Pathology of Pleura
Mesothelial reactions to damage
Reaction to irritation:
cell swelling,
desquamation
Unusual recovery:
Centripetal proliferation (curved around the centre)
Recombination of desquamated cells
Formation of new mesothelial cells from sub-mesothelial fibroblasts
May cause morphological diagnostic problems
Mesothelial healing
Inflammation of the pleura
Fibrinous pleurisy
Acute purulent pleurisy
Chronic purulent pleurisy / pleural empyema
Chronic granulomatous inflammation:
Tuberculosis
Sarcoidosis
Foreign body type granulomas
Acute pleurisy
Hyperaemia
Fibrinous pleurisy with pleural effusion
Serofibrinous pleurisy: Friction is reduced when exudation begins
Purulent pleurisy
Pleural empyema
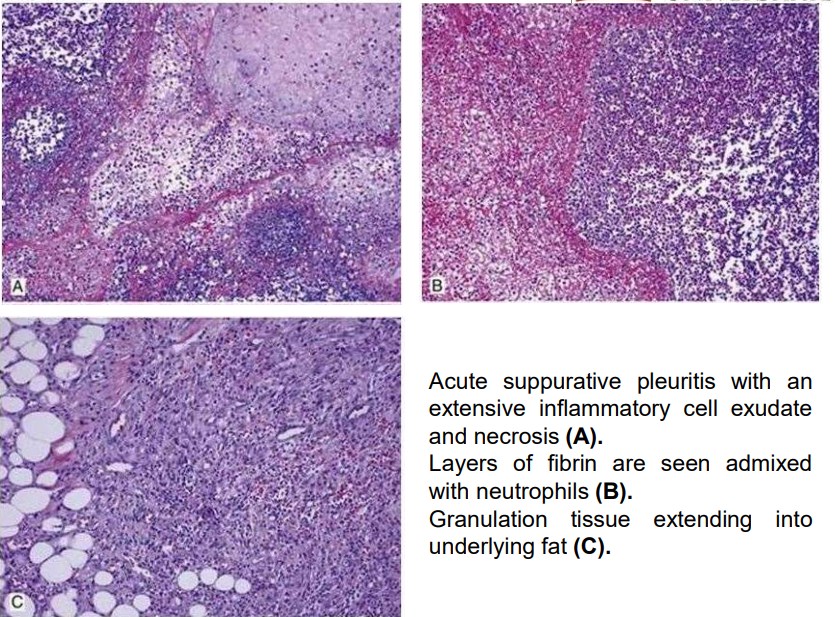
Pleura empyema
Collection of pus in the pleural space, most commonly isolated between connective tissue adhesions
Cause - bacterial infection
Contributing factors:
Diabetes
Alcoholism
Chronic lung diseases (bronchiectasis, cancer)
Immunosuppression
Surgical manipulations
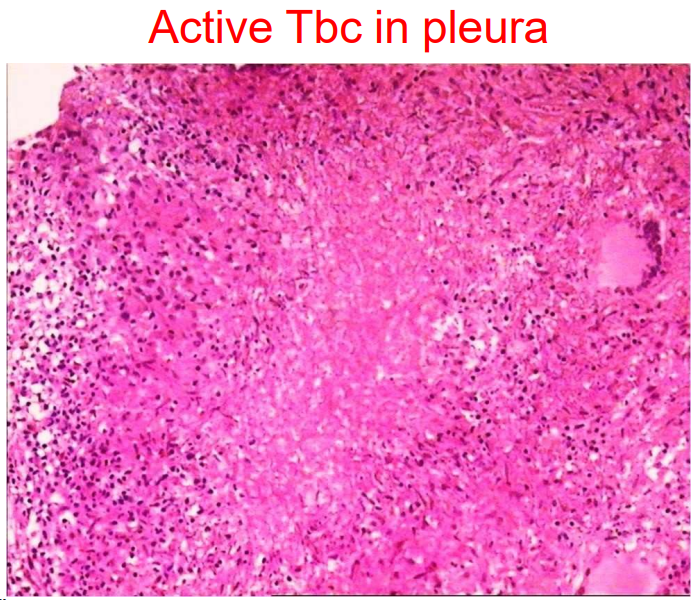
Tuberculosis in pleural tissues
Pleural damage is common in patients with tuberculosis
May be
Isolated tuberculous pleurisy
In connection with active pulmonary tuberculosis
Tuberculosis empyema if tbc cavernous erodes on pleural space
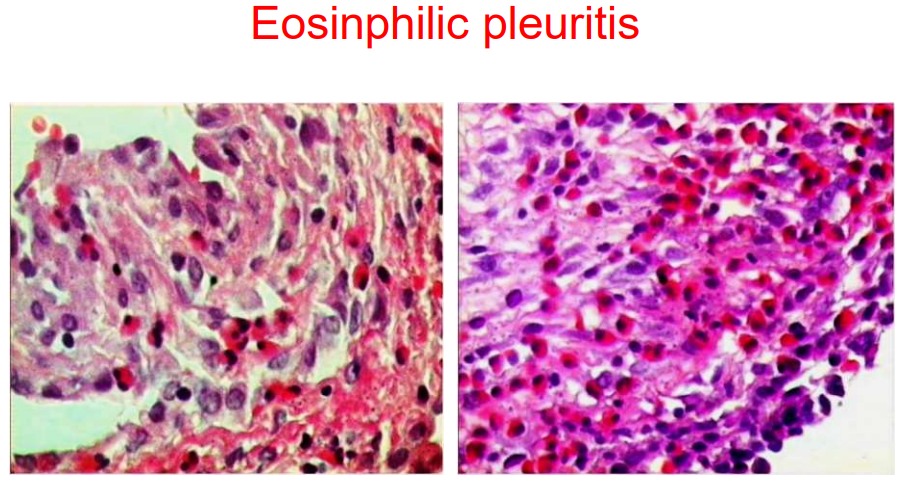
Eosinophilic pleuritis
Eosinophil pleurisy:
pneumothorax
Eosinophilic infiltrate penetrates tissue to a depth of <3 mm. Mesothelium is grossly hyperplastic.
eosinophil pneumonia
eosinophilic granuloma
malignancy
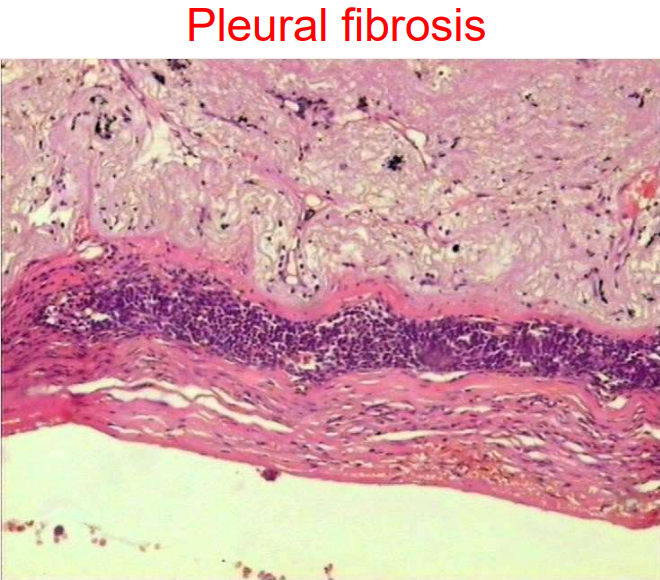
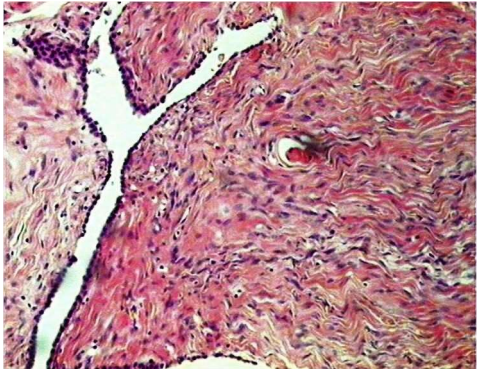
Pleural fibrosis
If fibrosis develops in the pleura, the amount of connective tissue in the pleura increases. The pleura thickens in the affected areas
Pleural fibrosis can be caused by:
Acute inflammation, prolonged
Pleural tbc
Uncommon pathologies
Asbestos-induced inclusions
Blesovsky's disease
Pleural Tumours
The most common primary pleural tumours:
Malignant mesothelioma
Solitary Fibrotic Pleural Tumour (SFPT)
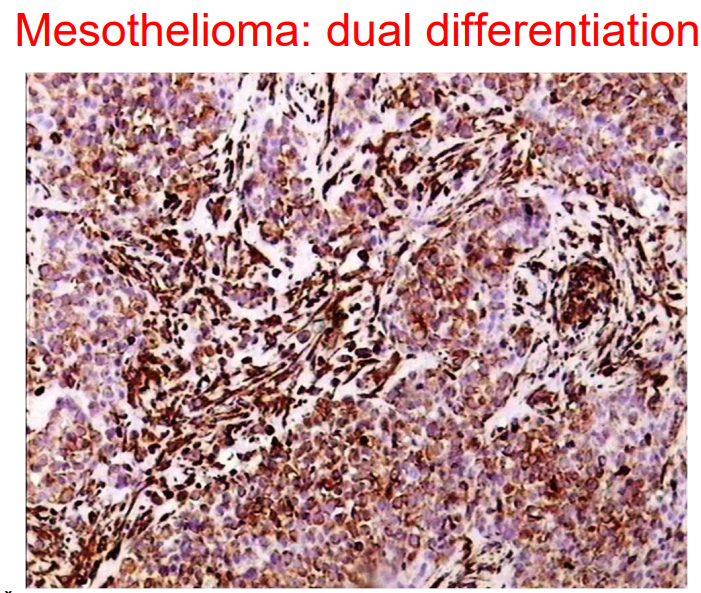
Mesothelioma s. diffuse malignant mesothelioma
Definition – malignant tumour that develops from mesothelial cells
Typical age and gender:
6th decade of life
Rarely for young people
More common in men
Fatality 100%
90% of cases are caused by asbestos
Growth and spread of mesothelioma
Diffusely spreads over the surface of the serous sheath: first small nodules, which then fuse to form a sheath
The lungs are compressed
Exudation to the pleural space
Can grow into pulmonary parenchyma and metastasize to laryngeal and mediastinal LM and further
Possible widening of the waistline to the healthy side
It grows in the adipose tissue and musculature of the thoracic wall. Typical implantation at sites of puncture, biopsy, or thoracocentesis
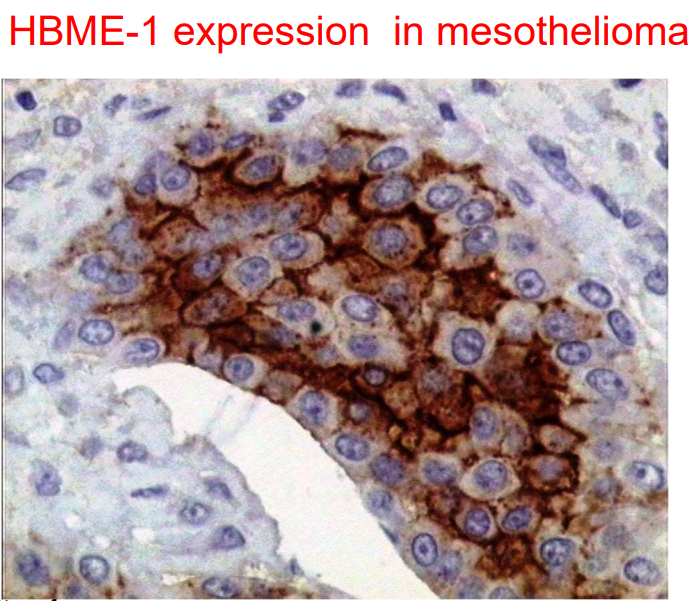
Immunophenotype: Contains calretinin and HBME-1: markers specific for mesothelium
Solitary fibrous tumour (SFT)
CD34-positive fibroblast tumour
Characteristic of the pleura but possible in any localization, e.g. orbit, kidney, deep soft tissue
Risk factors are unknown. The development of this tumour is not related to asbestos
SFT: clinical picture
May be an accidental radiological finding
Cough
Pain in the chest
Shortness of breath
Possible hypoglycaemia due to synthesis of insulin-like growth factor in tumour cells
Localized / Solitary Fibrotic Pleural Tumour (SFPT)
FOCAL INVASIVE GROWTH
benign SFPT may include mesothelium not to be confused with biphasic differentiation
benign visceral pleural SFPT can focally grow into lung tissues including alveolar epithelium
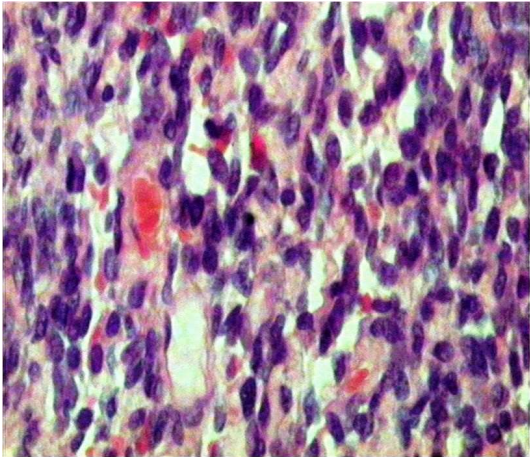
Malignant SFTP: hypercellularity and high mitotic activity
Metastatic tumours in pleura
Most common malignancy in pleura
In patients> 50 years, the 2nd most common cause of pleural effusion (after CHI – chronic heart insufficiency )
Origin
33% lung Ca
20.9% breast Ca
7.3% stomach Ca
ovaries Ca
46% of these cancers are primarily manifested by metastatic pleurisy
lymphoma