acquired cardiac
PEDIATRIC ACQUIRED CARDIAC DISORDERS (NUR 430 FA2024)
ASPIRIN USE IN CHILDREN
Aspirin linked to Reye's syndrome when given to children with fever & viral illnesses (e.g., viral influenza, varicella).
Reye's syndrome: Very rare multi-organ failure leading to cerebral and hepatic edema; can result in increased intracranial pressure (ICP), brain damage, or death.
Recommendation: Avoid aspirin in children aged 18 or younger for fever/illness.
Exceptions: Cardiac process. Aspirin is safe and ideal for cardiac conditions, such as Kawasaki Disease.
RHEUMATIC FEVER (RF) AND RHEUMATIC HEART DISEASE
Overview
Cause: Untreated or incompletely treated group A beta-strep infection, most common in ages 5-15.
It can originate from strep throat or impetigo infection.
Definition: Autoimmune reaction to group a strep infection affecting heart valves, joints, brain, and skin due to immune response, not the bacteria itself. *crucial concept *
Complication: Rheumatic heart disease is a complication of RF as heart valves can get damaged. (about 60% of kids w/ RF develop heart problems)
Inflammation & damage to valves can cause HF at some point in life
Nursing Implication: Stress importance of adherence to antibiotic treatment for strep to prevent RF and antibiotic-resistant bacteria
DIAGNOSIS BASED ON JONES CRITERIA
Jones Criteria:
Evidence of current or recent strep infection + 2 or more major signs & echo abnormal OR
Evidence of current or recent strep infection + one major sign & one or more minor signs & echo abnormal
CAN’T HAVE RF IF YOU HAVEN’T HAD A RECENT STREP INFECTION (throat cultures growing GABHS or elevated anti-streptolysin O titers
Major Signs: Joint involvement (migratory polyarthritis); myocarditis; subcut nodules (painless, over bony prominences & flexor tendons), erythema marginatum, Sydenham chorea
Minor Signs: CRP increase, arthralgia, fever, elevated ESR, prolonged PR interval, anamnesis of rheumatism, leukocytosis
Other symptoms: fever, joint pain, elevated inflammatory markers, murmur, chorea, EKG changes (tachycardia, AV block)
CLINICAL MANAGEMENT
Medications:
Antibiotics to eradicate strep if still present. (penicillin, erythromycin, sulfadiazine)
NSAIDs OR aspirin therapy 2x day for 2-8 week course
Potential steroids for severe heart inflammation causing CHF
Management Strategies:
Frequent cardiac assessments (esp if a new murmur develops); bedrest crucial for heart muscle recovery; periodic echocardiograms to check for valve damage. (valve damage = RH disease) WORST case scenario; may need a valve replacement. Now becomes RHD.
Nursing Care: Pain control (NSAIDs); provide abx (if strep still present); Passive ROM to not elevate HR; provide rest (quiet activities. 4-6 months bedrest w/ recovery)
psychosocial support especially for complications like Sydenham's chorea, an affect of the anti strep antibodies in brain
Sydenham’s-movement disorder (uncontrollable, jerky, purposeless movements of hands, feet, shoulders, legs, trunk)
At risk for PANDAS: Pediatric Autoimmune Neuropsychiatric
Disorders Associated with Strep infection
ANTIBIOTIC PROPHYLAXIS
We want to keep these kids from getting strep infections again (shown they have a bad autoimmune response to strep)
DAILY oral penicillin BID or IM monthly penicillin or sulfadiazine once daily
If a break through strep infection occurs, they will need tx doses of abx
CDC Guidelines: Recommended daily prophylaxis in children who had RF until age 21 or 5 years post-diagnosis (ATI); additional antibiotics required prior to dental procedures if heart valve disease develops. (to prevent bacterial infection endocarditis)
RF & RHD key points:
Autoimmune, inflammatory reaction to a group A beta -streptococcus infection
Can be prevented by fully treating streptococcal infection with antibiotics.
Manifestations: chorea, arthralgia, fever, carditis, erythema marginatum, subcutaneous nodules, polyarthritis, and elevated C-reactive proteins.
WORSE CASE WITH CARDITIS IS VALVE DAMAGE = Rheumatic Heart Disease
Diagnosed using Jones criteria and Echocardiogram
Care: Antibiotics and anti-inflammatory medications, pain control, rest
Long term daily antibiotic prophylaxis to prevent strep infections (penicillin 2xday or IM monthly or sulfadiazine daily) These kids reacted badly to strep. Do not want them to get it again.
Get culture of sore throats (need treatment dose of antibiotics and/or alternate antibiotic if strep returns)
Risk of Rheumatic heart disease: Valve replacement in future. If develop RH disease with valve damage, will need additional antibiotic prophylaxis for dental procedures in addition to daily antibiotics to prevent strep. But only if develop valve disease. WHY? At risk for infective endocarditis
KAWASAKI DISEASE
Overview
Definition: Acute, febrile illness causing systemic vascular inflammation of small and mid-sized arteries, especially coronary arteries.
#1 cause of ACQUIRED heart disease in kids in the US. (RF #1 globally)
Demographics: Most prevalent in children under 5 years (80%); higher incidence in males (Male: Female ratio 1.5:1) and certain ethnic groups (Asian, Pacific Islanders).
Cause: Unknown but linked to exaggerated immune response in susceptible children.
MANIFESTATIONS & COURSE: 3 STAGES
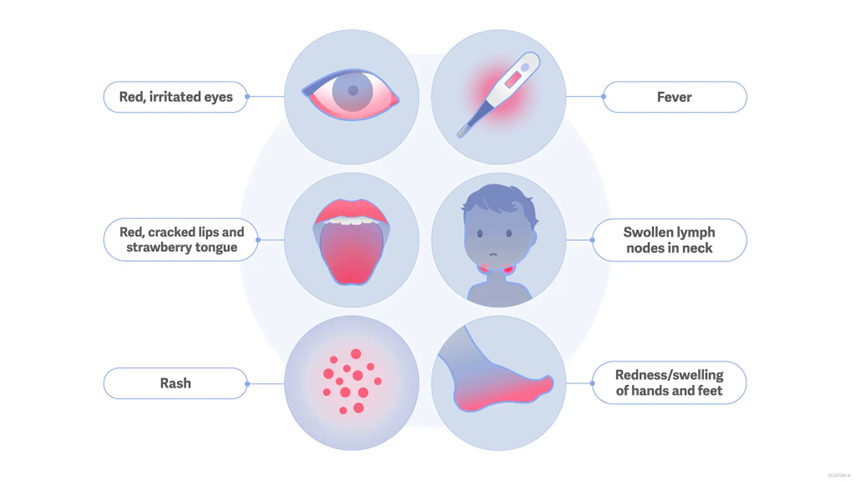
Acute Phase (1-2 weeks): High fever for at least 5 days (diagnostic), hyperemic conjunctiva, red throat, swollen hands and feet, rash, strawberry tongue & cracked lips, cervical lymph node enlargement ~hydration is key~
Treatment goal: lower fever, inflammation & prevent cardiac issues
Intravenous Immunoglobulin (IVIG) 2 grams/kg specifically helps prevent coronary artery damage. Second dose if fever returns within 36 hours of first infusion.
High-dose aspirin given, then low-dose aspirin in later stages until platelet count normal. Longer course if artery damage occurs.
This disorder is the Exception to the “no aspirin rule” in sick children
We are not sure what causes Kawasaki, but we know it is not a flu virus, so aspirin is ok. (Might be a SARs associated coronavirus)
IVIG nursing considerations:
Premeds:
Assessments:
Titration:
Side Effects:
Given IV infusion (can also be given at home SQ infusion for other diagnoses)
(Live vaccines- MMR & Varicella should be delayed 7-12 months after IVIG infusion when given for a short term.
Nursing interventions:
Fever management: frequent linen changes, hydration, comfort measures
Comfort care: soft foods, liquids, not too hot or too cold in acute and subacute phases. Tongue hurts! IVIG high dose side effects
Monitor for development of acute cardiac problems (myocarditis, LV dysfunction, arrhythmias)
Medication & home management teaching, emphasizing long term cardiac follow up needed for coronary artery aneurysm risk. Teaching: rest
Subacute Phase (2-4 weeks): Symptoms may include diarrhea, hepatic dysfunction (elevated liver enzymes), desquamation of fingers/toes, and cardiac disease manifestations.
Includes coronary artery inflammation & then aneurysm, myocarditis, impaired LV function, valve regurg, arrhythmias, pericardial effusions. THIS IS WHAT WE’RE TRYING TO PRESENT. Worst case scenario.
Thrombocytosis= increase # of platelets
Convalescent Phase (6-8 weeks from onset): Need rest. Children may appear normal but require cardiology follow-up due to potential ongoing heart issues.
Considerations
Monitor for cardiac coronary artery aneurysms for several months
Limit strenuous activities in kids w/ aneurysms. Of these, 2/3 resolve, 1/3 may need angioplasty or bypass graft if left with stenosis after the aneurysms heal.
Kawasaki Key Points
Acute, systemic vascular inflammatory disorder
Unknown cause
Usually occurs in kids 5 & younger
Most common cause of acquired heart disease in US
3 phases- acute (abrupt fever), subacute (fever resolution) & convalescent (complete resolution)
Manifestations: fever, strawberry tongue, rash, conjunctivitis, erythema of hands & feet, cervical lymphadenopathy & desquamation of fingers & toes
Last several weeks, but convalescent can take 3 months
Coronary aneurysms may occur. This is what we want to avoid
Treat w/ IVIG therapy & aspirin
NEW: COVID MULTI-SYSTEM INFLAMMATORY SYNDROME= VERY SIMILAR TO KAWASAKI
But seems to affects kids greater than 5 years old
Affects heart in greater percentages than Kawasaki (myocarditis mainly)
80% needed high support in ICU, most survived. 2% died and had underlying health issues.
Treatment:
IVIG (like Kawasaki)
Steroids
Immune modulators: tocilizumab, siltuximab
Exercise & sports limited until follow-up w/ cardio
ARRHYTHMIAS
Supraventricular Tachycardia (SVT)
Defined as heart rate over 220 bpm in infants and over 180 in children.
Symptoms: (stable or unstable) Infants: poor feeding, pallor, irritability. Kids: SOB, syncope, dizziness, chest pain, pallor, sweating. Untreated can lead to CHF or cardiogenic shock.
Treatment: Vagal maneuvers, adenosine, beta-blockers, amiodarone, procainamide.
Cardioversion if meds fail
Ablation of accessory conduction pathway is a permanent fix (usually). Nursing care post-ablation: like a cardiac cath
Ice to face!!
Cardiac Injuries Commotio Cordis
Leading cause of sudden cardiac death in young athletes
Refers to sudden cardiac death due to a blunt, non-penetrating blow to the chest during a critical stage of the cardiac cycle causing Vfib & sudden death. Wrong place wrong time in cardiac cycle.
Prevention: Keeping kids safe on the sports field-59% chance survival rate. School and sports safety practices; ensure coaches and teachers are trained in CPR and AED use.
AED quickly available
Kids to have protective equipment in use
CPR FOR INFANTS AND CHILDREN
Remember certification techniques for proper chest compressions, depth, and rate to ensure effective resuscitation.