W6: Myopia Myths
Commonly held beliefs that lack evidence
Previous
Low-Dose (0.01%) atropine slows myopia progression (Resolved: Barely)
Because 0.01% atropine offers limited long-term benefits, clinicians now favour higher concentrations—such as 0.05%—to achieve meaningful myopia control.
Relative peripheral hyperopia leads to myopia development and progression in children (Unresolved)
There is insufficient evidence to support peripheral hyperopia as a primary driver of myopia progression. 3
Under correction slows progression–Unresolved?
There is no strong evidence that under correction slows myopia progression, but consistent full time wear of myopia control lenses—especially during near work—is likely critical to maximize treatment efficacy.
Percentage treatment effect remains constant over time–Resolved (False)
Treatment efficacy typically declines after the first year, making fixed percentage estimates misleading over the long term.
Percentage effect applies uniformly across patients - resolved (false)
absolute treatment effects are more consistent across individuals, while percentage effects can overstate benefits in fast progressors.
Screen time directly causes myopia – Unresolved
Screen use is not a proven cause of myopia, though it may contribute as part of overall near work habits.
More outdoor time slows progression – Unresolved
Outdoor time modestly slows myopia progression and may be a helpful adjunct, though its main benefit remains in preventing onset.
The impact of outdoor activity on myopia incidence is due to daylight (Partially Resolved: Not Entirely)
Although researchers often credit outdoor light exposure as the key factor in preventing myopia, current evidence suggests that optical clarity and visual experience—not daylight alone—play a more significant role in modulating eye growth. 9
Subclassifications for myopia are effective (Partially Resolved: False)
The risk of vision impairment increases with every diopter of myopia—regardless of severity— making the focus on “high myopia” alone misleading, as even low and moderate myopia contribute significantly to long-term visual complications.
Myopia is a condition with a negative dioptric number (Resolved: False)
Myopic eye growth begins before refractive error turns negative, making early identification and intervention in pre-myopes essential
Newer beliefs that lack evidence
Myopia is an optical disorder, not a disease. (Partially Resolved: False)
Despite lingering debate, growing evidence and public health consensus support classifying myopia as a disease due to its long-term risks.
Accommodative lag leads to myopia onset and progression. (Partially Resolved: False)
Studies show no causal relationship between accommodative lag progression. and myopia development and
Myopia stabilizes in the teenage years. (Resolved: Not necessarily).
Although average progression slows by age 16, many individuals continue to progress into their 20s and beyond.
Only fast-progressing myopes need to be treated. (Resolved: False)
Waiting for rapid progression before initiating treatment risks missing the opportunity to reduce long-term severity and associated disease
Fast progression during treatment means the child is a non-responder. (Resolved: Not necessarily)
Ongoing progression does not imply that the treatment has failed, since clinicians must assess benefits relative to the progression they would expect without treatment.
Soft contact lenses cause myopia progression. (Partially resolved: False)
Contrary to early concerns, soft lenses do not worsen myopia and may even reduce peripheral hyperopia in some cases.
Red light therapy is safe and effective. (Partially resolved: Not necessarily)
While early results are promising, safety concerns about retinal exposure and high rebound rates raise significant caution.
Orthokeratology, or any contact lens wear in children, is dangerous. (Partially resolved: False)
With proper hygiene and fitting, contact lenses—especially OrthoK—are safe for children and carry low rates of serious complications.
Rebound is the difference between growth during treatment and after cessation (Resolved: False)
True rebound should be measured against untreated controls, not prior treatment rates, and is minimal for most interventions except atropine and red light
Myth busters in myopia management
Myth 1: Slowing Myopia by One Dioptre Won’t Make Any Difference
Myth 2: 0.50D Per Year Is Normal Myopic Progression
Myth 3: Myopia Stabilises at Age 15
Myth 4: Last Year’s Progression Allows Me to Make Informed Decisions About Management Options
Myth 5: Young Children Cannot Handle Contact Lenses
Myth 6: Vision Is Worse with Myopia Management Options
Myth 7: It’s Impossible to Practice Myopia Management Without Being Able to Measure Axial Length
Myopia New Frontiers
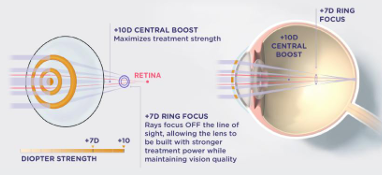
J & J Abiliti
New myopia control daily disposable silicon hydrogel contact lens
Released August 2025
RingBoost technology is key to the lens design, allowing the lens to have stronger treatment power while maintaining vision quality.
Good vision and comfort.
Slows axial elongation by 0.25mm over 2 years
65% had no myopia progression
Light Therapy: MyopiaX Dopavision
Virtual reality headset game.
Several minutes, twice daily
stated to be fun and easy for children
Delivers targeted bright light to the optic nerve head.
Suggested mechanism is modulation of retinal melanopsin-mediated dopamine release.
Increased choroidal thickness and decreased axial elongation
VR vertigo was the most common adverse event
Diet: Omega 3 levels
Researchers monitored diets via questionnaires of over 1,000 children aged 6 to 8 years.
Children with the lowest intake of omega-3 fatty acids had the longest axial length.
Children with a greater intake of omega-3 had the shortest axial lengths.
Individuals with greater intake of saturated fats—found in foods such as butter, palm oil, and red meat—had a more pronounced indication of developing myopia
AI and digital tools
AI has the potential to support multi-factor inputs and analysis for myopia risk, through evaluation of population data and verification against individuals.
A novel AI algorithm called DeepMyopia, which was trained on over 1.6 million fundus images and tested on additional Chinese multi-site data sets to successfully predict myopia onset within one, two, or three years.
Using multifactorial data, it was able to accurately stratify children into low and high risk. These two groups then underwent intervention of less (<120 min/day) or more (≥120 min/day) outdoor time, with those identified by DeepMyopia showing less myopia onset overall compared to those with risks isolated through non-cycloplegic metadata.
The authors state that AI can be used to support early detection of myopia and prediction of intervention effectiveness
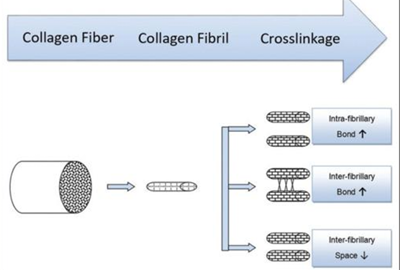
Scleral Cross-linking
The axial elongation changes the scleral biomechanics, with development of posterior staphyloma and sclera thinning. An approach to treatment progressive myopia is to prevent the sclera from expanding using scleral cross-linking.
Scleral cross-linking causes increased stiffness of the scleral tissue by forming new covalent bonds between collagen fibres and decreasing the space between fibres.
UV-A light and the photosensitizer riboflavin have the potential to increase the biomechanical strength of the sclera and slow the development of myopia.
IVMED-85 is a non-surgical, non-invasive, non-atropine eye drop that strengthens scleral and corneal collagen crosslinks.
Why does BV matter in myopia management?
Binocular vision assessment adds so much more to your clinical picture, ensuring that your patients not only have good acuity but can also see comfortably for reading and learning.
BV can help us to identify children at risk of myopia
BV can help identify children who will respond to progressive addition spectacle lens treatment
BV is altered in contact lens wear, and could be related to efficacy
BV can influence our prescribing choices for comfort and acceptance
The role of accommodation and binocular vision in the development and progression of myopia is not fully understood.
Aspects of blur from the lag of accommodation, the impact of spatial frequency at near work, and a short working distance may all be implicated in myopia development and progression. The response of the ciliary body and its links with changes in the choroid are still being explored.
Researchers have not ruled out the role of the accommodative system, but current methods of intervention based on this theory have not yielded significant results