gay stuff - chp . 12 booooo
blah blah blah
mental disorders are basis of behavior symptoms instead of physciological measurements. 12% of our global population are affected by major psychiatric disorders. every 1 in 5 people in the U.S which is 20% of popele will have psychiatric symptoms in the course of year. the rates for women are a lot more higher than for men because females are more likely to be dperessed. Also druge dpeendency alscholims is more frequence in males. scizophrenia last for a lifetime, for some it appears and disappears, schizophreinia is a public health problem because people with this become homeless. major symptoms are auditory hallucinations, highly personalized delusions, changes in emotion, and congintive impairments. there are postiive symptomsthat are abnormals behvairoal states have have been GAINED - like hallucinations, delusion, and ecvited motor behvaior such as psychosis, and negetive symtooms that have been reduced such as emotiaonal dna motivational impairments. Like slow improvered thoughts and speech, emotional and social withdrawls.
if schizophrenia can be inherited, relatives of people with schizophrenia should show a high indecident than is found in genreal population, the risk of schizoprenia among realvtives shoud increase with the clsoeness of the relatiosnhipe. parents and siblings of people iwth shozophren have a higher risk of developing schizophrenia than do indivudalds in the general population. The mode of inhertiance of schizophrenia is not simple, its not about revessive or dominant genees its about multiple genes playing a role together. so the closer somoen is related to someone iwth schizophrena that greater the chance that person is getting schoziphrenia. so like monozygotic twins is more likley, parents, siblings, childrens. in twins like identical twins, who deried from a single fertilzied egg have the same set of chenes and ar emorelikely to have schizophrenia if one has it the other one is 50/50 this is concordance. higher concordance in the gentically indeitcal twins the stronger evicence o a gentic factor. genes alone cannot fully exeplain if a person will have schizophrenia. sublte neurological sings such as impaired motor coordiaiton and difficultyr with smooth movments of the eyes to fololow a moving taryget are also common in people who are high risk of developing schizophrenia and in their realtives. there are genetic and environmental orgisin of scitozphrenia.
indiviual genes - it has been difificult to identiy any gene that causes it to develop or increaswe it. 100 genes infleunce liklihood. some genes are known to participate in snyaptic plasitity - one mutant is DISC 1, is linked to schizophrenai suscptibility.
children fathered by older men have a high reisk of developing schizophrenai, this might be because they are the produce of cell division than the sperm of younder men and older men have more opportunitiy to accumulate mutations by errors in coping chrosmomes.
prenantal stress such as infections during preganncy also increase the likelihood that a baby will develop schizophrenia later in life. If mom and baby have incomptabily bloodtypes, diabetes fror the mom, or low birth weight also add onto schizophrenia development, also if the fetus lacks oxygen. Relative minor stressors make a big difference. each stage of the fetus has its own vulunerability to schizophrenia,. complications before, during delivery, childhood and adulthood. alteration of the braind evelopment in people with schizophreinia is indicated by the acceleration of the normal thinning of cortical gray matter resulting from synapse rearragnment. once schizophrenia is developed, the person s behavior and physcial state of the brain are altered too.
- symptoms of schizphrenia can be marked and persistneged, pepole hyopotheized early on that the brain of pple with this have distincitve and abnormalities, ct and mri scands will confirm this idea. most people with schizophrenia have enlarged cerebral ventriles, lateral ventricles. Brain size doesnt affect ppl with schisophrenia, the enalrged ventricles come at expernse of the brain tissue. Possibe changes in brain structure - limbic system structure like the hippocampus and amygdala - tahat run along the laterla ventricles. So the volume of the cerbral ventricles , relative to overal brain zie, is greatin in peole with schizophrenia. because it takse up more tissue space. twin with schizophrenia have large lateral ventricles. those ppl with schizoprenai who have larger ventricles benefit less from antipsuchotic drugs.
disabled version of the gene DISC1 is associated with schizophrenia in one large family, The disc1 protein normally regulates trafficing of moelcules within enurons. So disc1 causes large lateral ventricles.
ppl with schizo have different corpus callosum. they also ahve accelerated cortiacal thinning. they also have impaired on neuropsuchological test that are senstive to frontal cortial lesions. frontal cortex activity is atypical in schizos. ppl with scizo have reduced metabolic activity in the frontal lobes. This is hypofrontality hypothesis that frontal lobes are underactive in ppl with schizo. these ppl have dendrites in the frontal cortex with reduced dentisty of synaptic spines which leads to less active frontal cortex. there are drugs that allivate the symptoms and increase frontal cortex.
ppl were so desperate they turned to lobotomy whic severed the protion of the frontal lobes from the rest of the brain as treament. this was bad as fuck instead they discovered the drug chlorpromazine whcih replaced lobotomy, it reduces postive symptoms of schizophrenia like hallucinations, delusion, disorderd thinking.
chlorpromazine and other anutphsycotic drugs were discovered. they block postynaptic dopamine receptors like the D2 receptor. Thi si sude to the dopamine hypothesis l that people with schizo have excess dopmaine rlease or receptors. hgih dose of amphetamine cause an excess of dopamine to accumulate in snapse reuslting in transient amphetiamine pyschoisi like schizoprenia and is revered by treament with antischophrenic mediation,
LSD and psilocybine are hallucinogens that act through sertonin receptors and produce effects that ber little resemblance to pyschosis,
first generation antupshotics - d2 receptor antagonist. haloperdoils has greater affinity for d2 receptors and became a widely used drug. treating ppl with parkisons disease with l dopa (metabolis recuror of dopamine) may induce shcio like symptoms by boosting snyaptic availability of dompaine. Ppl who stop getting these first gen antupshotic will resutl in increase in postiive schozo delusions. this supersentiivty psychosis though to be a rebound effect where chronic supression of dopamine enyrotrans causes an uprelation of dpamine receptors and can be reveresed by the increase dosage of doampine receptor blocking agents. So drugs with higher affinity for d2 erceptors can treat schozo at lower doses. there are problems with dompai hypothesis of schizo. There is no correspondence between speed with which drug block dompaine receptor and how long it takes for the ysmptoms to diminish 30 percept of ppl with schizo dont repsond to dopamoine antagonist. second gen antupschotics work with motor side effects. they have moderate affinityt for d2 receptors. second gen anti have their highest affinity for the other trasnmitr receptors clozapine, which blocks serotonin receptors 5th2a receptosr and other. Second gen is more affective than first gen. it relieves negative symtoms and psotive symtomes releived by first gen. second gen cause wiegh gain and other health problems. antipscyhpotic meds can relive symptoms at the onset of schoizo, . they arent so helpful for long term use. it works for replease in the first two years. PCP phencyclidine was used as a potent psychotomimetic, it preoduces strong resombling postive and negative sympomts as schoz. PCP ppl experience hallucinations, depersonalizaiton, disoreitnation, and can become violent, prolong psychotic states can develop with chronic use of PCP.
PCP acts as an NMDA receptor antagonis wich blocks the NMDA receptors central calcium channel, it prevents the ednogenous ligand gluamtate from bidning. It also results in senstive to prefrontal dmaamge. This proposs a glutamamte hypothesisi that schoz can come from defetive glumatmate transmittiosrs. Drugs that sitmulat the ionotopic nmda receptors tend to produce seizure so NMDA receptor agonist is not an option. Instea dresearchers are focusing on mantupualtors of other types of lgumatate receptors - the metabortopic gluamte receptors mglue - there are eight different subtypes.
12.2 -
distubrance of mood -
depression - unhappy mood, loss of interest, reduced energy, changes in appepetitie, and sleep pattterns, loss of pleasure in most things. diffulcty in cocnetration restless gaitation or torpor is common. depression can occur with no readily apprenet stress, and without treament the depression last longer. more than 7 percent of american adults experienceat least one perodise of clincally singificant depresson, This is more common in ppl over 40 espeically women.
depression can be suicidal. more than 500 ppl were prevented jumping off goldeng ate bridge, only 6 percent later went on to die by suicide. genetic studies of depressive disorders reveal strong hereditary contributions. the concordance rate for identical twins is subtaintially higher than for faternal twins. there is no single gnee repsonsibel for depression. difference in the brain of ppl with depression focus on the functioal changes. they show changes in brain region activity. there is an increased activation in the amygdala especially evident durign emotional processing, increased activity in the frontal lob es is evident during more cogntively demaning tass. Dscreaced activitin in the partiwel and posterior temporal cortex in the an teiror cingulate cortex sysmte have been implacted in attention. Increased activity of amygdala is incovlued in mediating fear and presists after the depression has been lifted. BANEULAE - a pair of mslal nuclei located adjacent to the pineal gland, links thruogh the limbic system, basal forrebain, and midbrain. The laterlal habenulae - in particual is dysfunitonal in depression acts as a antireward center mediating the low amood and loss of pleasure. ppl with depression have difficulties regulating stress hormone release.
studies report that hippocampal volume is reduced in ppl with depression meaning reduced activaton with emmroy tast.
electroconvulsive shock therpay - is intentional induction of a large scale siezure. - this was orginally a schozo treatement and it did help but its more evedent that ECT is more rapidly revesrse severe depression. anti depressannts made ect less common. repritive trasncraninal magnetic stimulation - ids also effective for depression. pace maker is also used for mild e lextric stimulation to the vagus nerve. this is offereed where ECT has been ineffective to establish whether vatal stimulation offers a long term solutions. -
rTMS is also an effective treament which is less invasive for altering cortical acitivity. - for rare extremely difficult cases of depression - deep brains stimulation DBS - mild electrical stimulation is pplied to targets in the limbic system of the brain. via surgically implaneted electrodes as last ditch to relieve depression. effectiveness of dbs or vagal nerve stimulation for depression is difficult to evlaute. the most common treatemnt for depression is the use of drugs that affect the monoamine tramitters : norepinpherine, dopamine, and sertannin. first modern antidepressant were inhibiotrs of MAO(monoamine oxidase), the enzyme that normlly inactivates mono amine in thesynaptic cleft. This action of MOA inhibitors causes monoaminoine transmitters to accumulate to higher level in snapses. ppl with depression do not get enoough stimulation at monoamine synapses. second gen antidepressants called tricyclics inhibit reuptake of monoamines which similarly boost their snpatic activity. one want ect help depressioni. sby inducing the release of monoamines.
serotonin seems to play an important rol in depression. A class of modern antidepressants, the SSRI’s like prozac, they increase snyaptic sertonin levels in the brain, in rats ssri’s increase the birth of new neurons in the hippocampus which mediate some of the mood effects on the drug
there are problems with the idea that reduced serotonin stimulation causes depression. there are poblems that reduced serotinin stimulation causes depression. ssri drugs increase snaptic seronin within hours but takes several weeks for ssri ppl to feel better. THis suggest that the brains repsonse to increase nspatic srtonin that relives symptoms takes time. so even though boostin seroninn helps some ppl, their depression comes from otehr factors in the brain. serotonin-norepinephrine reuptake inhibitors SNRI. potantieal antidepressants are glutamate receptor antagonist ketamine. This releieves depression almost instantly and adminstered as nasal spray. SSRI and SNRI must be taken for several weeks to work. LSD can also relive depression.
treatement with cogntivie behavoiral therapy CBT, is aimed to correct negative thinking andimprove interpersonal relationships. the rate of relapse is lower for CBT than for SSRI. combination of CBT and SSRI treaments more effecitve in combating depression than either one alone. CBT hels cline recognize self defeating modes of thinking and ecourage breaking out of a cycle .
women exepeirnce more depression than men. also there is measurement of depression and post partum depression rpeceding childbirth. one out ever seven pregmenat women will hsow symptoms of depression.
anhedonia - is used to to evaluate animal models of depression . learned helplessness - a animal is exposed to a repetitive stressfuls timulus, like electric shoch that it cannot escpae. Depression, learnd helpiness is linked to decrease in sertonin funciton, also to mechanism that control the release od dopamine. the main reward signal in the brian. removing olfactory bulb also creates depression.
diffuclty falling alssep and inabilityt os maintain sleep is common in depression. EEG sleep stidies show that ppl with depression have abonmalities. this major depressive disorder is marked bya. reduction in stage 3 sleep. or slow wave. increased in stage 1 and 2. also they enter REM much ssoner. length of time before rem sleep correlated with severity of depression.
Bipolar disorder - periods of depression alternating with periods of excedssive expanis mood (mania), increased energy, overactivity, talkativness, strange grandiosity. altneration of stages varies. some ppl exhibit rapid cycling bipolar disorder where they have four or more cycles. it is more hetible . the nural basiss of bipolar diorder isnt understood. Also these ppl have enlarged ventricles on brain scans like schizo. changes is evident in several cortical and subcortical substrucutres such as the amygala, hippo, cingulate and frontal cortex.
this patter comes from changes in the brain and havior. it is more in common iwht schizo than with depression. so manic depression is abonded. it resembles the frank deliusions, ppl with some indivualds have been disanoges with bi polar diorderes more than with schizo. litium is a med. manic phases blocked by lithium may be the reason some ppl with bpolar diosrder stop taking medication. The depression returns and then the mania also.
the DSM5tr distinguishes several major types of anxiety diorsder: phhobic diorders are intense, irrational fears . panic diorders attacks of intense fearfulness. Generalized anziety diorder . excessive anxiety or worry for months. ppl who have panic attacks have temporal lobe abonmalities in th left hemisphere. amygadlaa.
the tranquilizing drug meprobamate was introduced(miltown) it became instant serller. benzodiazepines replaced miltonwn . valium is this trade name. other types of benzodiapeines are xanax, halcion, avtvian. these drugs that combact anxiety are called anxiolytics. they were also used for preventing suizures or treating insomnia.
it interacts with binding sites that are part of gaba receptors liek gaba a where they act as noncmeptitive agonist. That gava is the msot common inhibitory tranmitter in the brain. whwne gaba is released from a presnaptic terminal and activates post nspative receptors, targe neuron beocmes hyperpolarized and fires fewer aciton poritneions.

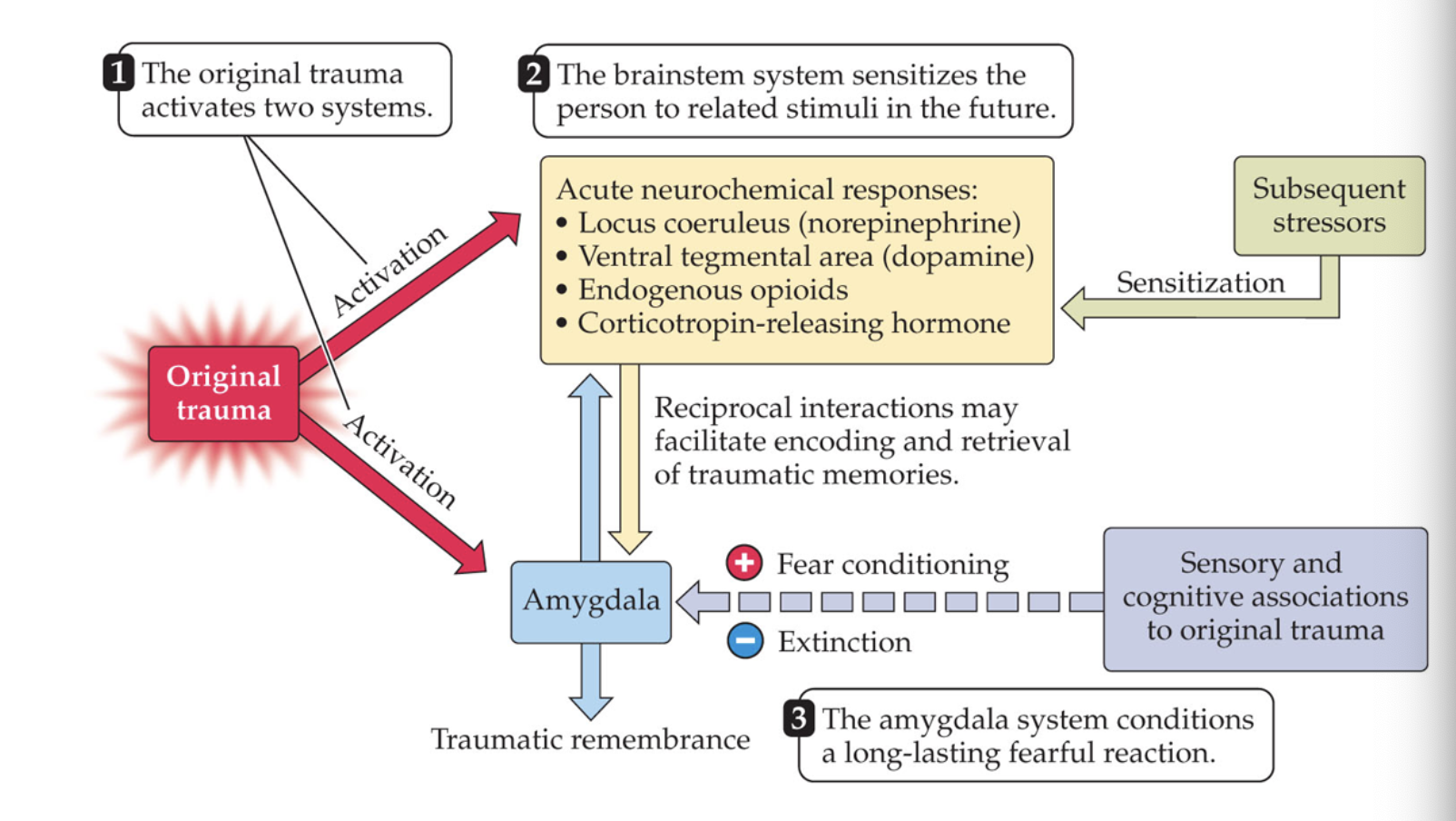
some ppl have vidid impressions after something bad happens like PTSD. they are called combat gatifue war neruosis or shell shock. it can affect anyone who has experienced a sudden distressing even. tsd ppl show meory changes like amneisa, flashbacks, deficit in short term memroy. These memory distubances suggest invoment of the hippocampus indeed the volume of the righ hipo camppus is smaller than those without ptsd. ig ppl with small hipocapus are mjore susceptible of developing ptsd from perons exposed to stress. a comprehensive biological model of the ptsd draws connection from ptsd memoruy distubances to the nerual mech of fear condition, behavioral sensitaion and extinciton. fear conditioning - memory for a sitmulus that the animals has learned to associate with a negative events. - this involves the amygdala and the brainstem pathways. presistence of memory and fear in ptsd depend on the faulure of the mechanisms to forget. ppl with ptsd exhibit a partadoxical long term reduction in cortisol with a the stress hromone, this is due to sesntigvity to coritsal. therapy for ptsd involves a increaseing clinets exposure to thsoe stimuli and conditions that trigger flashbacks . this can be cobined iwth drug that block the effect of stres hormones. MDMA can relive the symptoms of ptsd in some ppl.
ODC - reperitive retials persistent though. obsessions like fears of germs.
genome -wide associated studies GWAS allow for researchersto screen the entire genome of ppl with mental dirorder to clear many diorders are no so distince from one other. schizo and bipolar are to show strong genetic correlation.