Chapter 10: Drugs & Crime ⭐️
Introduction
Psychopharmacology/Behavioural Pharmacology: The branch of psychology that studies the effects of drugs on human cognition, emotions, & behaviour.
Psychoactive drug: A substance that acts on the central nervous system & produces changes in a person’s cognitions, emotions, or behaviours.
Drugs are not always harmful; their negative impact may depend on the way they are used as well as on the context.
Distinction between licit (ex: tobacco caffeine) & illicit drugs (ex: heroin, cocaine).
Illicit drugs: substances that are illegal to possess, sell, or use.
The degree of legislative control may vary significantly depending on the jurisdiction.
Drug Use & Its Effects
Substance use: Consuming drugs at moderate levels that do not cause any significant impairment in functioning.
Substance misuse: Taking drugs/products at levels or for purposes other than those prescribed or intended
Ex: prescribed sedatives
Tolerance: A condition caused by regular drug intake, whereby a higher dose is required to produce the same effects previously obtained with a lower dose.
Withdrawal: A condition characterized by unpleasant symptoms that emerge when a person who has developed tolerance to a drug abruptly stops taking it. These symptoms are often the opposite of the effects produced by the drug, and they disappear eventually, as the body…
Major Classes of Drugs
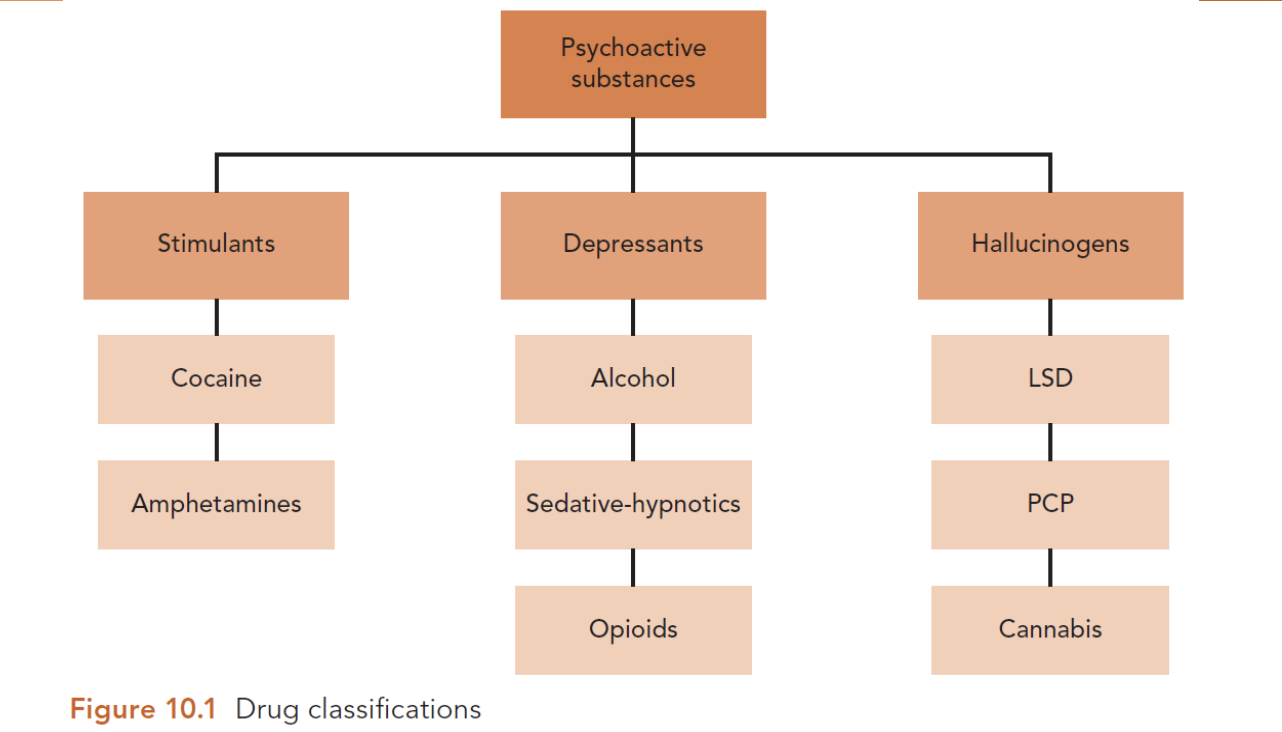
Stimulants
A class of drugs that elevate aspects of central nervous system function → increased attention, mood, & activity levels.
Nicotine, caffeine, cocaine, amphetamines.
They enhance the activity of dopamine, epinephrine & norepinephrine (reward system of the brain).
Cocaine (coca plant):
Symptoms: Alertness, euphoria, enhanced energy for about an hour.
Characteristic: The pattern of rush (euphoria) & crash (depression, hunger, lethargy).
Health risks after chronic use or high dosage: Anxiety, agitation, paranoia, psychotic break, convulsions, respiratory & cardiac arrest, death.
Amphetamines (ex: MDMA-ecstasy): They are produced in labs & are medicinally used to treat narcolepsy & ADHD (in past: weight control, depression, asthma).
Short-term intoxication effects are similar to those of cocaine; nevertheless, effects last longer & crash is less intense.
Depressants
A class of drugs that depress/slow down certain aspects of central nervous system functioning (reduced overall neural activity in the central nervous system).
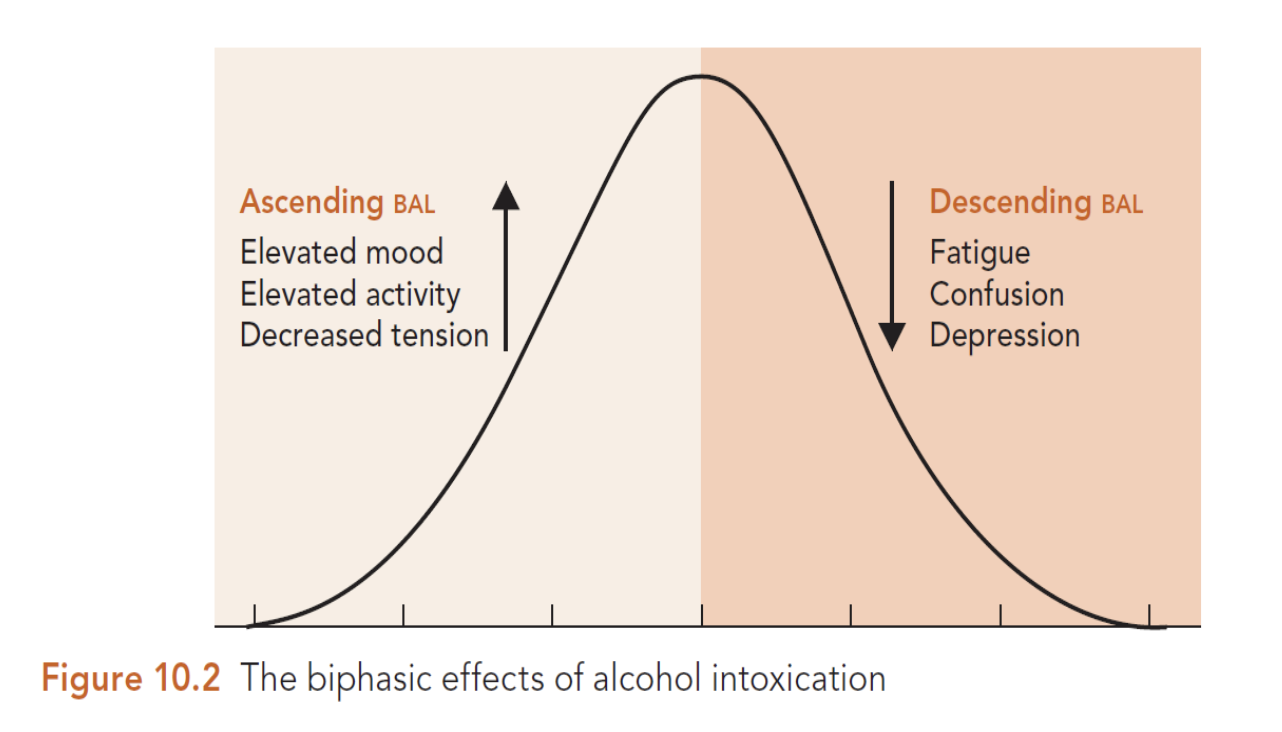
Alcohol: The most misused of all drugs. Tolerance develops quickly, but withdrawal symptoms usually appear only after chronic use, & last 7-10 days on average.
Characteristic: Biphasic effects, meaning that the blood alcohol levels increase initially & drop later on.
Biphasic Effects of Alcohol Intoxication
Sedative-Hypnotics (benzodiazepines): originally used for the treatment of anxiety & insomnia.
Common Effects: Impaired mental performance, memory, judgement; slurred speech, decreased coordination, slowed reaction time, fatigue, drowsiness.
Withdrawal Symptoms: Tremors, agitation, insomnia, nausea, seizures, coma.
Rohypnol is a potent benzodiazepine, used to facilitate sexual assaults; it is knows as the “date rape drug”.
Opioids (opium, morphine, heroin, methadone, naloxone).
Medicinal use: analgesic.
Tolerance develops quickly.
Common effects: Feelings of relaxation, pleasant mood, intense rush, dreamy-cloudy mental state, reduced psychomotor performance.
Health risks: Coma, respiratory arrest, death, as well as risks related to the context (needles, impurity of substance).
Withdrawal symptoms: Tremors, chills, cramps, vomiting, symptoms similar to those of a bad flu.
Hallucinogens
A class of drugs that are chemically unrelated but are all capable of producing hallucinations & distortions to self, space, & time.
Lysergic Acid Diethylamide (LSD): Positive mood states, euphoria, distortions of time, space, & self; visual hallucinations; flashbacks. Tolerance develops quickly; lack of withdrawal symptoms.
Phencyclidine (PCP): Euphoria, anxiety, alienation, depression, panic; Suspicious, confusing thinking.
Risk of stupor or coma after high dosage.
Cannabis (from cannabis sativa plant): Its main psychoactive ingredient is THC.
3 products derived from the plant: marijuana (lowest concentration of THC), hashish (medium concentration, & hash oil (highest concentration).
Effects: Feelings of relaxation, mild euphoria, amusement, laughter; Impairment in cognition, memory, balance, motor coordination; paranoia, disorientation, panic.
Tolerance may occur after heavy & prolonged use.
Some users experience craving, difficulty to control, & withdrawal symptoms.
Substance Use Disorder (DSM-5)
A pattern of problematic psychoactive drug use that causes significant distress or impairment & is typically associated with impaired control over drug taking & harm to the user.
In the past, it was called substance abuse, substance dependence, or addiction.
Indicators of maladaptive substance abuse:
Impaired control over drug taking
Ex: craving, inability to handle withdrawal symptoms.
The APA defines 11 diagnostic criteria.
The severity of the condition is determined by the number of presenting symptoms.
A diagnosis requires 2 or more symptoms in a 12-month period, that cause significant emotional distress or functional impairment.
The disorder is considered mild when 2 or 3 symptoms are present, moderate with 4 or 5 symptoms, & severe when there are 6+ symptoms.
DSM-5 Alcohol Use Disorder Diagnostic Criteria
Impaired control
Alcohol is often taken in larger amounts or over a longer period than was intended.
There is a persistent desire or unsuccessful efforts to cut down or control alcohol use.
A great deal of time is spent in activities necessary to obtain alcohol, use alcohol, or recover from its effects.
Craving, or a strong desire or urge to use alcohol.
Social impairment
Recurrent alcohol use resulting in a failure to fulfill major role obligations at work, school, or home.
Continued alcohol use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of alcohol.
Important social, occupational, or recreational activities are given up or reduced because of alcohol use.
Risky use
Recurrent alcohol use in situations in which it is physically hazardous
Ex: driving
Alcohol use is continued despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by alcohol.
Pharmacological criteria
Tolerance:
A need of markedly increased amounts of the substance in order to achieve the desired effect or intoxication.
A markedly diminished effect with continued use of the same amount of the substance.
Withdrawal:
The characteristic withdrawal syndrome for alcohol.
Factors Impacting Drug Effects
Most of the drugs activate the brain reward systems, particularly those involving dopamine.
In the beginning, drug use is pleasurable & rewarding. When the brain reward system adjusts to the drug’s chronic presence, drug use starts to become problematic.
More pleasurable & rewarding drug use experiences pose a greater risk of later problematic drug use behaviour. The nature of the experience depends on…
Drug-Related Factors
Drug type: Different drugs produce different effects because of their different neurochemical action; some effects are more pleasurable than others.
Route of administration: Intravenous injection or inhalation produce more intense effects compared to oral use.
Dosage size: Larger doses produce more intense effects.
Person-Related Factors
Physical attributes
Ex: body weight
Substance use history
Ex: tolerance
Psychological expectations.
Set & Setting
Set: Anything related to the internal state of a person, including personality, preparation for the experience, intention, as well as “mood expectations, fears, wishes”.
Setting: Anything related to the environment in which the experience takes place, including the physical environment, the emotional/social environment, & finally the cultural environment - the ideas & beliefs which are prevalent in the society regarding drug effects & the world in general.
The Drugs-Crime Link
There are 3 major models that examine the drugs-crime link.
Drug use leads to crime
Ex: Goldstein’s tripartite model
Crime leads to drug use
Ex: subcultural theory, self-medication hypothesis
Drug use & crimes have a common etiology
Ex: reciprocal model, relationship constructed by policy & law.
Goldstein’s Tripartite Model
Paul Goldstein (1985) developed a framework to describe the drug-violence connection, which can be adapted to fit other crimes.
Goldstein identified 3 possible links:
Systemic violence
Economic compulsive violence
Psychopharmacological violence
Systemic Crime
A form of drug-related crime that occurs because the drug trade is illegal & its participants cannot turn to authorities for assistance.
3 dimensions of systemic crime:
Organizational crime: related to the establishment & operation of the organization
Ex: member’s misconduct, rivalry with other groups, bribing state officials.
Transaction-related: systemic crime typically revolves around a business deal, or the seller-buyer interaction.
Ex: disputes over the payment or the drug quality/quantity resolved with use of violence.
Third-party: systemic crime involves people at the periphery of the drug trade (illicit drugs are part of a broader illegal market, ex: prostitution, protection rackets). Then, criminal & violent behaviour from the drug trade can spill over.
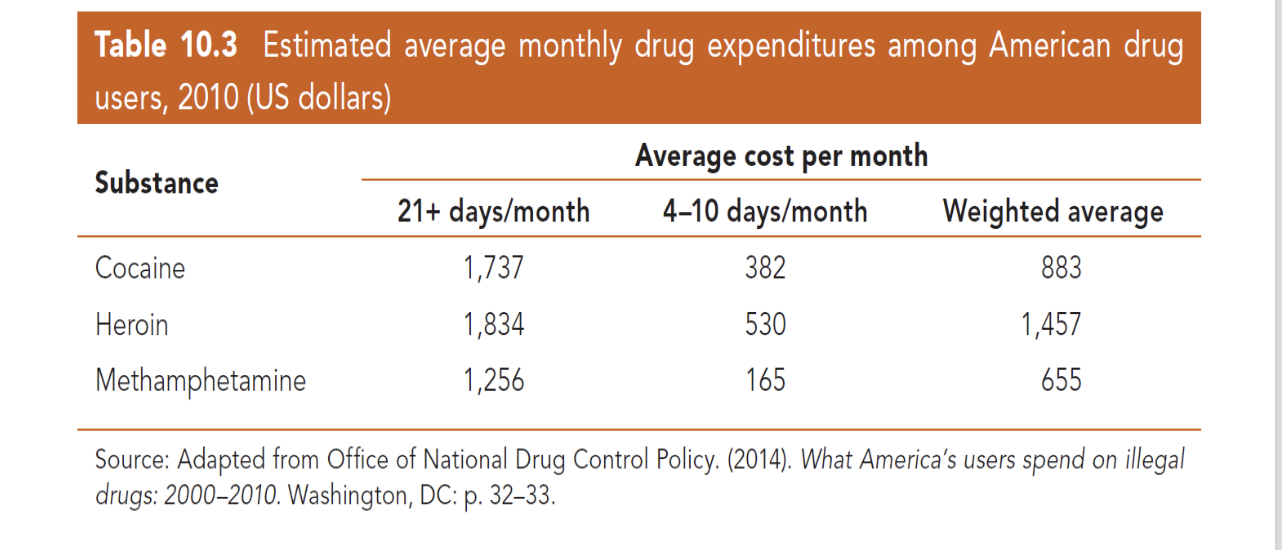
Economic Compulsive Crime
A form of drug-related crime that occurs as a result of drug users engaging in illegal behaviour as a means to support their drug habit. Mostly non-violent offending.
Ex: stealing drugs, illegal commodities bartered, drug dealing.
It is estimated that 20-30% of arrestees & inmates in USA & UK committed their offence to purchase drugs.
The level of drug use & the cost of preferred substance are the factors that determine the financial cost of using…
Psychopharmacological Crime
A form of drug-related crime that occurs as a result of the acute & chronic effects produced by a psychoactive substance.
It is estimated that 25-50% of incarcerated offenders in North America report being under the influence of a psychoactive substance at the time of their offence.
The fact that one is intoxicated while offending does not prove that the substance caused the person to commit the crime; the effects of intoxication, withdrawal or long-term neurological changes could increase the likelihood of crime & violence.
Stimulants
Amphetamines most frequently implicated with violent behaviour (correlation).
Inconsistent findings regarding cocaine use & violence.
Stimulants enhance arousal, mood, activity → increased potential for interpersonal conflict.
Paranoid delusions and/or emotional instability/impulsivity.
Hallucinogens
They exhibit the weakest relationship to crime & violence.
PCP use: unclear relationship with violent behaviour. LSD: no evidence.
Cannabis withdrawal (but not intoxication) can induce aggressive & violent behaviour.
Depressants
Disinhibition, poor judgement.
Alcohol: Most strongly associated with crime & violence.
Benzodiazepines: Dose-dependent psychopharmacological effects (low doses related to aggressive behaviour).
Opioid intoxication does not seem to facilitate aggression (“reverse psychopharmacological effect”), but withdrawal may have this effect).
Ex: unbearable symptoms, or self-medication hypothesis.
Theories of the Alcohol-Violence Relationship
3 categories of theories
Disinhibition theories
Cognitive disruption theories
Expectancy theories
Disinhibition Theories
Alcohol depresses functioning in areas of the brain responsible for behavioural control and, as a result of intoxication, behaviours normally suppressed are exhibited.
Alcohol intoxication does not inevitably lead to aggressive behaviour; its influence depends on individual characteristics & circumstances.
Selective disinhibition: According to Parker & Rebhun (1995), the effect of alcohol in the disinhibiting violence depends on the perceived effectiveness of acting violently in the particular circumstances.
Active constraint: The relatively large conscious & deliberate effort needed to act in a socially acceptable manner in situations where acting violently is perceived to be an effective & desirable course of action. The level of intoxication required to override active constraint is contingent on the person & the situation.
Passive constraint: The relatively small conscious & deliberate effort needed to act in a socially acceptable manner in situations where acting violently is perceived to be an ineffective or undesirable course of action.
Cognitive-Interference Theories
Alcohol intoxication impairs human social cognition (ex: encoding & processing of information) in ways that increase the chance of aggressive & violent behaviour.
Misinterpretation of thoughts & actions of others during social interactions (ex: misunderstandings → increased chance of inappropriate or violent behaviour).
Information processing errors are attributed to the temporary psychopharmacological effects of alcohol (not to the individual’s way of thinking that is stressed by information processing theories).
The self-awareness model: People must be actively conscious of what they are doing in order to evaluate their conduct against relevant internal & external standards of behaviour.