Week 7 - 7MNT0003 - Policymaking and Nutrition Course
Course Overview
Course Title: Policymaking and Nutrition
Date: 14th November 2025
Instructor: Dr. Kevin Walsh RD FHEA
Learning Objectives
To develop an understanding of nutrition policy history within the UK and other regions, including recent UK regulatory changes (2018-2026).
To describe the policymaking process and policy options in public health nutrition.
To critically discuss current challenges in policymaking in nutrition.
Overview of Key Topics
Timeline and history of nutrition policies in the UK.
Overview of the policymaking process.
Policy options in nutrition.
Challenges in policymaking.
Activity to engage with the material.
A Brief History of Public Health Nutrition
Key Developments
1910, 1930: Vitamin discovery.
1950: Focus on Food Fortification due to rising cardiovascular diseases (CVD).
1990-2010: Establishment of Food Assistance Programs to eliminate hunger, and a debate over energy vs. protein in undernutrition.
Growing focus on dietary patterns, randomized controlled trials (RCTs), and nutrigenomics.
Significant Nutritional Challenges Over Time
Historical focus: Iron, vitamin A, and iodine deficiencies in less wealthy countries.
Rise in chronic diseases and dietary pattern considerations in wealthier nations.
Historical UK (& EU) Perspective
1940s Developments
1940: Formation of Scientific Sub-Committee on Food Policy based on nutritional needs rather than agricultural interests.
Recommended high extraction after pushback from the food/agricultural sector.
Welfare Food Scheme: Aimed at ensuring adequate nutrition during WWII; prioritized pregnant women and children with supplemental food.
Nutrient standards introduced (1940-1941); fortification of margarine (1942) and flour with calcium (1946).
1950s to 1960s Developments
1951-1954: Phasing out of food rationing in the UK.
1956: Shift in food policy from high extraction to nutrient restitution (fortification).
Introduction of EU Common Agricultural Policy (CAP) aimed at agricultural productivity and food supply security.
Tightening of fortification regulations in 1963 for bread, flour, and margarine.
1970s to 1990s Developments
1973: UK joined European Economic Area and CAP.
1978-1979: Government releases healthy eating advice, including salt intake reduction.
1981: Maternity and Welfare Act facilitated low-cost milk for impoverished families.
Launch of the Eat Well Programme (1994) and the Health of the Nation Report (1992), focusing significantly on nutrition.
2000s Developments
2000: Establishment of the Health Development Agency for public health strategy implementation.
2003: Publication of Salt and Health Report by SACN; introduction of food labelling legislation.
2005: National institute for Clinical Excellence (NICE) set up
2006: Low income survey published detailing nutritional status/diet in lower income groups
Policy Milestones (2016-2026)
2016: Implementation of the childhood obesity plan, including soft drinks industry levy and sugar reduction program.
2018: Introduction of the soft drinks industry levy resulting in a 46% average reduction in eligible beverages (2015-2020).
2022: Calorie labelling mandated for large food outlets (250+ employees) and HFSS (high in fat, salt, sugar) placement restrictions introduced.
2025: Ban on HFSS multi-buy promotions.
2026: HFSS advertising restrictions and mandatory folic acid fortification in non-wholemeal flour.
Monitoring & Surveillance of Nutritional Status
Monitoring nutritional status assists with early warning, policy development, and evaluation.
Surveillance focuses on population trends rather than individual risk assessment.
Referenced Source: Tuffrey, V. (2016). “Nutrition surveillance systems: their use and value.”
In the UK, we use NDNS: the National Diet and Nutrition Survey, which provides comprehensive data on the dietary habits and nutrient intake of the population.
Definition of Policy
Definition: A set of ideas or plans agreed upon by a group (government, organization) to achieve a desired goal that benefits society.
Types of Policy:
Proactive: Initiated following party manifesto or aims.
Reactive: Responds to crises or health emergencies.
Current/Live: Relevant and actively discussed in public agendas.
Dormant: Existing but low awareness/enforcement.
Legislative Change
Legalisation = Refers to laws passed through and approved by a legislature like a parliament or congress
Passed laws represent a transformative goal for public health advocacy (i.e., soft drinks industry levy, calorie labelling, HFSS restrictions).
Enactment requires parliamentary debate and scrutiny; must be articulated clearly to the public.
When enacted, benefits from legal apparatus of implementation and enforcement.
The Policymaking Process
Described as a decision-making process, which may not be linear, ideal scenario involves:
Identifying the problem.
Analyzing potential policy solutions.
Engaging stakeholders effectively.
Stakeholder engagement is critical.
Role of public health professionals in the process:
Conducting policy analysis
Communicating findings
Developing partnerships
Promoting and implementing evidence-based interventions.
Problem Identification
Process: Collect, summarize, and interpret data related to the problem (frequency, severity, scope); identify gaps in data.
Define the characteristics (e.g. frequency, severity, scope, economic, and budgetary impacts of the problem
Identify gaps in data
Problems need to be framed to lend themselves to policy solutions.
Determinant Analysis
Identification of factors affecting the problem with a review of their interrelations, recognizing multiple causes.
Identification of causal relationships is important for strategy selection and prioritisation
Understanding both proximate (direct impact) and distal (influence) causes is crucial for effective intervention strategies.
Policy Options in Nutrition
Framework:
People, Products, Promotions, Place, Price: essential components influencing nutritional policy.
Examples:
Reformulation and new product development, e.g., soft drinks industry levy and folic acid fortification.
Stakeholder Engagement
Critical at all policymaking stages:
Identify key stakeholders (decision-makers, affected individuals, community partners).
Assess their characteristics and implement effective communication strategies.
Evaluation of Policy
Essential to systematically assess steps in the policy cycle, including impact and outcomes.
Formulate prioritised evaluation questions to guide the evaluation process.
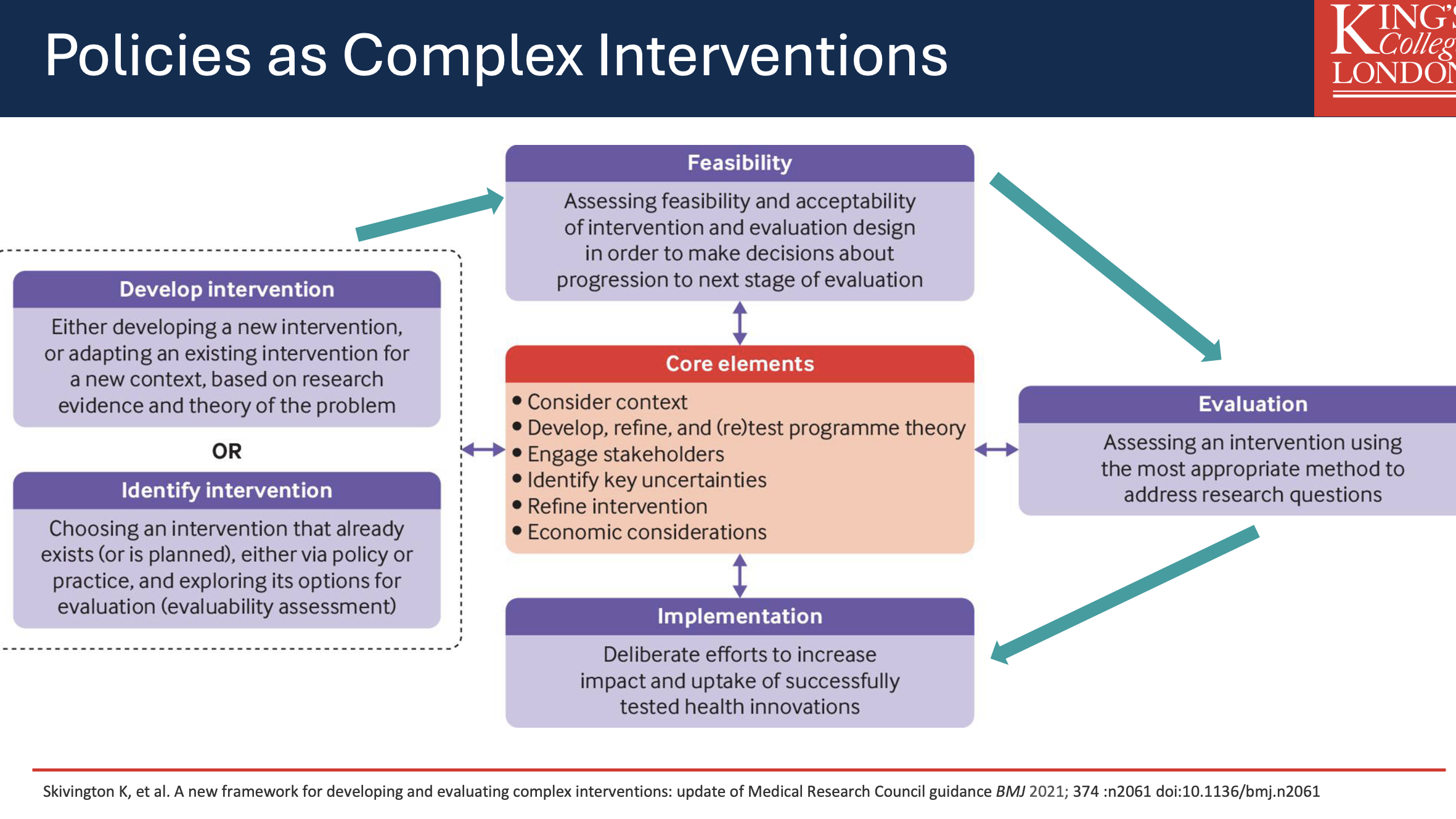
Complex Interventions
Identify or develop intervention
Assess feasibility
Assess intervention and evaluate effectiveness
Implementation of intervention
Policy Options in Nutrition
Products = Reformulation new product developement. e.g soft drinks levy (2018)
Promotions = Advertising and marketing e.g (Ad restrictions on HFSS from 2026)
Place = Buying standards for public procurement, planning policy (HFSS placement restrictions 2022)
Price = taxes or subsidies (SDIL levy, Multi-buy HFFS ban
People = Increase awareness, educate (eatwell guide)
Policy Analysis/Feasibility
Identify different policy options to address the problem/issue and use quantitative and qualitative methods to evaluate and the policy options to determine the most effective, efficient, and feasible option:
Research and identify policy options
Describe:
a)how the policy will impact health/nutrition
b)the costs to implement the policy and how the costs compare with the benefits (economic and budgetary considerations)
c)the political and operational factors associated with adoption and implementation (feasibility)
Assess and prioritise policy options
Always consider the option of doing nothing and assess the impacts compared to ‘active’ policies
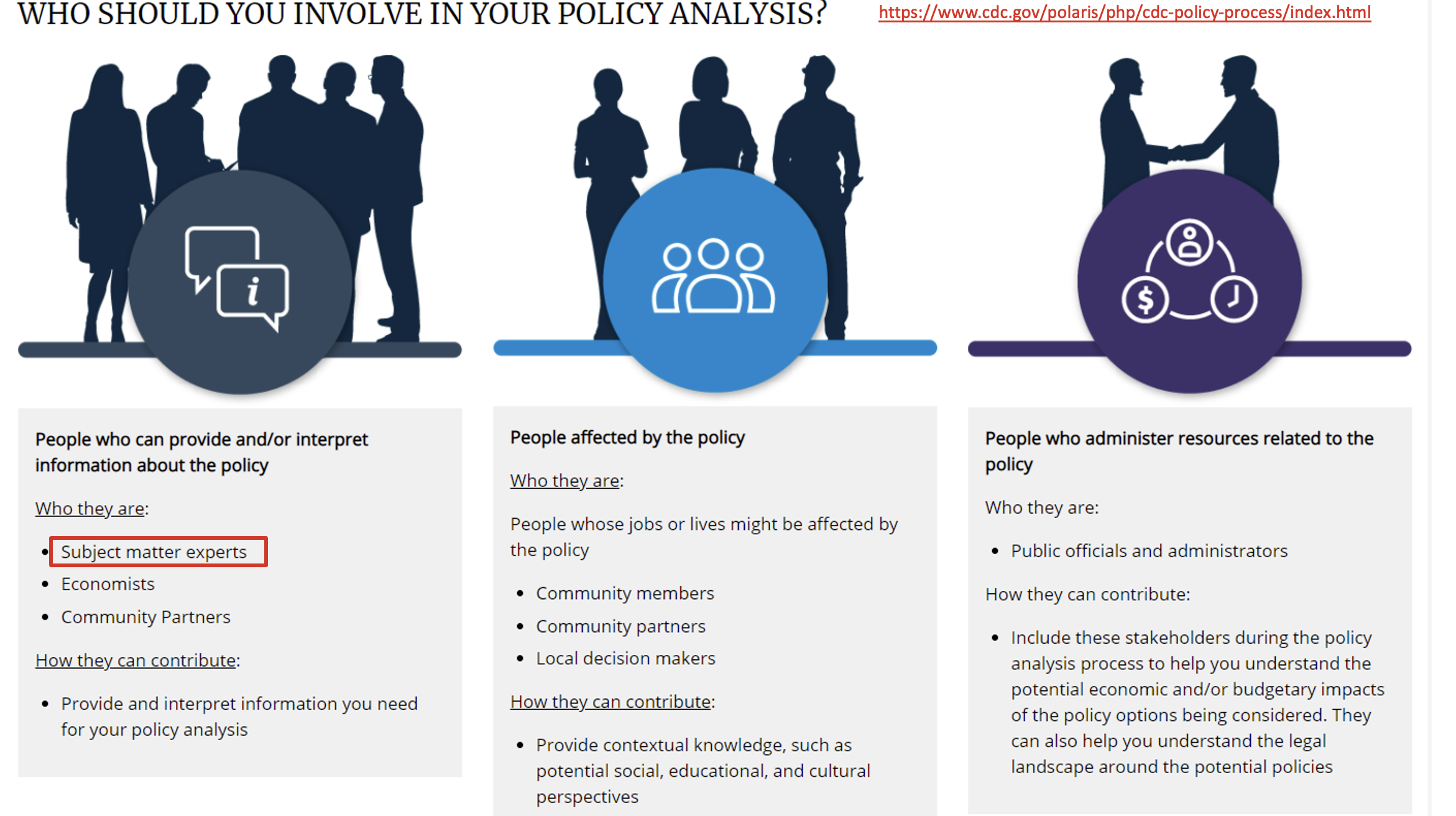
Stakeholder Engagement
Crucial in all stages of policymaking process
Involves identifying and connecting with decision-makers, partners, those affected by the policy, and the general public:
Identify key stakeholders, including supporters and opponents (e.g., community members, decision-makers, nonprofit, and for-profit agencies)
Assess relevant characteristics (e.g., knowledge, attitudes, needs)
Implement communication strategies and deliver relevant messages and materials
Solicit input and gather feedback
Strategy and policy developement and enactment
Identify the strategy for the policy and how the policy will operate
Identify how the policy will operate and what is needed for policy enactment and implementation (e.g., understand jurisdictional context and identify information and capacity needs)
Define strategy for engaging stakeholders and policy actors
Possibly draft the policy (law, regulation, procedures, actions, etc.)
Policy Enactment:
Follow internal or external procedures for getting policy enacted or passed
Enact law, regulation, procedure, administrative action, incentive, or voluntary practice
Policy Implementation
Translate the enacted policy into action, monitor uptake, and ensure full implementation:
Translate policy into operational practice and define implementation standards
Implement regulations, guidelines, recommendations, directives and organisational policies
Identify indicators and metrics to evaluate implementation and impact of the policy
Coordinate resources and build capacity of personnel to implement policy
Assess implementation and ensure compliance with policy
Support post-implementation sustainability of policy
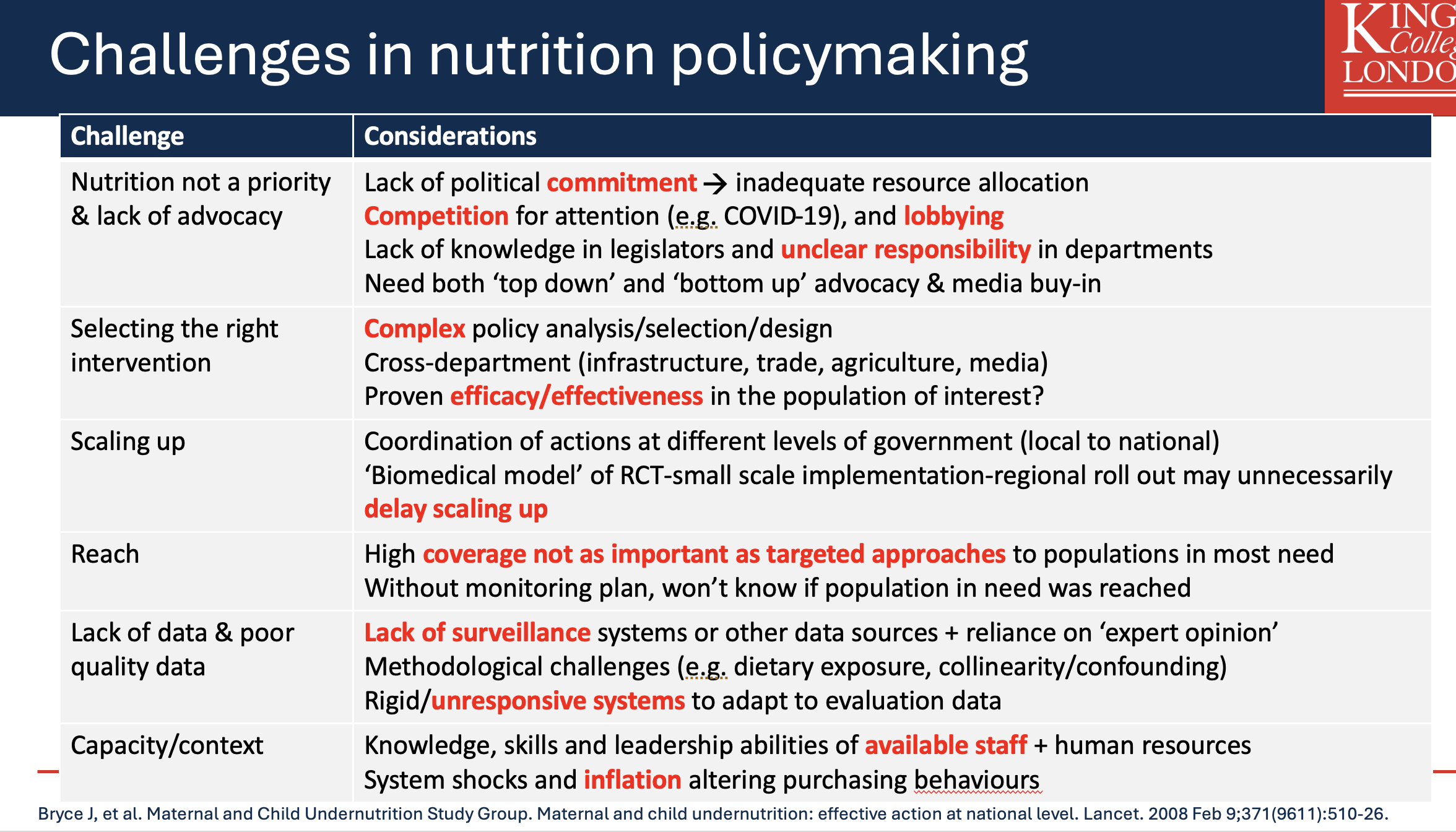
Challenges in Nutrition Policymaking
Common Challenges:
Lack of political commitment, competition for attention, unclear legislative responsibilities, complexity in policy design.
Data gaps leading to poor decision-making and lack of robust surveillance systems.
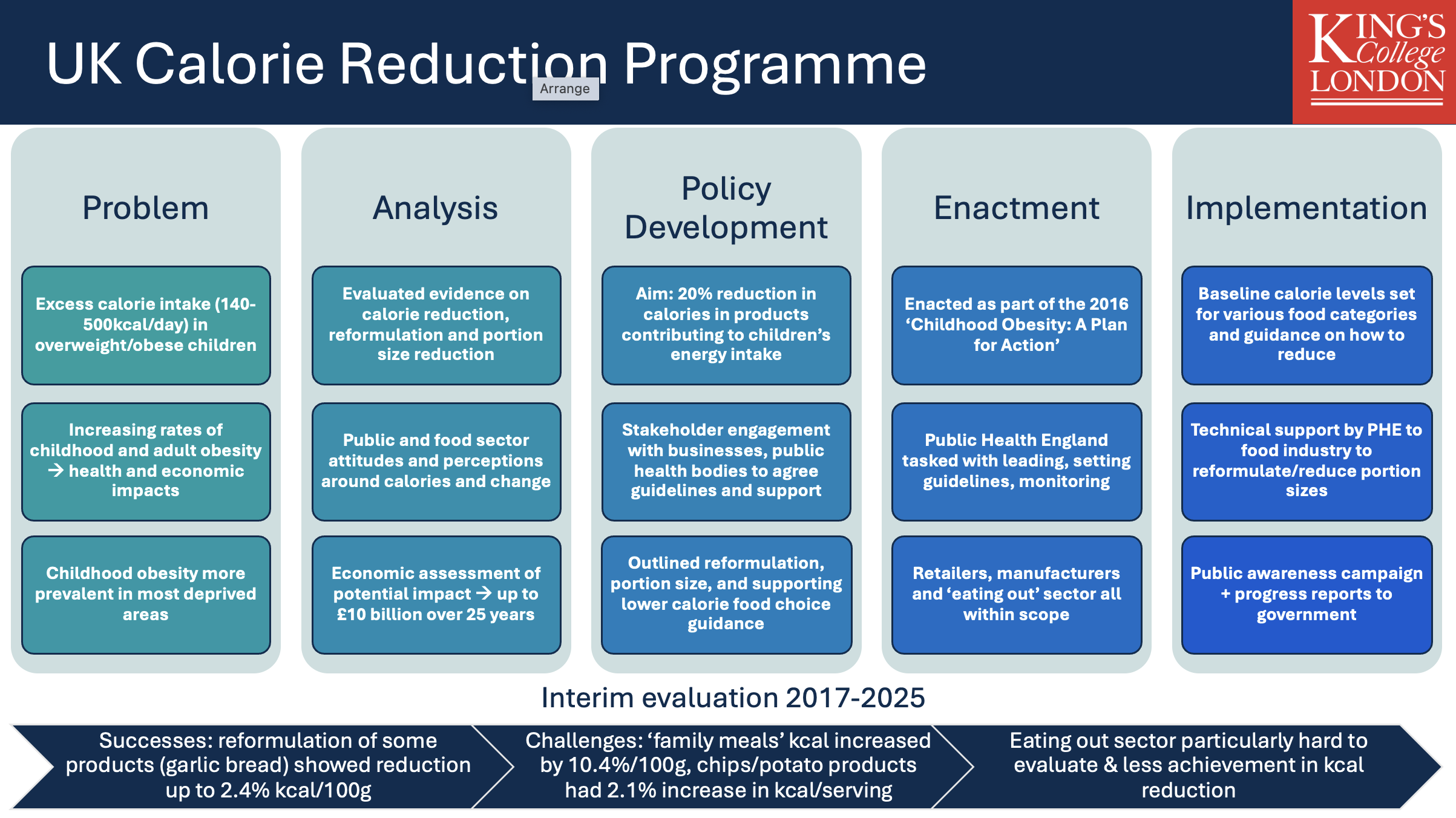
Case Study: UK Calorie Reduction Programme
Problem: Excessive calorie intake among children.
Policy Aim: Achieve a 20% reduction in calories from specific food categories through stakeholder engagement and public awareness campaigns.
Challenges: Evaluation difficulties for the eating out sector; mixed success regarding calorie reduction initiatives.
Key Takeaways
Importance of continuous advocacy and evidence-based policymaking in public health nutrition.
Understanding the complexities and necessity of cross-sector collaboration is vital for effective policymaking.
An understanding of what policy is and the different types of policies/policy actors.
UK policy momentum since 2016 includes Soft Drinks Industry Levy (2018), HFSS placement (2022), calorie labelling (2022), HFSS multibuy (2025), HFSS ad restrictions (inc. 2026), and folic acid flour fortification (inc. 2026)
The policymaking process: key stages and what they involve
The many challenges involved when making nutrition policy
Cross-sectoral, multi-disciplinary working is key, but difficult. Buy-in from commercial/industry partners is important.
Importance of public health nutrition needs to be recognised – need continuous advocacy
Need for policymaking to be grounded in evidence, but data gaps/limitations of evidence can make this difficult
Contact Information
Instructor: Dr. Kevin Walsh RD FHEA
Contact: +44 (0)20 7848 4437 | kevin.walsh@kcl.ac.uk