emt medications
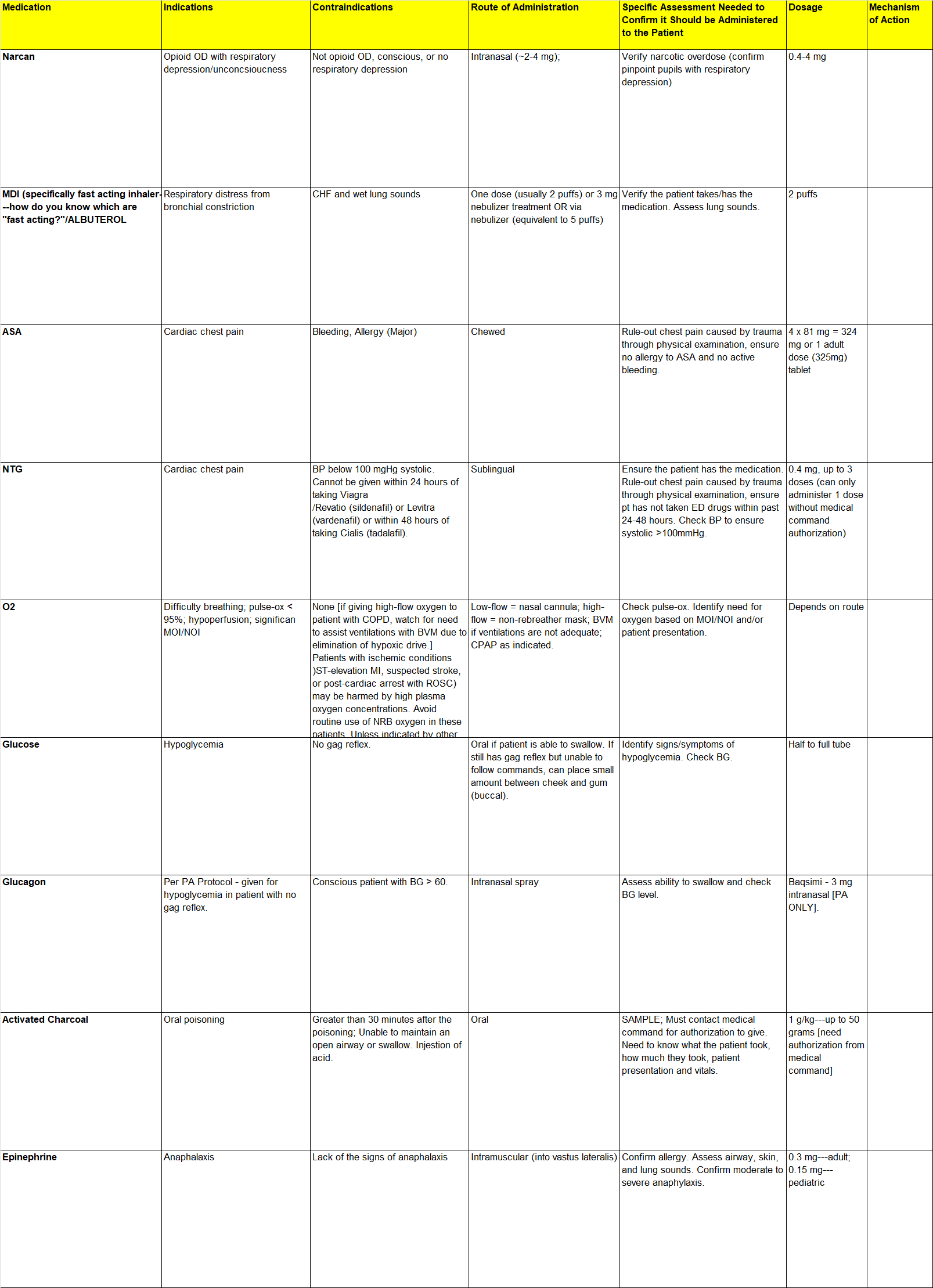
Medication | Indications | Contraindications | Route of Administration | Specific Assessment Needed to Confirm it Should be Administered to the Patient | Dosage | Mechanism of Action |
Narcan | Opioid OD with respiratory depression/unconcsioucness | Not opioid OD, conscious, or no respiratory depression | Intranasal (~2-4 mg); | Verify narcotic overdose (confirm pinpoint pupils with respiratory depression) | 0.4-4 mg |
|
MDI (specifically fast acting inhaler---how do you know which are "fast acting?"/ALBUTEROL | Respiratory distress from bronchial constriction | CHF and wet lung sounds | One dose (usually 2 puffs) or 3 mg nebulizer treatment OR via nebulizer (equivalent to 5 puffs) | Verify the patient takes/has the medication. Assess lung sounds. | 2 puffs |
|
ASA | Cardiac chest pain | Bleeding, Allergy (Major) | Chewed | Rule-out chest pain caused by trauma through physical examination, ensure no allergy to ASA and no active bleeding. | 4 x 81 mg = 324 mg or 1 adult dose (325mg) tablet |
|
NTG | Cardiac chest pain | BP below 100 mgHg systolic. Cannot be given within 24 hours of taking Viagra | Sublingual | Ensure the patient has the medication. Rule-out chest pain caused by trauma through physical examination, ensure pt has not taken ED drugs within past 24-48 hours. Check BP to ensure systolic >100mmHg. | 0.4 mg, up to 3 doses (can only administer 1 dose without medical command authorization) |
|
O2 | Difficulty breathing; pulse-ox < 95%; hypoperfusion; significan MOI/NOI | None [if giving high-flow oxygen to patient with COPD, watch for need to assist ventilations with BVM due to elimination of hypoxic drive.] Patients with ischemic conditions )ST-elevation MI, suspected stroke, or post-cardiac arrest with ROSC) may be harmed by high plasma oxygen concentrations. Avoid routine use of NRB oxygen in these patients. Unless indicated by other complications, apply oxygen only if room air SpO2 is <95% and titrate oxygen to attain SpO2 in range of 95-99%: | Low-flow = nasal cannula; high-flow = non-rebreather mask; BVM if ventilations are not adequate; CPAP as indicated. | Check pulse-ox. Identify need for oxygen based on MOI/NOI and/or patient presentation. | Depends on route |
|
Glucose | Hypoglycemia | No gag reflex. | Oral if patient is able to swallow. If still has gag reflex but unable to follow commands, can place small amount between cheek and gum (buccal). | Identify signs/symptoms of hypoglycemia. Check BG. | Half to full tube |
|
Glucagon | Per PA Protocol - given for hypoglycemia in patient with no gag reflex. | Conscious patient with BG > 60. | Intranasal spray | Assess ability to swallow and check BG level. | Baqsimi - 3 mg intranasal [PA ONLY]. |
|
Activated Charcoal | Oral poisoning | Greater than 30 minutes after the poisoning; Unable to maintain an open airway or swallow. Injestion of acid. | Oral | SAMPLE; Must contact medical command for authorization to give. Need to know what the patient took, how much they took, patient presentation and vitals. | 1 g/kg---up to 50 grams [need authorization from medical command] |
|
Epinephrine | Anaphalaxis | Lack of the signs of anaphalaxis | Intramuscular (into vastus lateralis) | Confirm allergy. Assess airway, skin, and lung sounds. Confirm moderate to severe anaphylaxis. | 0.3 mg---adult; 0.15 mg---pediatric |
 |