while experiencing nurturant orientation to women/femininity – may choose to have sex with men while partnering with women
Partner number sexuality: erotic AND nurturant connections with multiple people
Sexual parameters: BDSM
Is sexual/affectional orientation stable over time?
Identity labels: can and do change over time OFTEN, these labels have personal significance to the individual, partner identity can change your own identity
Eroticism: ALSO CHANGES/is fluid, sexual interests can change over time however this is predominant among people with non-exclusive sexual attractions, there is variability in the strength of erotic attraction day-to-day
Nurturance: much less research is focused on this affectional aspect, though there is reason to believe that this could change over time consistent with SCT
Among sexual minority women, there is a lot of variation in attraction and eroticism!!
- LOTS OF FLUIDITY
- We typically see the most fluidity amongst individuals who report non-exclusive sexual attraction (those who were on polar ends of the Kinsey scale (only one or the other reported much less), even if you report a very small interest, you are still non-exclusive, and that is where the majority of the shift is reported.
Data from a large US study of young adults and sexual orientation identity:
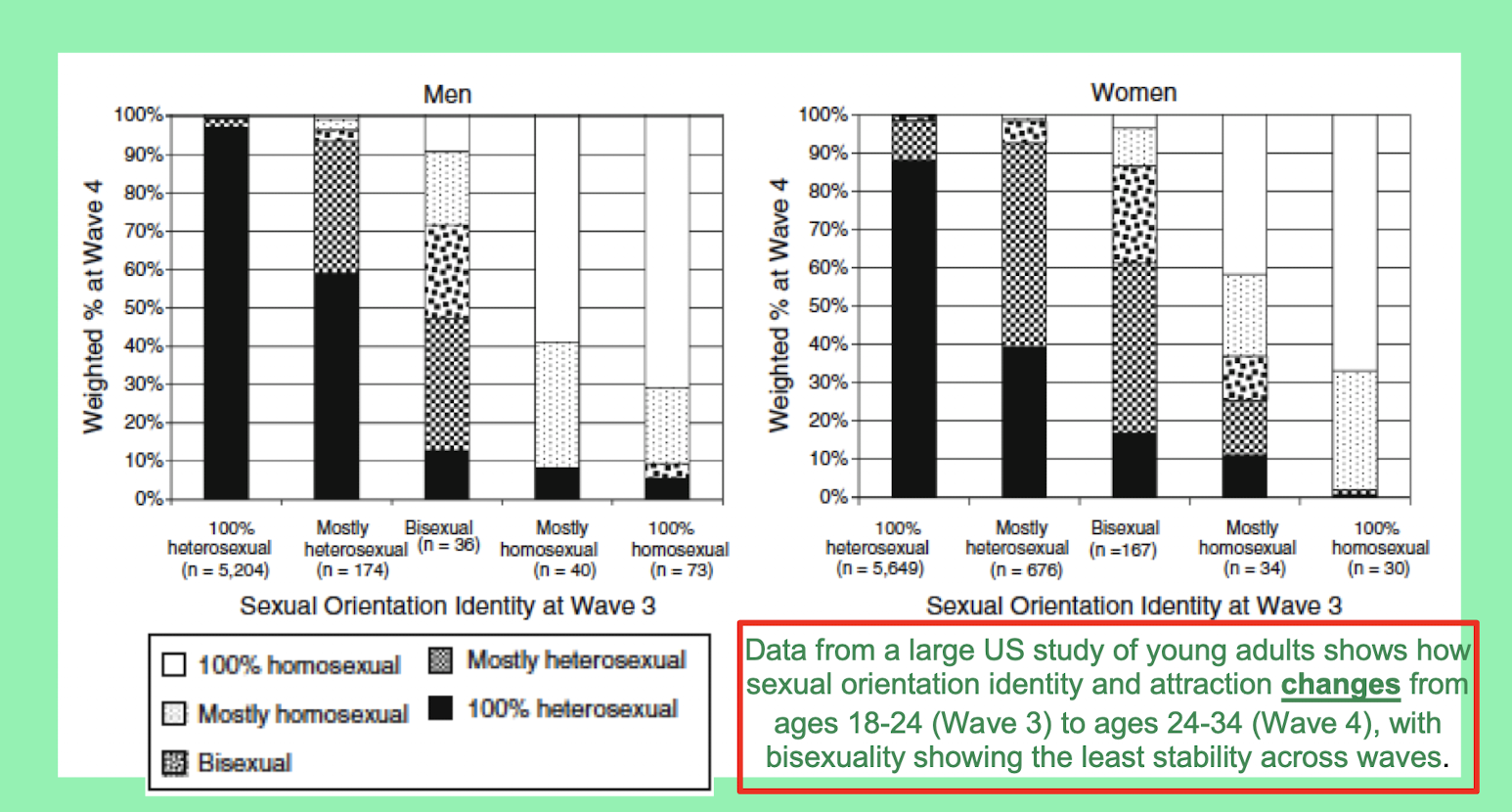
-of the men who reported that they were heterosexual at wave 3, 98% at wave 4 reported that they were still heterosexual, and those who were homosexual reported mostly being homosexual as well
- paying attention to the middle area: individuals who identified as bisexuals in the middle area in wave 3 experienced large shifts in wave 4 → All 5 sexual orientation identities are endorsed
- Fluidity is not specific to women
- The largest variation shifts in those who were non-exclusive
How do sexual and affectional theories develop? – no one theory can support all.
Failure of psychosocial theories (least empirical evidence)
- Psychodynamic perspective: there is no evidence that gay men had hostile fathers or overprotective mothers; there is too much relation to parents which just isn't true; homosexuality is not due to an aversion to women or due to wanting to fill in void for bad fathers
- Social learning perspective (1980s~): suggested that people learn through different social interactions and experiences to have a specific sexual orientation; there was an idea that early experiences with specific people, that the reward from that may condition/make you develop towards having a specific orientation – WE KNOW: many people have sexual debuts and experiences with people of the same gender sex however they arent more likely to go on to be gay; behaviour =/= orientation; it is actually difficult to condition sexual preferences based on gendersex – YOU CANNOT REALLY CONDITION ORIENTATION
- Socialization: gay people/being raised diffeerently from hetereosexual pairs may influence their development – no evidence
BIOLOGICAL THEORIES – can be harmful but there is evidence that it is not a choice
- Prevalence rate is quite consistent - when something is consistent even though it is low, it suggests that there is a biological/genetic basis ;
- we see much higher matches in identical twins
- Fboe Fraternal birth order effect : the presence of each older brothers increases chances of a younger brothers odds of being gay by 47% : Brain development that happens in utero: mothers can have reactions to androgens; antibodies that mothers are used to can change after carrying xy babies, there can be shifts in brains, etc. HIGHER IMMUNE RESPONSE
We cannot pick who we are erotically or nurturant interested in
Reparative therapy: is it possible to change sexual orientation
- We realized through findings that many individuals who reported differents were masking or were able to stop engaging in behaviors however actual orientation and attraction did not change
- REPARATIVE THERAPY is not effective in changing sexual orientation
- It is harmful and is considered a human rights offense AND NOT EFFECTIVE
Minority stress theory: Brooks was a lesbian woman who was the first ever to publish work on lesbian women and stress; it has LOTS of empirical support: THERE ARE LOTS OF STRESSORS THAT impact an individual, depending on the context, you experience stigma and stress differently and this has effects on minority stress and health
- These stressors particularly embody microaggressions that communicate negative messages about identity or group membership
- Microaggressions: HIGHLY PREVALENT and most likely, linked to poorer academic performance, and higher stress, more health difficulties
\
Microaggressions:
- Microinvalidations: invalidating a lived experience: not being homophobic bec you have a lesbian or gay friend
- Microinsults (more overt): act less gay, gay as an identity, its a sin, direct communication that something is not ok, i wouldve never known…
Sexual debut
Research results for how undergraduate students define having sex: for the vast majority of individuals, penetrative sexual activities were identified as “sex” (penile-vaginal/penile-anal), oral sex, masturbation, kissing body parts, bathing/showering were not as endorsed– probably involves genitals, probably involves yourself and others.
What does it mean to have sex– 1) There is lots of variability, orgasm is a possibility
- Variability: typically sex is defined as mutual genital contact AND orgasm (these definitions apply to individuals of all gender, sexual, and affectional orientations), lesbians show greater flexibility in their definitions
- This is important as there is often a script/step-wise pattern for what one should expect – understanding lifespan’s influence and flexibility that comes with script changes.
- Having a flexible definition of sex (sexual script flexibility) allows individuals to stay positive about their sex life
- FLEXIBILITY IS GOOD!!!
Why should we care about definitions of sex?: how individuals define and understand sex can influence how healthcare individuals question sexual status, make decisions about contraception, respond to your sexual information (condom use), make decisions about health conditions (cervix cancer)
- How an individual communicates about what sex means has implications for their access to care
What are some general trends in people’s “first times”?
- A wide range is typical both before and after – how did our expectations line up with what we expected of the situation, who the person was? What did you do?
- 71% of men and 61% of women thought that their sexual debut was good, v good, perfect
- 11% of men and 13% of women thought it was bad, very bad
- Men reported more pleasure than women did → 62% of men and 6% of women recalled having an orgasm; ORGASM GAP STARTS EARLY
Recollection of sex can impact how we feel about sexual debuts → If you had sex at age 16/17 and everyone at school knew, your gender sex could impact your debut as certain expectations may be placed on girls and guys respectively (eg. girls are seen as sluts; guys are seen as ‘the man’)
Recent research from UofT:
Women who debut with men → less orgasm, less pleasure
Women with women → higher rates of orgasm and pleasure
- Perhaps anatomically the increased familiarity assists in making an experience better
- Between women, it is not orgasm driven, when there is no penis there could be more focus on pleasure
Factors that influence age at sexual debut: Later vs Earlier Age
Later Age: parental disapproval of early sex and contraception, higher parental control (greater involvement of parents in everyday life – more empowered), higher self-esteem, higher religiosity, higher academic achievement (busy, ambitions are elsewhere)
Earlier Age: earlier puberty (more hormones = greater interest, seeking out more opportunities), greater peer pressure, substance use with peers, having an older partner, early dating, lower SES/family distribution
In grade 9 – 19-23% of students have had PVI
In grade 11 – 40-46% of students have had PVI sex
- This data is important as it is used to inform health policies and intervention strategies about STI awareness, barrier awareness, giving individuals access to contraception, helping them prevent unintended pregnancies, and sexual coercion → SEXUAL CONSENT IS KEY!!!!
- Understanding who is having sex and when is important for informing public health policies + helping them implement needed services
Research study: Population based study about sexual debut and later outcomes; what are the links between age of sexual debut and later outcomes? Findings: Greater number of lifetime, recent, concurrent partners is associated with increased risk of sti (hpv)/cervical cancer; more variation in sexual experience – more exploration; more pregnancies in adolescence; greater length of time between sexual debut and marriage (increased rates of cohabitation); there is mixed findings for sexual difficulties
Consent:
Research Study: Does more sex make you feel better? Sexual frequency predicts greater well-being but more is not always better. Findings: sex correlates with well being however not when sex is done more than once a week and in relationships. Folks that are having sex once a month have the least reported satisfaction in life; ONCE A WEEK APPEARS TO BE THE SWEET SPOT – you hit a plateau, there is no measurable benefit
What are the three key components of sexual consent
- The person has to have a clear understanding of what they are consenting to
- Consent must be given freely and not coerced
- Consent should be ongoing and can be withdrawn at any point – can be withdrawn not only between actions but also between days/sessions too – just cause something is done once doesnt mean it can be done every time.
** verbal affirmative consent is the gold standard
Research Study: What kind of setting/relationship context makes it so that verbal consent is more apparent vs not → public? Not? Certain type of sex? Situationship? + role of gender/gender norms. Findings: consent varies depending on context – Explicit verbal consent is less likely if person is a woman, sexual relationship is casual, and when behaviour is something other than PVI (things like oral sex are less likely to have verbal consent)
Sexual compliance: when a person freely consents to engage in sexual activity even when they truly do not want to participate (happens in long term relationships often) → pressure to participate even though they do not necessarily want to.
- When might you be likely it be sexually compliant – theyre upset, havent done it in a while
- What are your reasons/motives to have sex with your partner – make them feel better, prove you love them
Sex to pursue a positive outcome has an important role: 2 outcomes: approach motives & avoidance motives
Approach motive: increasing intimacy/ feeling emotionally close/ making another happy/ leading to a more positive outcome for partner, you, the relationship
- Individuals that engage in approach motives = associated with greater sexual and relational satisfaction
Avoidance motive: sex to avoid conflict/negative outcome, to not disappoint someone,
- Individuals who engage in avoidance motives = linked with lower sexual and relational satisfaction
** its better to not have sex at all than to have sex for avoidance motives (if you only have sex for avoidance motives)
Types of sexual relationships
Sexual satisfaction: the overall appraisal of one’s sexual life; it plays an integral role in quality of life, mental and physical health – 50% of individuals in long term relationships report relatively high levels of sexual satisfaction even during large shifting/change periods ( like postpartum)
Interpersonal exchange model of sexual satisfaction is all about the costs and rewards associated with sexual interactions and behaviours with one’s partners = viewing this kind of intimacy as an exchange.
- How relationally satisfied (relationship satisfaction) plays a large part in sexual satisfaction
- Relative level of rewards to costs
- Comparison level of rewards to costs
- Equality of rewards and costs
- Main takeaway for cost/reward: we feel most sexually satisfied when the rewards are greater than the costs!!!!
Research study: how people’s profiles and the ways in which they interact and engage online influence dating success/ whether or not those profiles and interactions lead to long-term dating intentions; compliment given vs humor + altered attractiveness levels. Findings: whether or not you found a person hot or not + positive attributes that you are associating to the profile (eg kindness) influenced whether or not people would choose a person for long term vs short term. We associate positive things based off if we find someone attractive
- For women: using humor and being kind has significant effects on long and short term dating intentions
- For men: it doesnt matter what you open with, it is only what you look like
- Overall: perceived attraction + positive attributes predict long and shortterm dating intention
We are seeing a shift in which a rate of marriage is going down; number of cohabiting couples is rising, canadians also remain single for longer (potentially due to pursuit of higher education)
Sexual satisfaction in committed relationships may fluctuate: factors that may influence this are childbirth, stress, hormonal shifts + the frequency of sex may decline. Researchers find that despite decline of sex, there is a maintained satisfaction for couples who are relationally satisfied – couples who are relationally satisfied tend to stay sexually satisfied even if they have sex less.
Friends with Benefits: FWBR
- Characterized by 4 components:
- Ongoing
- Sexual
- Requires no sexual or emotional exclusivity
- Relationship is rarely discussed or directly revealed to others
Consensual non-monogamy (CNM)
- Vary depending on people however it involves partners who have romantic or sexual relationships in addition to sex
- Include polyamory (long term romantic + sexual relationship with 1+ person at the same time; motivated by nurturant component), swinging (both partners are in a committed relationship agree to have sex w the same people at the same time; more erotic), open relationships (usually where both partners consent to sex but not emotional bonds with others; you could have multiple partners who are long-term however the nurturant relationship is focused on the primary), and other
- Nonconsensual non-monogamy - any kind of emotional or physical connection with a person outside of a monogamous relationship without the agreement of one’s partner
- About 3-7 % report currently being in a CNM relationship
Unique and Shared benefits of CNM relationships + Monogamous relationships
CNM only:
- need fulfillment - being able to engage + fill a need for fulfillment
- Activity variety (non-sensual) - being able to engage in activities that you enjoy w a partner that perhaps only one wouldnt be able to offer (eg. you have a partner who is a runner)
- Personal growth/expansion - can expand world view + personal growth
CNM and monogamous:
- family/community benefits
- Trust
- Sex + love
- Differing levels of commitment
- communication
Chapter 15 - PARAPHILIA and SEXUAL VARIATION
Paraphilic interests can be divided into two main categories: preferences for atypical targets and preferences for atypical targets
- Where would these paraphilias fit within the sexual configurations model?
What is atypicality?
- Variability could be defined through prevalence, what is legal, what does not cause harm, what is seen as a norm
Prevalence: doesn't judge - only accounts for now often something occurs.
norms: may not be great is they can be subjective— norms can change over time as norms are constantly shifting
Legality: sex between two men may be legal/illegal- what is viewed as legal in some places may not apply to legality globally.
Harm: there is a lot of subjectivity (whether it harms individuals viewing or partially in a behaviour does having a fetish cause harm?- there is no general consensus - the is a multifactorial approach - a deviation from average
What is Paraphilia? para = deviation; philia= love
Paraphilic interest can be described as an intense and persistent interest that is in something other than genital stimulation with physically mature, consenting, adults — can be exclusive or non-exclusive
- Paraphilic interests are more common
Paraphilic disorders are when an interest causes distress and impairment to the individual OR causes personal harm or risk of harm to others when acted upon
- these individuals would prefer not to have these interests
- Whether they act or do not act on these interests, it is capable of causing individual harm
- Pedophiles have a Paraphilic disorder but it possible that they never act on it
Paraphilic disorders related to different stages of courting— unsuspecting persons that are at risk for harm are impacted.
Voyeurism: one of the most common, it is the act of watching an UNSUSPECTING PERSON who is naked, disrobing, or having sex, with the potential of getting caught
- watching your partner undress is not a Paraphilic disorder
- watching porn is also not a Paraphilic disorder— as they have consented individuals to get turned out and aroused (not unsuspecting) (the people in porn cannot catch you watching)
- watching your neighbours having sex through a telescope IS a Paraphilic disorder
exhibitionism: intense arousal from exposing one’s genitals to an unsuspecting person
- scatalogia: is arousal by making sexually explicit phone calls and masturbating during or afterwards
- is streaking across a public event a Paraphilic disorder? — depends on if you are getting turned on, if you are looking for individuals watching you, depends on motivation, thrill; individuals who streak at sporting events typically are not classified as exhibitionism
- Masturbating on a phone call with your partner is not a Paraphilic disorder as no one would be unsuspecting
- Exposing your genitals to a person at a bus stop — would be a Paraphilic disorder, especially if you’re looking for shock
- Sending an unsolicited dick pic could be a Paraphilic disorder, esp if it is being sent to strangers, and if the reaction itself is sexual. however there is no consensus, it just illustrates how cyber sex and online spaces have shifted the ways in which paraphilias could present
Frotteurism: frotter=to rub; arousal from fantasizing about engaging in or rubbing against a non-consenting person; requires crowds and public transport
- grinding on a person on a bar dance floor would not be a Paraphilic disorder as it is somewhat expected, some consent in participating in the dance floor
- You cram into a bus of people and run up against someone until you reach organism — would be a Paraphilic disorder as it is explicitly sexual, you orgasm, the person is not mentioned to be suspecting of such an action, and it is interpreted as sexual when typically it is not.
Paraphilias related to atypical targets: could be Paraphilic disorders but could also be paraphilias that are part of their sexual menus
- Fetishes: persistent and repetitive use and dependence on non-living objects or a specific non genital body part for arousal, typically come in come in combinations and is necessary for arousal. - how intense or persistent something could be; fetishes could be feet but only if you cannot reach orgasm without it, enjoying the sensation of getting your feet sucked is not a fetish unless you need it to cross a specific line.
- Transvestism: cross dressing within a sexual context; arousal by cross dressing; NOT to be confused with a persons experience of their gender sex or gender affirming practices
- Pedophilia/hebephilia (disorder): sexual arousal and attraction to individuals below the age of puberty (pedophilia), or early stages of puberty (hebephilia)
Other Paraphilic interests
Urophilia- pee
Scatophilia- arousal to poo
Biastopohilia- arousal to non consent
Zoophilia- arousal to animals
Somnophilia- sex with someone who is asleep or unconscious
In terms of gender diversity and paraphilias— paraphilias are more common with men over women.
research study findings: why do we see more Paraphilic interests (not disorders) in men rather than women? Is there a gender sex difference? Neurodevelopment were considered, perhaps there is a common causal mechanism in developing psychopathology and paraphilias; if men are 3 times more likely to be affected by prenatal environments, are they more likely to develop paraphilias cause of this. Is sex drive why we see more of a gendersex difference in the literature surrounding paraphilias? What about impulsivity and low inhibition/risk-taking? Maybe differences in how we seek new sensations influences how one experiences paraphilias? What about masculinity — manifestations of masculinity that are associated with either masculinity or femininity? Is it based on exaggerated gender roles? What about the sexual double standard — women don’t report honestly?
- TOTAL PARAPHILIC INTERESTS SCORE: m> w (d=0.4), men report greater interest (medium sized) difference in Paraphilic interest compared to women
- For ALL paraphilias, especially voyeurism, urophilia, hebephilia, biastophilia, fetishiism, men reported more
- No difference: masochism (d=.008), transvestism fetishism (d=.08)
Utilization of multiple mediation ( don’t need to know what it is) to explain and account for gendersex differences — do any of these things make it so that gendersex differences disappear
- only one factor ameliorated/eradicated gendersex difference and that was sex drive
- Gendersex difference factors men more so than women
- eg. Prostate cancer/ chemical castration patients could experience different sex drive vs testosterone, how one responds to cues, it could have an effect but there is no research on it yet
Findings: yes there is a difference, however differences explain gendersex difference
- people who have low sex drive may have limited sexual energy towards preferred people (smaller sexual menu)
- People who have high drive may choose to expend vast energy more towards preferred targets and behaviours; maybe they habituate more quickly to specific activity + enjoyment of switching it up, more novelty + also about having lower aversion levels
- Maybe it is about possibility of expenditure
- Sex drive may have a more generalized effect on arousal, fantasies, etc. which could influence comorbidity
- Sex drive is also possibly explanatory to higher sexual violations
Follow up research study: what explained the interest to behaviour seen through Paraphilic interests and behaviours; findings: more interest in links between Paraphilic interests means you will be more likely to pursue it in some way— sex drive impacts engagement. LINK BETWEEN HAVING PARAPHILIC INTEREST AND ENGAGING IN THE ASSOCIATED BEHAVIOUR IS STRONGER AT HIGHER KEVELS OF SEX DRIVE — figuring out treatments for sex drives (we cannot change people’s sexual interests) specifically targeting sex drive, could be a potential target to counter people sexually offending
Pedophilic disorder: individuals often suffer from cognitive distortions- Cognitive distortions are often statements that individuals make to themselves that serve as excuses to allow them to rationalize, justify, minimize, or deny that they are behaving in an inappropriate manner.
SEX DRIVE EXPLAIN gendersex difference, for explaining link between interest and how one pursues it
Guest Lecturer: Cara Dunkley
BSDM
Fetishism is included in BDSM umbrella
Scene= engagement in bdsm play
d/s → power exchange, it is an exchange of power and control
Less to most intense
top/sadist → bottom/masochist
Dominant → submissive
mistress/master → pet/slave
The power dynamic of switches can shift throughout the scene, however, they tend to shift depending on partners; could also be position dependent
There is a distinction between hurt (physical or emotional) and harm
BDSM pain is defined as QUALITATIVELY different
Pain– can alter subspaces → Pain could be desired for a variation of motivations → could help individuals let go of the burden of “self-hood”
Association between bdsm preference and everyday lifestyle → There can be a link but it is not in a predictable uniform way
- A person who has no control in their personal life may enjoy dominating in BDSM as a way to get a sense of control
- Another person who has absolute control over every aspect of their life may also happen to enjoy dominance in that arena as well
- There are tropes but it depends on the person.
Both DS and SM can be enjoyed without sex !!!!!!
- Sexual activity can happen however bdsm events can take place, there can be pick ups or activities done with friends who are also into BDSM
Prevalence: how common is bdsm and how common is interest??
- approx 45-60% of people report having fantasies that have something to do with BDSM
- 30% of people have fantasized about being involved in some sort of pain play/ impact play (refers to the practice of being struck)
- 10% have reported engaging in BDSM at some point
- 1-2% hold an identity that is very centered on BDSM
These are very conservative estimates !!! there is some variability
There are many reasons why individuals may be into bdsm
- Common reports: individuals have always been kinky (enjoying playing games involving being tied up in childhood)
- Kink could potentially be biological and have some sort of inheritable relation however there is a lot of varied discussion about this.
There are reports that fetishes tend to happen through classical conditioning and childhood impactful experiences → sexually rewarding in childhood tends to be conditioned into fetishes later on.
Those who partake in BDSM have corresponding rates of anxiety and mood disorders; BDSM practitioners are no more likely to have a history of sexual abuse or assault than an average person
- Same rates of mental illness, sexual distress, sexual adjustment
- BDSM practioners are just as well socially adjusted
- BDSM can be helpful with sexual trauma
BDSM practitioners tend to be high in conscientiousness, less agreeable, more open, less neurotic, more extroverted
BDSM may be best regarded a recreational or leisure activity rather than other previous labels
Aftercare → begins when scene ends, afterplay ties to limbic system and prefrontal cortex activity.
- Needs of bottom > top, unless top has trauma history
- Need for aftercare is easier to see for tops, however it can be needed for top
- Perhaps need for reassurance is part of aftercare as well
Age matters less, more focus is on how long one has been playing → they will enter a scene as a submissive, they will try topping and get more into domming, more as a switch, shifts occur this way.
Chapter 13- Communication
Want an effect to generally match - not laughing while talking about something very sad - effective communication
- We dont want disaccordance with our emotion as it can lead to miscommunication and confusion
Relationship communication:
Amongst couples that are already having problems – there are longitudinal studies that based on the four horsemen can predict with 90%+ accuracy who will get a divorce
Gottman- Four horsemen:
1. Criticism
2. Contempt - extra criticism – sneering, mocking, insulting someone's character
3. Defensiveness
4. Stonewalling
Perceived partner responsiveness:
- Even though couples can be brought in and their values and behaviors can be reported on, what matters most (and what is the number 1 factor that predicts relationship satisfaction) is: do you perceive your partner to be responsive to your communication? (regardless of what others perceive)
- Greater relationship and sexual satisfaction – this causes the difference between how you perceive a relationship and how others perceive it
- Response =/= reacting
- Partner doesnt see, value or hear you = low ppr (perceived partner responsiveness)
- High ppr (perceived partner responsiveness) = better relationship longevity
In the context of relationships, sexual consent tends to be non-verbal
- a look
- These non-verbal approaches can be less intensive and can lower pressure
- Quality of non-verbal communication is a higher predictor of relationship satisfaction than verbal communication
Communication during sex:
1. Brainstorm before - what are your sexual likes and dislikes? buffet
2. Talk right before (context) - what do you want this time? You dont eat the same thing at a restaurant every time
3. During sexual activity (checking in + verbal and non-verbal consent)
4. After sex (what could have been done differently)
Mutualistic sexual talk - other focused
- Method of communicating the sexual talk that is related to sharing sex with your partner
- Exclamations: yes, ahh
- Positive feedback: that feels amazing
- Instructions: more, go slower
- Intimacy: i feel so close to you right now
Individualistic sexual talk - self-focused
- Relates to one's own experience
- Dominant - show me your, give it to me
- Submissive - I'm all yours, do what you want
- Ownership - you’re mine, whose __ is this
- Fantasies - let's pretend…, ive always wanted to
Study results: when one partner contributes to dirty talk and the other does not (when this is desired in the relationship)/when there is unequal sexual talk in a relationship, there are increased levels of sexual distress
- Findings: having a partner that is unresponsive to sexual talk is associated with higher sexual distress and lower sexual well-being
Responsiveness could be tied to sexual complacency – perhaps they are using avoidant purposes, perhaps it has to do with cognitive distractions
- Cognitive distractions play a big part in unsatisfying sex
- Motivations between partners could be different
- Mismatches in how you communicate
- Sex guilt can change how you respond
When people talk about sex, it is good for their sexual satisfaction, communication serves as protection against lower sexual well-being – those who communicate are better
How to reject sexual advancements – related to compliance
- Study findings: there are better and worse ways to reject sexual advances
- Perceived partner responsiveness matters – if a response is warm. understanding and welcoming,
Best way to reject sexual advances: reassuring rejection!!!
- Reassuring rejection is showing positive regard for your partner – coming from a place where you care for and are attracted to this person ( can be done non-verbal and verbal)
- Non-verbal → alternate forms of physical contact - cuddling + kissing
- Verbally → reassurance, adoration for partner + deferring to future.
- Associated with less distress and the best possible outcomes
Having sex for avoidance goals is associated with worse outcomes than just not having sex
Hostile rejection is the worst way to reject them → contempt, criticism
- Non-verbal → stone walling, dagger eyes for even trying to initiate, disgust, eye-rolls
- Verbally → “No get off me”
- criticism around how they are even initiating (but there is no communication on how they would prefer it)
- Those who engaged in more hostile rejections experienced more problems and a higher level of distress.
What are the associations how we communicate and the longevity of relationships?
- Reassurance is key → We want to listen, be receptive and open, and communicate this with non-verbal and verbal behaviors. We want to have high perceived partnership responsiveness
- We want concordance!!!
How do people communicate about sex before during and after – timeline of conversations
- Brainstorm before - what are your sexual likes and dislikes? buffet
- Talk right before (context) - what do you want this time? You dont eat the same thing at a restaurant every time
- During sexual activity (checking in + verbal and non-verbal consent)
- After sex (what could have been done differently)
What are the best ways to communicate around rejecting sex
- Reassurance rejection
- Non-verbal - redirecting to a different type of touch
- Verbal - reaffirming and reassigning a different activity or date
Chapter 16 - Dr. Katrina Bouchard
Sexual Dysfunctions – biopsychosocial model; assessment; treatment
Dynia: pain
Sexual difficulties are common
- It is not uncommon for 50%+ canadians to experience difficulties like low desire, orgasm difficulties, vaginal pain, erection problems, ejaculation problems
- This shifts with age; the older the population the more likely one is to experience these difficulties
- Sexual difficulties shift with blood flow → vascular system changes as we age and our blood flow becomes less robust through age
DSM5-5 Sexual dysfunctions
- Delayed ejaculation
- Erectile disorder
- Female orgasmic disorder
- Female sexual interest arousal disorder (FSIAD)
- Genito-pelvic pain/penetration disorder (GPPPD) → some people have a genetic disposition to this disorder
- Male hypoactive sexual desire order
- Premature (early) ejaculation
Area of desire on a linear model: Male hypoactive sexual desire disorder
Area of Excitement on a Linear Model: Erectile Disorder
Area of Resolution on a linear model: Delayed ejaculation + Early ejaculation
There is no perfect mapping for women:
Area of desire/arousal on a linear model: Female interest/arousal disorder
Area of excitement/plateau/orgasm on a linear model: Genito pelvic pain/penetration disorder
Area of orgasm on a linear model: Female Orgasmic Disorder
For women:
- There is less distinction among women; arousal and desire are thought of similarly
- How an individual perceives their desire matters – how spontaneous ?
- Variation exists however group level differences explain on merges that occur within disorders/states of arousal/orgasms during sex.
DSM-5 specifiers – how long and when it occurred
Categories for specifiers:
- generalized: not limited to certain types of stimulation, situations, or partners; happens in all contexts → eg. erectile dysfunction would occur in lots of ways whether it is masturbation, with all partners
- Situational: only occurs with certain types of stimulation, situations, and partners → eg. a person experiences no issues masturbating but experiences issues with a partner
___
- Lifelong: difficulty has been present since the individual became sexually active
- Acquired: difficulty began after a period of relatively intact sexual function
A biopsychosocial model is important when discussing sex
- Focusing on organic causes (or any one cause) misses the bigger picture !!!
Biological reasons for sexual dysfunction:
- Aging can cause changes in health
- Life stages can impact sexual function: Puberty/adolescence, pregnancy and postpartum, fertility, menopause
- Diseases impact vascular, neurological, and endocrine systems
- Damage to the central nervous system (MS, spinal cord, injuries)
- Hormonal problems like hypothyroidism, anemia, diabetes
- Prescription drugs are a common cause for sexual difficulties
- Medications used to treat cardiovascular health, arthritis, cholesterol
- Medication for psychiatric conditions also has sexual side effects
- Some hormonal contraceptives have adverse effects on arousal and desire
Psychological reasons for sexual dysfunction:
- Childhood sexual abuse and maltreatment – distal
- Attachment style → anxious-avoidant, insecure – distal
- Mental health concerns (depression/anxiety) – proximal
- Emotional regulation difficulties – proximal
- Life stress – proximal
- Performance anxiety – proximal
Social reasons for sexual dysfunctions:
- School-based sex education
- Family-based teachings (or lack of it)
- Religious teachings about sexuality
- Cultural sexual scripts
** HIGHLY cis/heteronormative
Psychosocial
- Sexual schemas:
- Shaped by the information and messaging we receive + our own experiences
- Childhood messaging that sex is bad, dirty
- Negative messaging about self-touch
- Sex-negative education
- Biological factors
- Still, take medication, there are options for better sexual well-being; there is therapy, broadening sexual repertoires, there are options that can be done
- Not all biological factors stand isolated
- Even hormones are influenced by other things
- There are multiple directions that one can put in efforts to influence.
Interpersonal activity → sexual activity often occurs in diads or triads+
Interpersonal reasons for sexual dysfunction:
- Low relationship satisfaction, low intimacy, relational distress
- Partner’s sexual function
- Partner’s response to the sexual concern
- Communication difficulties, problems with conflict resolution
Sexual stimulation is important
- Sexual technique can be an important contributor to sexual concern
- We do not want to over-pathologize something reasonable
- Note on couples *** When individuals are in relationships, one concern impacts others as well; when one person presents with sexual concern, the presence of sexual difficulties is a couple's issue
- You are not damaged !!!!
- Couple level approach, reduce pressure
- Note on couples *** When individuals are in relationships, one concern impacts others as well; when one person presents with sexual concern, the presence of sexual difficulties is a couple's issue
Case study: Naomi + Will (within the context of biopsychosocial + interpersonal model)
- Naomi had pain since the first time she had sex in her late teens
- Her and her partner Will have been married for 3 years
- Both want children
- Naomi → anxiety (ssri) and takes medication, takes birth control, uncomfortable talking about sex and genitals
- Cautioned not to masturbate by kind and religious parents
- Will had an open discussion with his parents about safe sex, and masturbation, but this conversation was awkward
- Parents not religious
- No sexual concerns in his history
Both are highly committed to their relationship; Naomi used to initiate sex → decreased frequency; will has stopped initiating for fear of rejection and not wanting to pressure naomi
- When they do have sex; the sexual repertoire focused on vaginal insertion, limited stimulation of the external genitals
- Stressed that Will is gonna leave her
Biological
- Naomi is on birth control and SRRIs
- Naomi is having pain since the beginning – what are some factors that could be related?
- Medication can affect sexual response
Social
- Sex negative messaging
- Catholic teachings? → what were these teachings in more detail?
- No family talk about sex
Psychological
- Anxiety disorder – highly comorbid with sexual dysfunction
- Discomfort talking about sex
- Fears about partner rejection
- Low self-esteem
Interpersonal
- Highly committed to the relationship
- No sexual difficulties
- Lack of sexual intiomacy
- Sexual avoidance
- Limited sexual menu
Just because there are sexual difficulties doesn't mean there are sexual dysfunctions
— nov 28
The specifiers for naomi’s GPPPD
- Generalized (hurts regardless of partnered/solo sex) and lifelong (has started since her first ever sexual experience)
Where does generalized and situational come in → for individuals with erectile dysfunction, many individuals experience difficulties during partnered sex but not solo sex
- Specifiers of generalized + situational are more created to describe what is going on
Specifiers for will’s erectile dysfunction
- Situational (doesn't apply to solo sex) + acquired (did not experience this initially in his relationship)
- Difficulty has to be going on for 6 months or more + distress must be present
Sexual dysfunctions are highly comorbid, however, there is a GIANT training gap in healthcare, especially when it comes to sexual health
- Data shows that how individuals feel about sex can dictate how they handle it in a clinical setting
- Doctors have also grown up with cultural sexual scripts→ if you have myths, then healthcare professionals are NOT trained to properly provide for patients
- Improving interview skills for discussing with patients is key**
Clinical interview for sexual dysfunctions:
- demographic information
- Presenting problems
- Personal distress
- How generalized? Is it situational
- Biopyschosocial factors that are at play – can be different depending on where individuals get their training + space they are surrounded by (ensuring youre not missing something that needs tobe treated biomedically if you are working as a sex therapist)
- Sexual technique
- Sexual response
- Partners response
- Treatments to date
- *it is important not to overpathologize when there has not been an opportunity for a desire to occur**
- “What do you do during a sexual encounter? What typically happens to test for this”
PLISSIT MODEL:
- provides a step by step approach in which anyone working has a path to talk about sexual health
P - obtaining permission to raise sexual issues
LI - providing LIMITED INFORMATION needed to support sexual function
SS - giving specific suggestions for individual to proceed with sexual activity
IT - providing intensive (higher level of care) therapy surrounding the issues of sexuality for the individual
** we want individuals to get responsive care**
Multidisciplinary Assessment
- Considering the biopsychosocial interpersonal factors → if they are referred to see a gynaecologist they see a gynaecologist first and then are possibly directed to other specialists!!!!
- Diagnostic for vulvar pain : cotton swab test that is pressed on to see if an individual experiences vulvar pain – is it an infection? Skin condition? Etc.
- The gynaecologist rules out potential factors, patient can then be referred to see a physiotherapist who assesses pelvic floor muscle assessments – diagnosing vulvodynia + treatment planning
- After physiotherapist + physio (helpful for general pain including for post-partum) + providing pain education, teaching PFM exercises
- Assessment of muscles is important as vulvar pain can be tied to tight muscles
- the patient may be directed to see a registered psychologist (states of higher anxiety can worsen pain – how an individual thinks of their pain has an influence on one’s health)
- Assessing sexual function
- Assessing reactions to pain
- Providing pain psychoeducation
How we react to pain matters !!!
There is a huge psychosocial component to sexual concerns
Pharmacotherapy for erectile disorder
- Viagra: PDE-5 inhibitor increases blood flow but only if paired with sexual stimulation
- Most people who receive a prescription do not fill it; for those who do fill it, only 50% get a refill
- NOT created as an ED medication → was originally for cardiovascular purposes
- Most people who receive a prescription do not fill it; for those who do fill it, only 50% get a refill
key main factors as to why people dont fill the prescription/refill it:
- People felt as though it did not help to take viagra
- Comorbidity (wasn't safe to take it)
- Cost (insurance used to not cover viagra/sexual health medications)
Flibanserin (Addyi) performs quite poorly in trial however it is mostly used as a treatment for low desire
- Increase in less than 1 sexual encounter a month
- Side effects: drowsiness, dizziness, nausea, fatigue
- Addyi is taken more like an anti-depressant (daily) while for viagra it is right before any sexual encounter
Flibanserin is quite polarizing
- Evening the score – social need for having “evenness” between sexes
- New view campaign – maybe there are other factors that are influencing why sexual desire is at an all-time low. We should consider other factors more as well
Lidocaine – topical treatment that is applied before sex + nightly before cotton swab to numb in order to avoid pain
- Downside: Has the potential to cause burning, there are challenges to engaging with treatment
- Lidocaine does not address all behaviors (like avoidance behavior)
- First line treatment
Pelvic floor physiotherapy
- First line treatment
- Vaginal inserts
- The pelvic floor plays a role in sexual functioning → there are rhythmic ejaculation processes
- If individuals have tight muscles, they may struggle with tense muscles and concurrently tense muscles in their pelvic floor
- Common for tight pelvic floor muscles at 5-7 o'clock of the vagina (clitoris as 12 pm) (the back end)
- The pelvic floor is supposed to move with the diaphragm – practicing breathing and moving
Cognitive behavioral therapies
- Focusing on the interaction between thoughts, behaviours, and emotions
- Being able to break down sensations is important
Evidence-based psychological treatments
- Individual, group, and couple cbt (where individuals dont have as much knowledge about what to expect during specific contact
Treatment for premature ejaculation
- Stop and Squeeze method
Psychoeducation
- Education on sexual response cycles
- Education on changes due to aging
- Educating oneself!!!
Restructuring unhelpful thinking styles ** similar to cbt
Communication skill training
- Reflective learninghan214
- How do people meet sexual challenges
- How do people talk to each other
- Is communication harsh? Open?
Sensate focus
- Touching exercise where they touch each other in a non (necessarily)-sexual way in order to pay attention to your own interests and the sensations that you feel
- Point: getting away from the pressure of if you are doing right but more on what things feel like
- Literature has shown that sensation improves arousal
- Distraction management!!!
Intrapsychic - personal factors, the psychological factors that have come to play since childhood/ capable of impacting one’s interactions
Interpersonal - in relation to others
Cultural + psychosocial - social scripts and religious teachings that have to do with sexual interactions later along the line
Family based teachings
School based teachings
There is still a lot of misinformation regarding things like hormones – people perceive it as the single one sided defining factor for particular situations. However, hormones are very capable of being a biological factor that influences women who are (postparturm) recent mothers
Neurological disorders + central nervous system injuries
Drug related disorders
- Increase in iatrogenic reasonings for sexual disorders by a double
- Psychogenic only accounted for 90% before but now it only accounts for 80%
Aphrodisiacs do not exist – strict placebo
Hormonal contraceptives are capable of having an influence
Quality of sexual contact can also impact sexual dysfunctions
Article by Katrina Bouchard
DSM5 sexual dysfunctions:
- Male hypoactive desire disorder - absence of arousal and desire considering factors that could potentially influence
- Delayed ejaculation
- Erectile dysfunction - pde 5
- Premature ejaculation
- Female orgasmic disorder
- Female sexual interest/arousal disorder
- Genito pelvic pain penetration disorder - tensing of pelvic floor muscles during penetration
Criticisms regarding dsm5 diagnoses tie to how they diagnose based on sex, diagnose based on an independent case’s low arousal desire (and fail to consider how this could play into partnered sex –pathologizing one person’s low arousal), lack of regard for comorbidity with anxiety and ptsd etc.
Masters and Johnson – 4 stage linear model of sexual arousal from observation
- Excitement, plateau, orgasm, resolution
Kaplan - 3-stage triphasic approach to sexual arousal that includes a psychological aspect – desire
- Desire, arousal, orgasm
Basson - circular theory of sexual arousal that incorporates physiology, context, and partner(s) into the picture to better understand and validate all individual’s experiences of sex
- Not everyone can orgasm, not everyone aims for orgasm, there is no one right script.
As research continues to grow there is a continued need to understand biopsychosocial connections to interpersonal connections in the study of sex, gendersex, and sexology
- Emphasis on a more interdisciplinary approach to sex research and therapy
Process of evaluating a sexual dysfunction →
1. Interdisciplinary team
2. Clinical interview (4 ps)
- PLISSIT MODEL – Permission, Limited Information, Specific Suggestions, and Intensive Therapy
3. Self-report questionnaires – that measure arousal or erectile conditions
Treatment for sexual dysfunctions
- Biomedical treatment - viagra and PDE 5, ongoing search for the female equivalent (there is currently no drug that is 100% equivalent without offering serious side effects) (brings upon the question of – does this aspect of equality really matter as there is genital differences and other factors that influence gendersexes differently
- Evidence-based therapy –like certain forms of cognitive behavioural therapy that are mindfulness based however more tailoring is needed
- Therapeutic approaches in sex therapy
- sensate focus:
- Sensate focus encompasses a series of exercises involving touch without goal-oriented expectations related to sexual desire, arousal, pleasure, or even enjoyment or relaxation
- Therapy to manage thoughts and understandings
- Cognitive behavioral framework restructuring
- How to turn way bad thoughts and insecurities one has during a relationship?
- Additional methods to understand turn-ons and offs
- sensate focus:
It is also crucial to remember that diversity in treatment is key → individuals growing up in highly sex-negative/ high religious spaces may need different types of support and different access to education
- Acknowledging that there are different barriers that sex therapy should aim to cross depending on individuals affected
intra-vaginal ejaculatory latency time (IELT). The new criteria diagnose men as premature (early) ejaculators if they ejaculate within 60 seconds of penetration 75 percent of the time for a period of six months or longer
Anorgasmia in women - persistent inability to achieve an orgasm.
Dyspareunia- Pain during intercourse—or, more broadly, pain related to sex—is known as dyspareunia.
Genito-Pelvic Pain/Penetration Disorder
There are two major elements or features of genito-pelvic pain/penetration disorder (GPPPD). The first is pain and/or fear of pain, while the second involves a significant muscular component.
- Stretching the muscular component can be extremely helpful + pelvic exercises
- Pelvic floor exercises
Treatment models should be focused more as well, not only the statistics