WK 2 Pelvis, hip and femur
Pelvis and Hip
Pelvis
Bones
3 bones make up the pelvis: ilium, ischium and pubic - all fuse
Acetabulum formed by the fusion of the 3 bones - deep articular surface and obturator foramen lays inferior to it
Joints: sacroiliac joint and pubic symphysis
Pelvic cavities
Pelvic brim: horizontal plane that passes from the sacral promontory to the upper margin of the pubic symphysis
Greater pelvis (false): holds abdominal organs
Lesser pelvis (true): holds pelvic organs
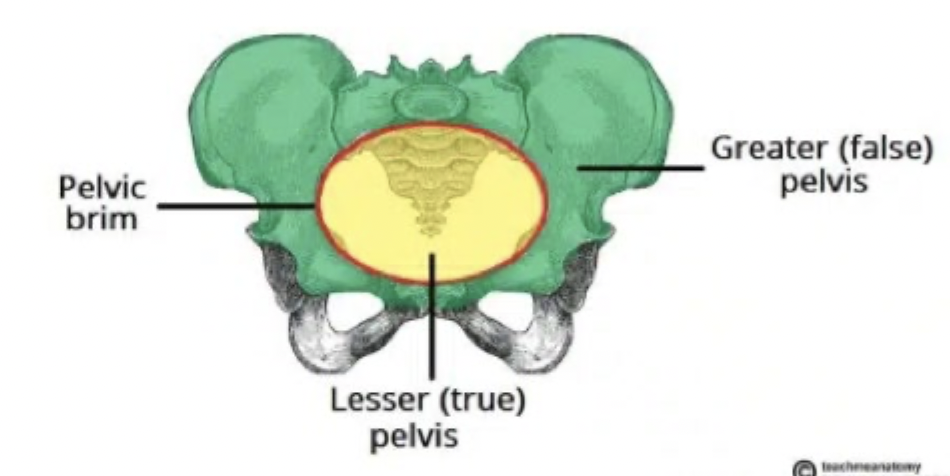
Pelvic inlet: superior circumference of the true pelvis and pelvic brim (has specific views as it is curved)
Pelvic outlet: inferior circumference of the true pelvis formed by the pubic arch
Boundaries:
Anterior: rami of ischium and pubis and lower margin of symphysis pubis
Posterior: coccyx
Lateral; ischial spines and ischial tuberosities
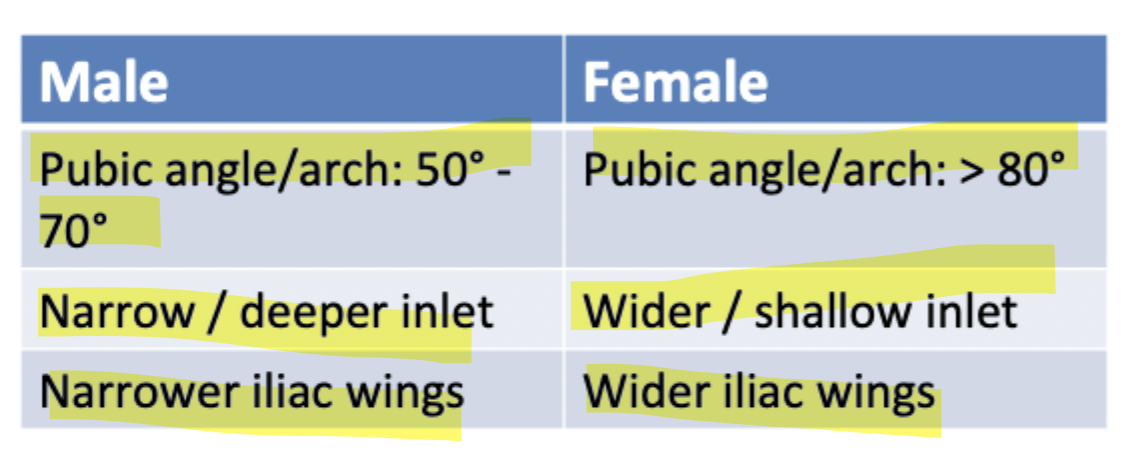
Gender differences in the pelvis
Radiography of the pelvis
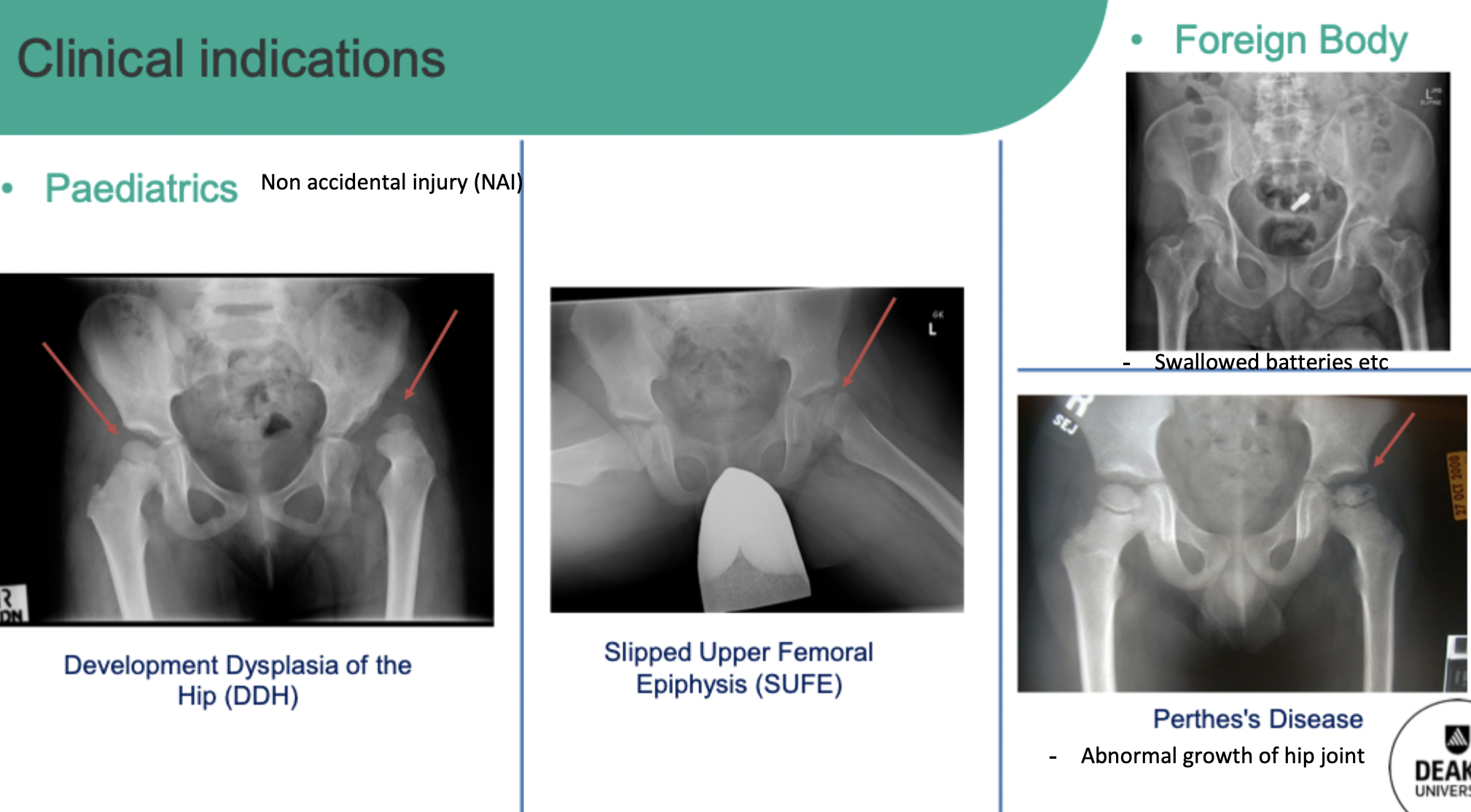
Clinical indications
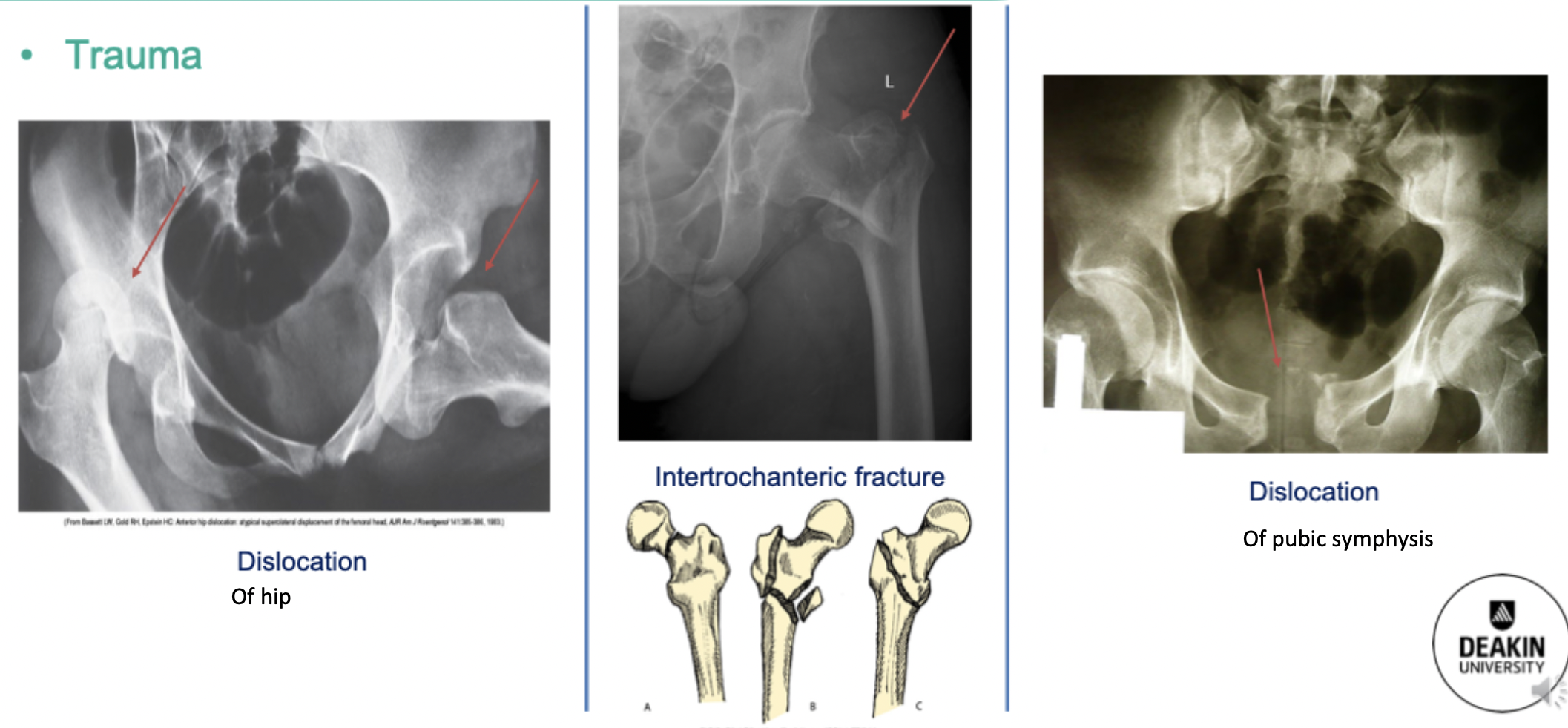
Trauma
Dislocation of the hip - tendons an ligaments spasming and pinching - painful
Pubic symphysis dislocation
Intertrochanteric fracture: fracture between greater and lesser trochanters
Projections:
Standard: AP - normally comes with hip referral too
Modified: AP charnley - includes more of femoral shaft - for prosthetic devices and total hip replacements
Additional views
Oblique: for the ilium
Judet: obliques for the acetabulum
AP axial inlet and outlet views: for pubic rami, ischium and pubic symphysis
Parameters for all pelvic views
Use grid
Broad focus
SID: 100cm
kVp: 75-85
mAs: 15-40 - average patient is 25
AEC: 2 lateral chambers
Breathing: suspended respiration
Gonadal shielding for females - dependent on clinical indications eg. 35 yr old female follow up x-ray
Greater trochanter is in the same line as the pubic symphysis
Positioning
AP pelvis:
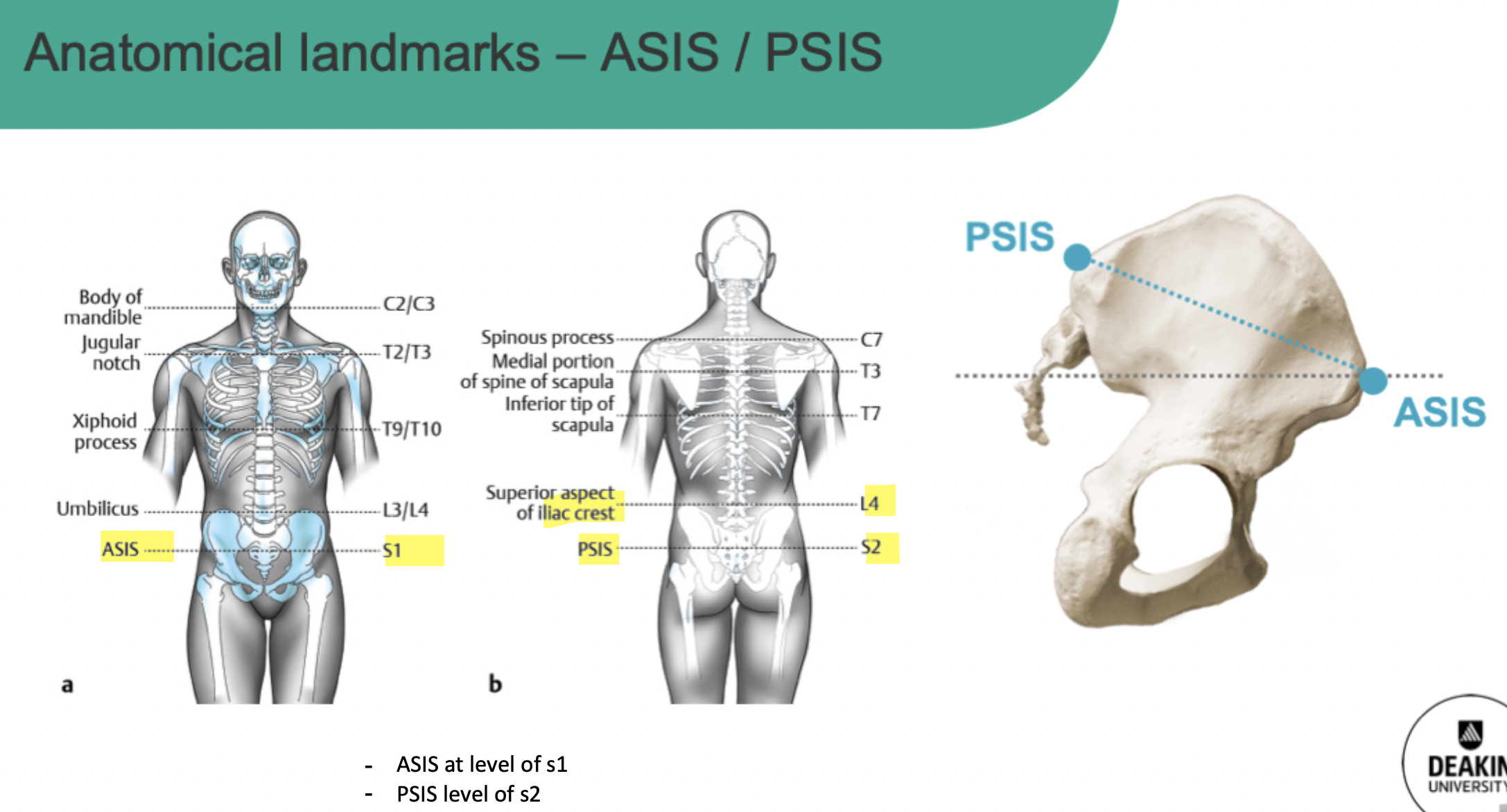
ASIS equidistant from the IR
Internal rotation of legs 15-20 degrees
CR - 5cm above pubic symphysis or midway between ASIS and pubic symphysis
Collimate to include iliac crests and pubic symphysis with greater troch
Assessment criteria:
iliac crest levels the same - tilt
Shape of ilium equal on both sides - if one is wider it is rotated towards that side
Obturator foramen size equal - side that is narrower is the direction of rotation
Sacrum and coccyx midline with pubic symphysis - if rotated to one side the pelvis is rotated in the opposite direction (sacrum and coccyx visualised towards the left = right rotation)
Internal rotation of the femur so the GT is in profile and LT is superimposed
Trabecular bony patterns
AP Charnley:
Align ASIS to upper collimation field - captures full length of prosthetic device
Same assessment criteria
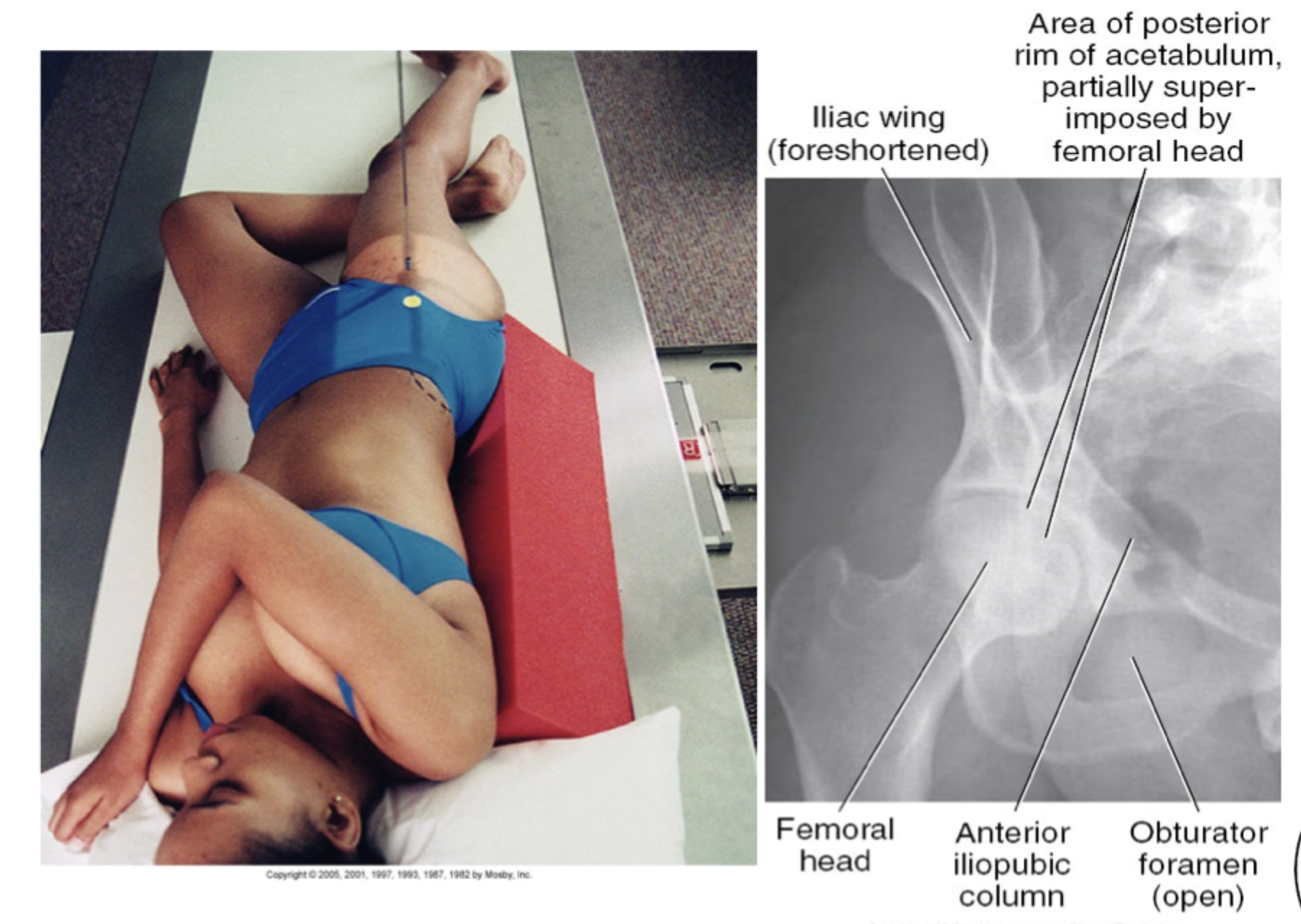
Judet method: right or left acetabulum - two views of the same side
Projection 1: unaffected side raised 45 degrees, collimate to affected acetabulum and CR 5cm distal and medial from ASIS
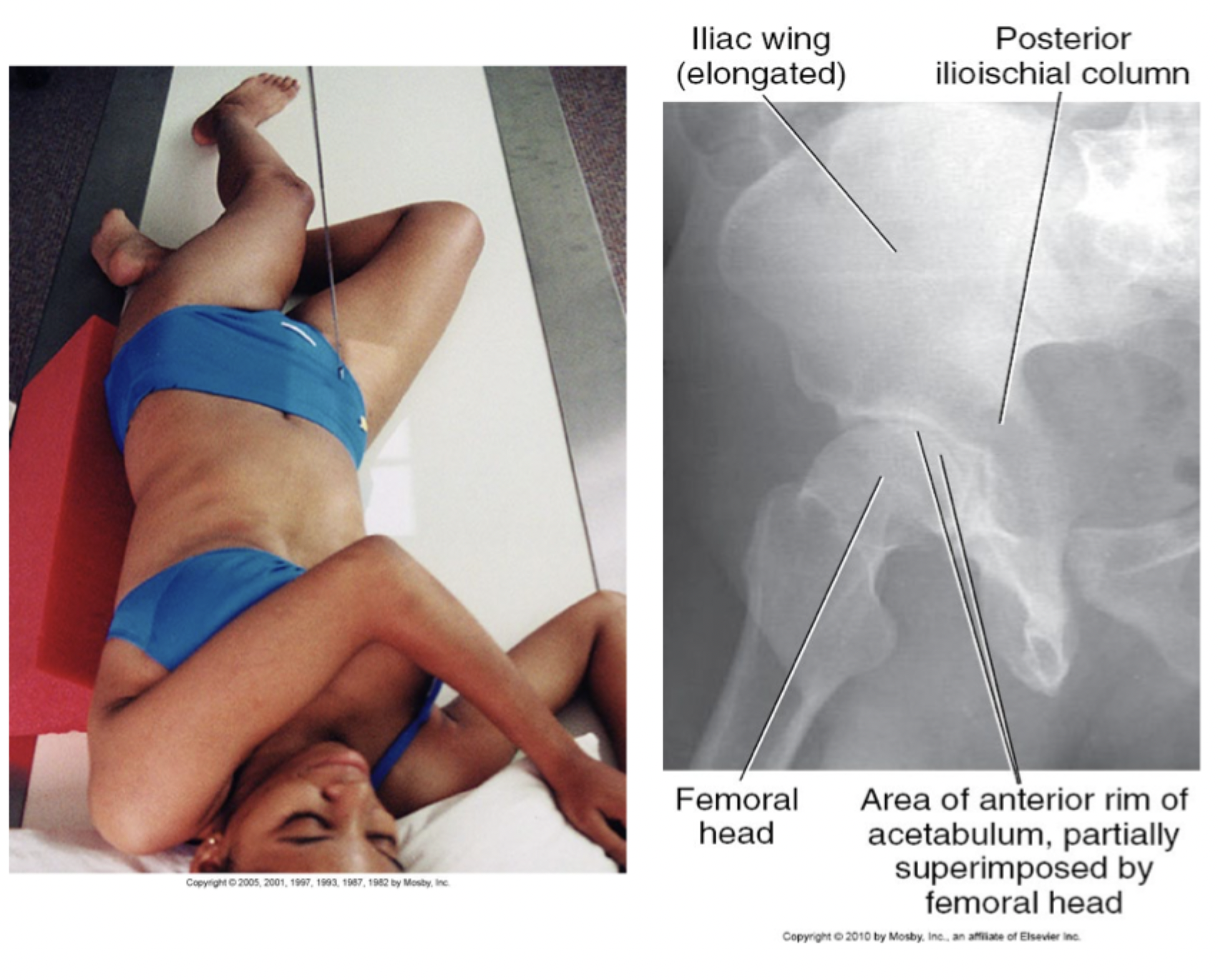
Projection 2: affected side raised 45 degrees, collimate to affected acetabulum and CR 5cm distal and medial from ASIS
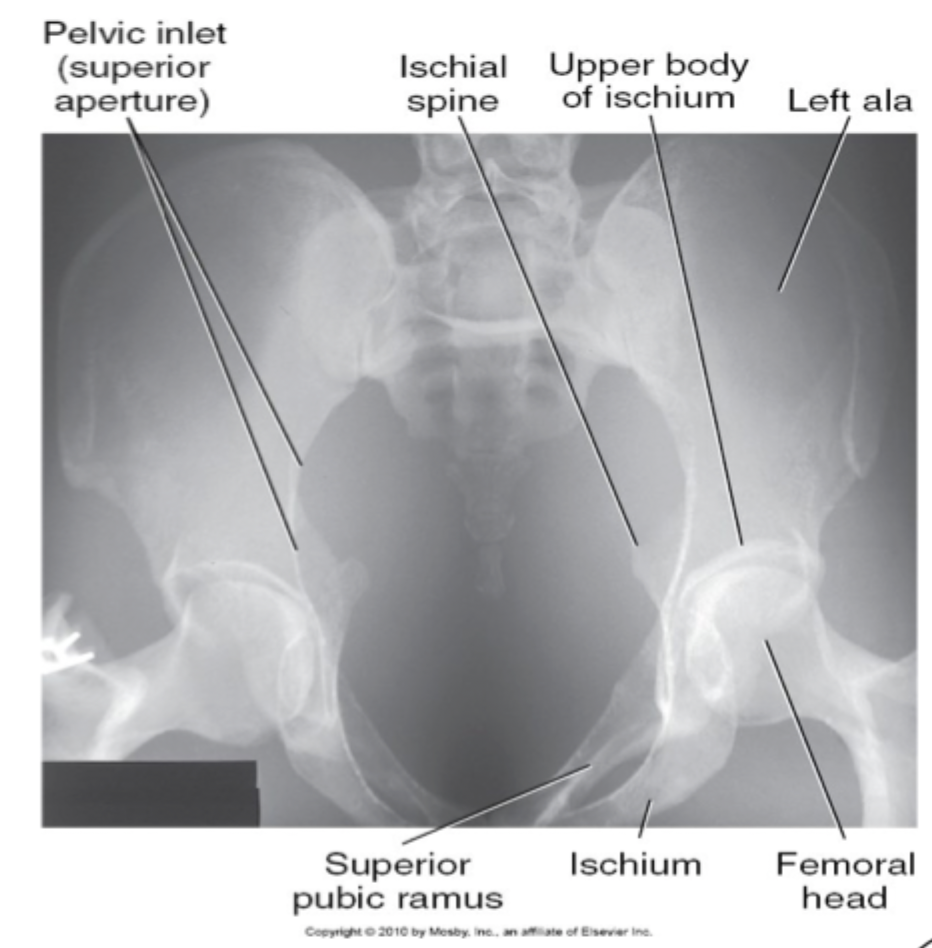
AP Axial inlet:
Patient supine AP position
Tube angled 40 degrees caudally
CR midway between ASIS
If patient is unable to be fully supine - increase angle to open up pelvic inlet
AP Axial outlet:
Patient supine AP position
Tube angled 20-35 degrees (males) and 30-45 degrees (females) cranially
CR at level of greater troch - midline
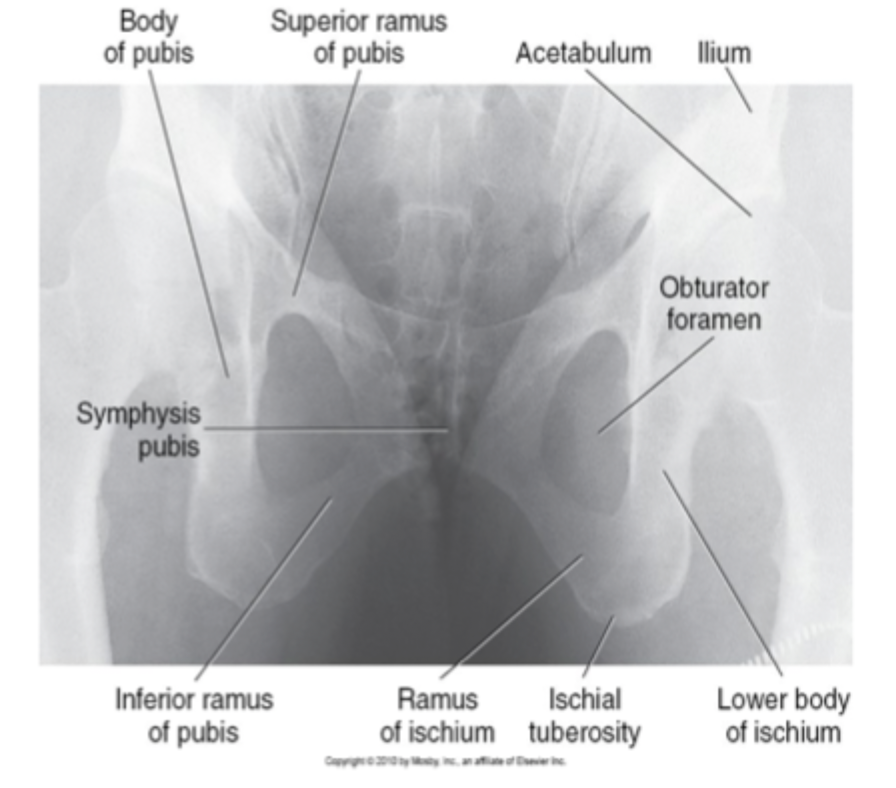
AP axial inlet and outlet views can help with pubic ramus fractures
Hip/Proximal femur
femoral neck fracture common
Angle of inclination - angle of head of femur to the femoral shaft - 110-140 degrees
Angle of inclination changes with age and length of femur
Hip in anatomical position: GT and LT in profile and femoral neck is foreshortened
To counteract: internal rotation 15-20 degrees - elongate NOF and LT superimposed with shaft
Radiography of the hip
Clinical indications
Same of pelvis
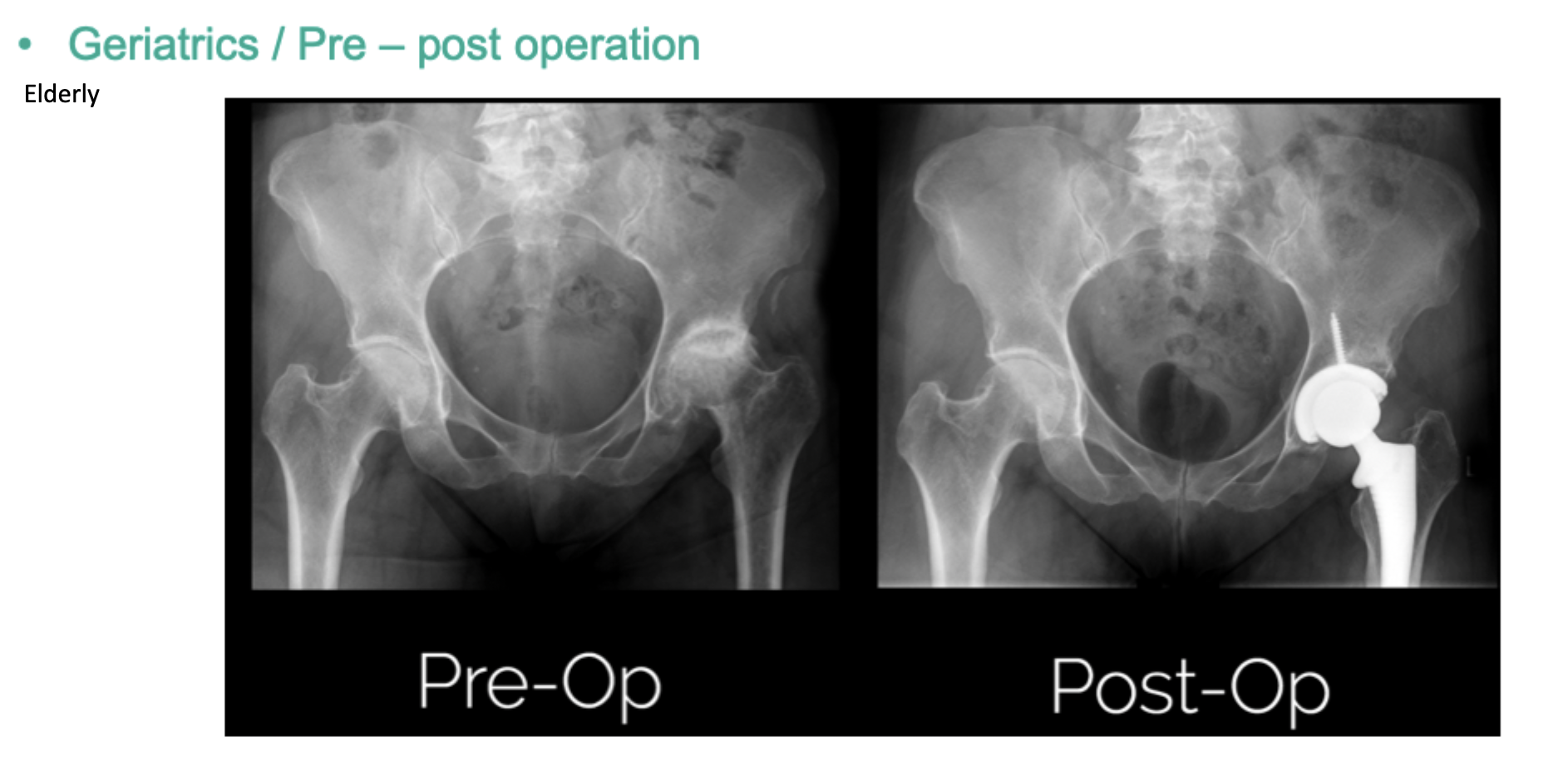
Surgical assessment (pre-op, templating and mag-marker) eg. THR
Osteoarthritis
Projections
Standard
AP unilateral/bilateral hips (AP pelvis/charnley)
Lateral hip:
Medio-lateral obliques (unilateral): Rotating hip from medial to lateral side - projection is lateral, position is oblique hip - rotating hip not body
Frog leg bilateral - paediatric
Axiolateral horibeam
Clements- Nakayama - when unable to move patients
Parameters for AP Hip and Lateral
Use grid
Broad focus
SID: 100cm
kVp: 75-85
mAs: 25-50 - average patient is 25
AEC: middle chamber
Parameters for Axiolateral hip/Clements-Nakayama (Horibeam will wall bucky or free detector)
Use grid
Broad focus
SID: 100cm
kVp: 80-100
mAs: 80-100 - average patient is 80 (use less if it is free detector)
AEC: middle chamber
Patient prep
try to do in bed if possible
do not forcefully internally rotate - cut femoral artery = no supply to lower limb
NOF presents as foreshortened leg and externally rotated
Positioning
AP hip unilateral:
Supine
CR over femoral neck - CR at greater troch or at the level of PB upper margin
Internally rotate
Mediolateral hip:
Flex knee to rotate affected leg 45 degrees so the foot is touching the other knee
CR at femoral neck
NOF partially superimposed with GT
Good visualisation of hip joint, acetabulum and head of femur
OR rotation of the pelvis to 60-75 degrees with femur abducted - NOF foreshortened but can see head an acetabulum
Frog leg lateral - bilateral
Flex hips and knees so that soles of feet touching
Paediatric
Axiolateral hip
in trauma
unaffected limb raised so beam can shoot through femoral neck - crease
IR parallel to femoral neck
Clements-nakayama
when patient cannot move either leg
on very edge of bed with IR lowered down - try not to shoot through bed
Caudal angle of 15-20 degrees from horizontal position
CR at NOF
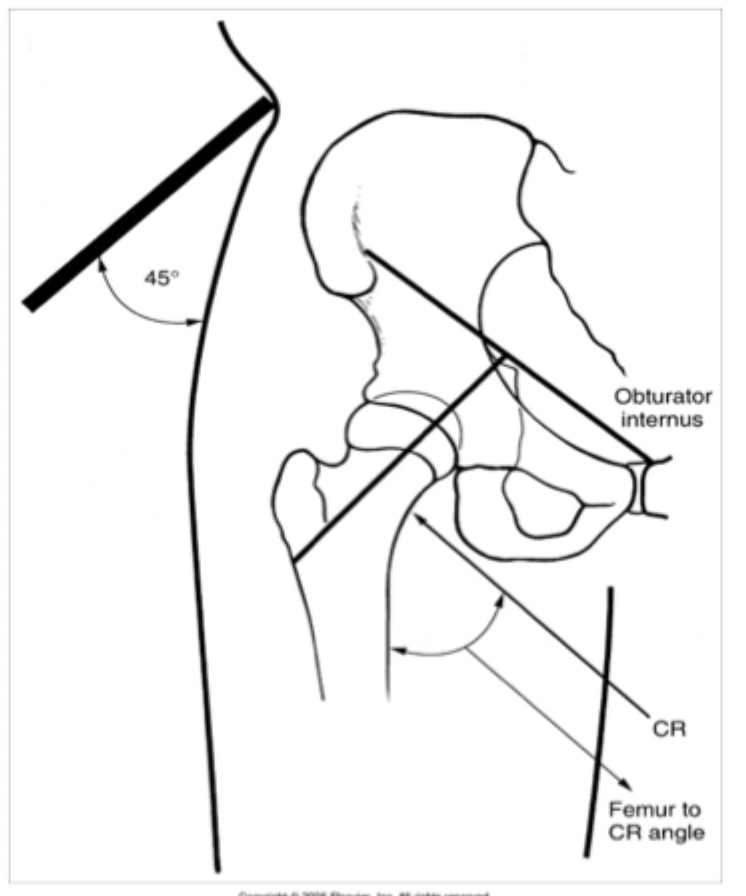
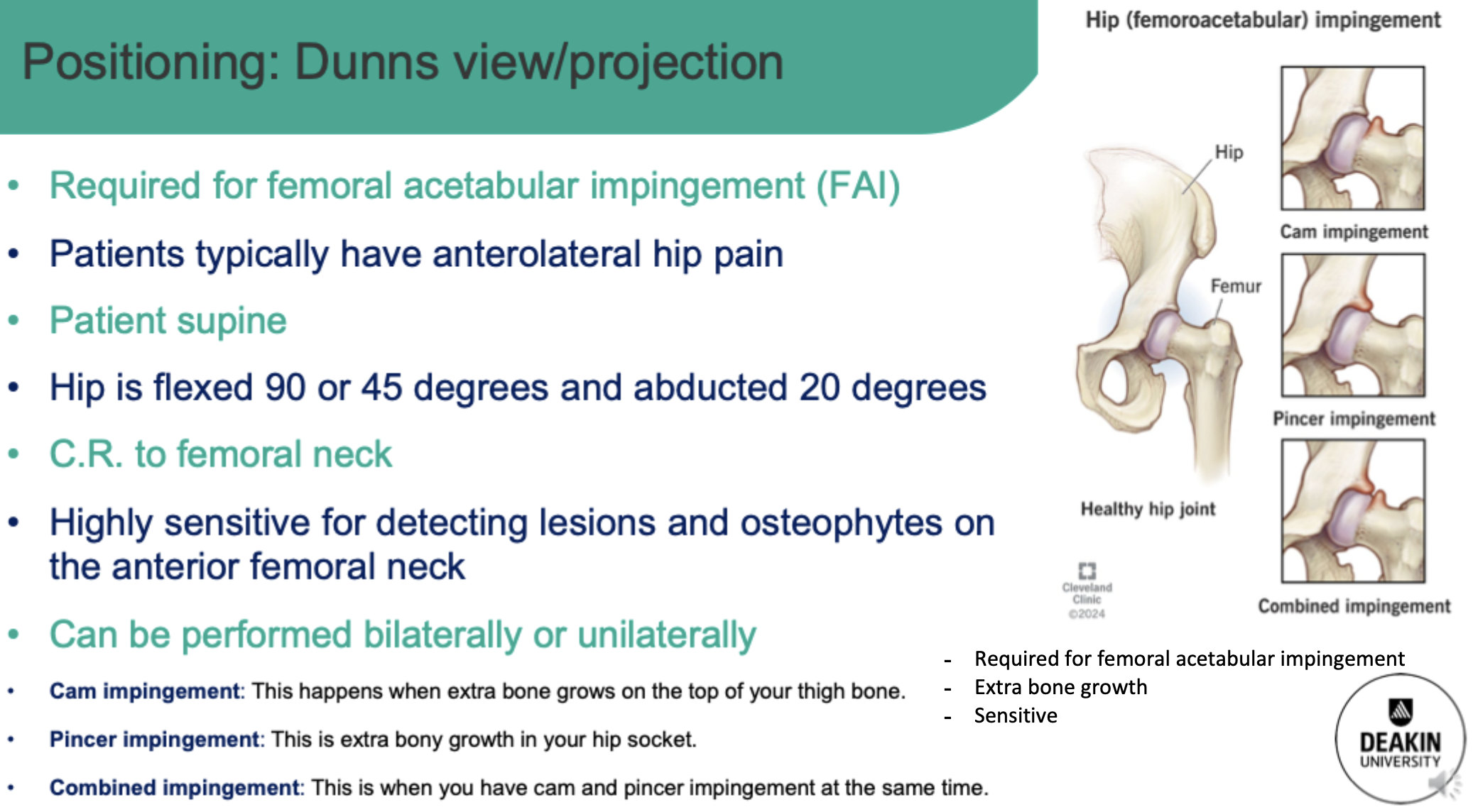
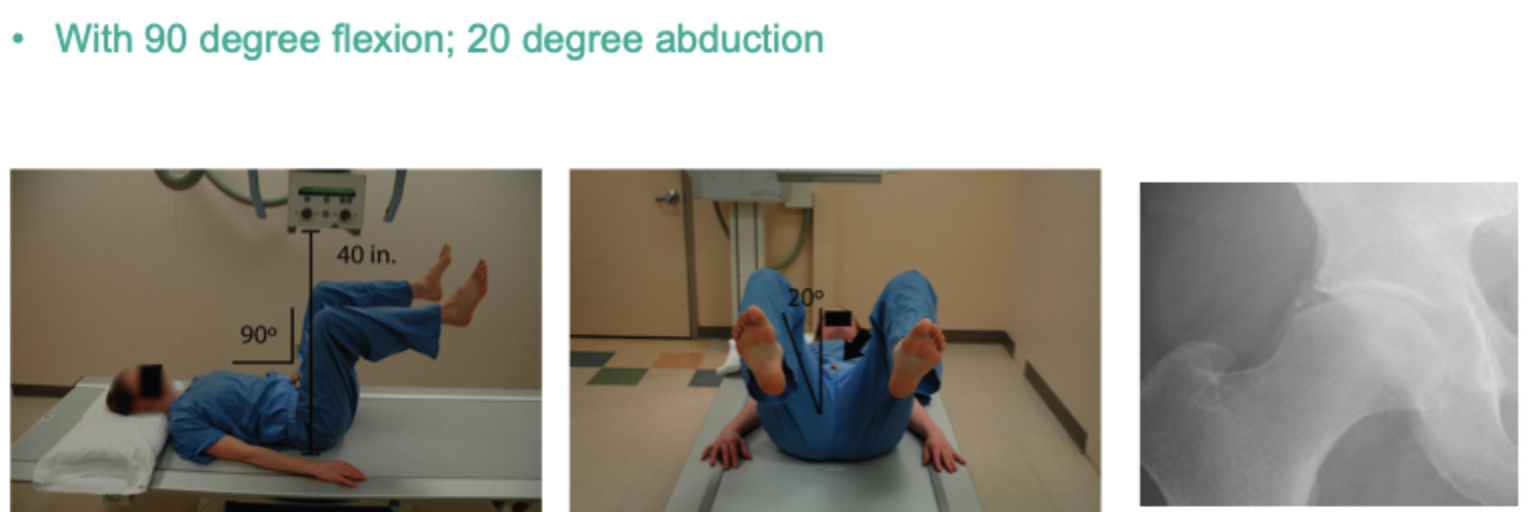
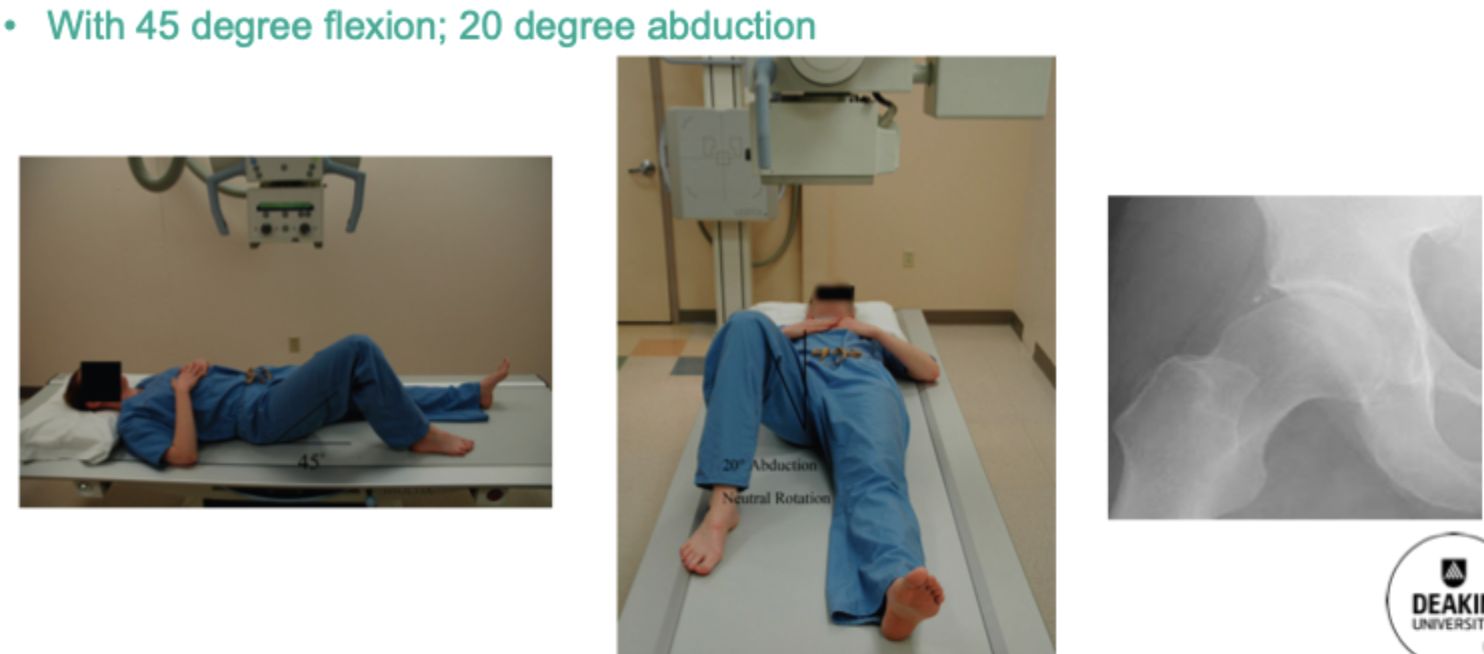
Dunns
Radiography of the femur
Clinical indications same as pelvis and hip
Patient care for trauma - limited movement
Projections
Standard
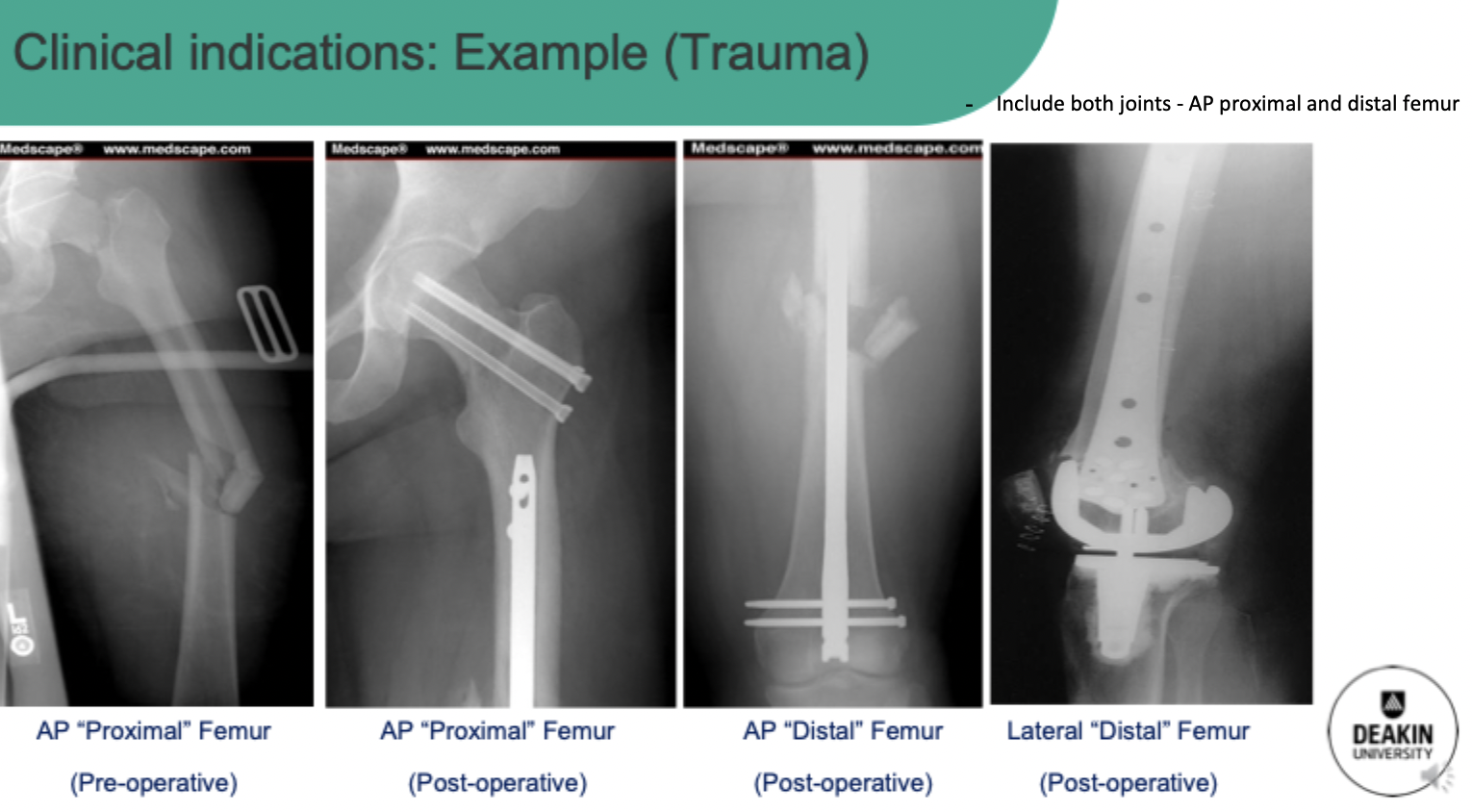
AP proximal (same has hip) and distal (same as knee) femur to include prosthetic device and both hip joint and knee joint
Lateral femur
Medio-lateral obliques - similar to hip
Lateral distal - similar to knee - CR over the knee joint
Axiolateral - horibeam proximal and distal (cr over knee joint)
Parameters
use grid
Broad focus
100cm SID
kVp: 70-80 (if out of bucky for distal femur use knee exposures - 60-70)
mAs: 25-40 or 50-100 (horibeam or large patient)
AEC middle chamber
Positioning
AP femur proximal and distal:
supine
leg internally rotated
CR mid femur with ASIS upper border of collimation (proximal) OR CR lower third of femur with knee joint included (distal)
Lateral femur (proximal):
abduct 60 degrees - move body to achieve lateral femur
Mediolateral hip to include shaft of femur
OR axiolateral HB of hip to include shaft of femur (trauma)
Lateral femur (distal):
Mediolateral - body to the side and CR at knee joint
OR axiolateral HB to include shaft and knee joint