CSD 538 FINAL REVIEW
Things to know:
Newborn VF length= 2.5 - 3.0 mm
Application Question: Opera singer who is on tour and has VF hemorrhage. Which would be the best treatment option for this patient?
Vocal rest and healthy vocal habits (drink more water, avoid caffeine/alcohol/tobacco)
Review the following:
Impact of cleft palate on speech, resonance, and feeding
Articulation errors due to cleft:
nasal emissions with consonants-plosives, fricatives, affricates
Turbulent nasal air emission
Compensatory articulation-glottal stops, weak omitted sounds
Nasal grimace
Articulators are unable to meet in the right positions due to restrictions from the cleft
Voice Disturbance:
Dysphonia- breathiness, hoarseness, glottal fry can mask hypernasality and nasal emissions
Short utterances due to wasted air from poor velopharyngeal closure
Vocal cord nodules- glottal stops=strain on larynx
Feeding:
babies are unable to suck on nipple during feeding and cleft can cause nasal regurgitation (food coming up through the nose)
Resonance:
Resonators are also unable to create proper airflow which can cause limited or excessive nasality. Feeding is difficult for babies with cleft lip/palate because they are unable to latch and suck.
What is the difference between hypernasality and hyponasality?
Hypernasality:
An excessive quantity of nasal resonance during speech is referred to as hypernasality. It happens when airflow via the nose is improperly produced during speaking sounds, giving the voice an excessively nasal tone.
Hyponasality:
is defined by a loss of typical nasal resonance during speech. It happens when sounds that normally require nasal resonance are produced with inadequate airflow through the nose.
What is Velopharyngeal insufficiency (VPI)?
The insufficient closure of the velopharyngeal port during speaking is a defining feature of velopharyngeal insufficiency (VPI). The velopharyngeal port is the orofacial-nasal opening, and normal speech resonance depends on its proper closure.
How does unilateral vocal fold paralysis occur?
When one of the larynx's vocal folds is paralyzed, it is known as unilateral vocal fold paralysis. Damage or malfunction of the nerves that regulate the movement of the vocal folds is usually the cause of UVFP.
Can occur during: surgery (thyroid/cardiac), neurological conditions (stroke,tumor), viral infections, neck trauma, can also be idiopathic.
Damage to Recurrent Laryngeal Nerve (RLN), either from viral onset, idiopathic, tumor compressing a nerve, or nerve injury.
In bilateral vocal fold paralysis, what will the patient struggle with if folds are paralyzed in an abducted position? What changes if the folds are paralyzed in a closed position?
A patient with bilateral VF paralysis in abduction would struggle to create voiced sounds and increase their volume. They would have a breathy and weak vocal quality because their VFs are open and would have swallow issues because the glottis is open.
Alternatively, bilateral VF paralysis in the adducted position would create difficulty breathing since their VFs are closed. They would have a strained, rough, vocal quality since air is not coming through the VFs.
What is the most common type of Spasmodic Dysphonia? What muscles are injected with Botox for Adductor SD? What muscles for Abductor SD?
Adductor Spasmodic Dysphonia (ADSD) is the most common form of SD. Botox is injected either unilaterally or bilaterally and innervates the muscle to temporarily block the release of acetylcholine at neuromuscular junction. This induces parisis to allow VFs to open more.
The most prevalent kind of spasmodic dysphonia is adductor SD. The involuntary contractions or spasms of the muscles that bring the vocal folds together during speech are its defining feature.
Injections of Botox are frequently administered to the thyroarytenoid (TA) muscle.
Less often than adductor SD, abductor SD occurs. When speaking, they spread the vocal folds apart. Speech becomes strained and often breathy as a result.
It is common practice to inject Botox into the posterior cricoarytenoid (PCA) muscle.
What are the speech/voice characteristics of the different types of SD?
Abductor SD (ABSD)
Characteristics: weak and breathy. VFs opened when it should be closed.
Adductor SD (ADSD)
Characteristics: strained. VFs are closed when they should be opened.
What does Botox do to nerve transmission?
Botox gives the ability to temporarily interrupt nerve-muscle communication.
By inhibiting acetylcholine release, Botox induces temporary muscle paralysis.
(Acetylcholine is responsible for transmitting signals from nerve cells to muscles, leading to muscle contraction.)
What is laryngomalacia? What are signs/symptoms?
A frequent congenital condition affecting the larynx
The soft tissues of the larynx are more floppy than typical in laryngomalacia, which causes the airway to partially collapse when breathing.
Signs and symptoms:
Noisy Breathing (Stridor), Worsening with Feeding, Retractions, Feeding Difficulties, Gastroesophageal Reflux, Cyanosis (bluish discoloration of the skin)
What may contribute to polypoid degeneration of the vocal folds?
Polypoid degeneration- Severe form, membranous portion becomes permeated with the fluid
Long-standing trauma or chronic exposure to irritants can contribute to polypoid degeneration
Cigarette smoke
Laryngopharyngeal reflux
What are vocal nodules and how do they form? What about vocal fold polyps?
Vocal nodules are:
The most common benign pathology
Inflammatory degeneration of the superficial layer of the lamina propria
Typically form bilaterally
May be acute or chronic
Caused by high impact stress during phonation or phonotraumatic behaviors
Typically are firm and callous-like
Vocal fold polyps
Fluid-filled lesion
Develops in the superficial layer of the lamina propria
Has its own blood supply
Typically forms unilaterally
Sessile pedunculated in appearance
Cause thought to be from acute vocal trauma or from phonotraumatic behaviors
Can occur as the result of a single traumatic incident
What are the options for speech post-laryngectomy? Which option sounds the most natural?
Esophageal speech (burp speech)
Tracheoesophageal prosthesis
Electrolarynx
Most natural= Tracheoesophageal prosthesis
What is leukoplakia? What risk is associated with this diagnosis?
White plaque like formation occurring on the vocal fold surface
Usually found at the anterior portion of the vocal fold but may extend into the interarytenoid area
Considered a precancerous state and should be biopsied
Primary cause is chronic irritation
Primary irritation is cigarette smoking
Environmental exposure to irritants
Alcohol use
Other inhaled drugs
Risk associated:
could be cancer
What are the symptoms of laryngeal cancer? What are the primary contributing factors?
Symptoms:
Hoarseness
Change in pitch (typically lower due to mass effect)
Vocal strain
Sore throat or globus sensation
Persistent cough
Stridor
Primary contributing factors:
Smoking
Alcohol use
Reflux
HPV
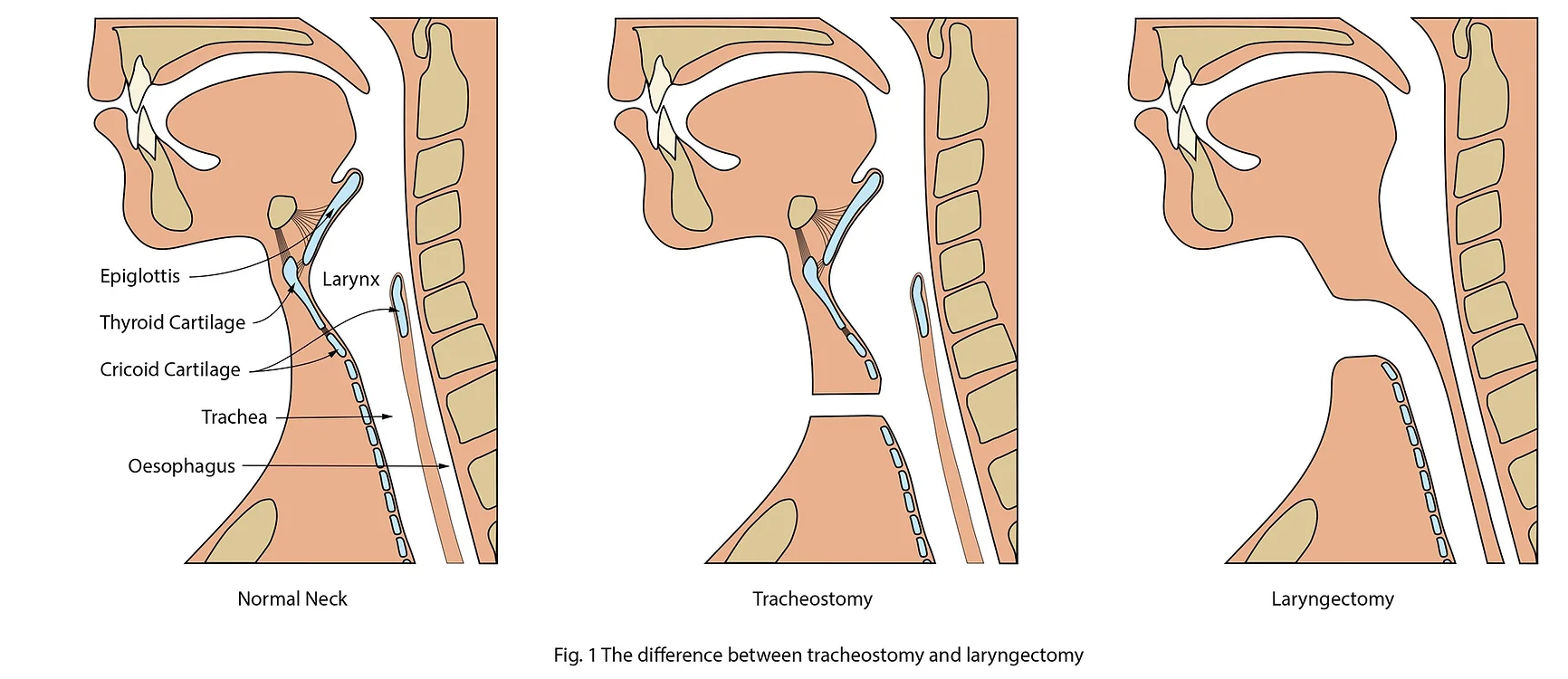
What is the difference between a laryngectomy stoma and a trach tube? Why is this important?
A tracheostomy:
is a surgical procedure that creates an opening through the neck into the trachea. There is still a connection from the nose or mouth to the lungs, so traditional airway manipulation will work. The tracheostomy can be short-term or permanent.
A laryngectomy:
is the surgical removal of the larynx, completely and permanently. The remaining trachea is sutured to the anterior neck. There is NO CONNECTION from the nose or mouth to the lungs, so traditional airway manipulation will not work. Laryngectomy patients are known as Neck Breathers - individuals who breathe through a neck stoma.
It is important because the appearance of the stoma can be confused for either one.
For a laryngectomy, it is impossible to deliver oxygen to the lungs with nasal cannula, face mask, or bag-mask ventilation. Attempts to intubate the trachea from above the stoma via the oral or nasal route will be unsuccessful.
What is medialization thyroplasty commonly used to treat?
Thyroplasty is typically used to treat unilateral vocal fold paralysis. A mesh device is placed into the paralyzed VF to bring it closer to the working VF. They can also be used to treat spasmodic dysphonia and help transgender patients achieve the pitch they are wanting.
What are the goals of voice therapy? What is the patient’s role in therapy?
Goals:
Aronson, 1985 – the objective is “the best possible voice within a patient’s anatomic and physiologic capabilities”
Colton and Casper, 1990 – “To restore the best voice possible, a voice that will be functional for purposes of employment and general communication”
Enhance voice quality by optimizing conditions under voice production
Patient’s Responsibility:
Completing their home exercise program outside of therapy sessions and maintaining vocal hygiene. The patient is also the one determining what they are looking to get out of therapy regarding their voice.
Review the treatment approaches and what they are commonly used for.
Hygienic Voice Therapy
Focus on behavioral causes of voice disorder and modifying/eliminating those factors to improve vocal quality.
Symptomatic Voice Therapy
Modification of deviant vocal symptoms such as breathiness, inappropriate pitch, loudness, hard glottal attacks, etc.
Focuses on modifying aberrant vocal symptoms observed by the patient or SLP, such as: high pitch, breathy voice, or hard glottal attack
There is a hierarchical pattern:
Patient identifies the behavior that needs to be eliminated or modified
Stimulate the desired target behavior by using facilitating techniques
Chant talk
Chewing/yawn-sigh
Confidential voice
Counseling
Head position
Laryngeal massage
Open mouth approach
Pitch Inflection
Psychogenic Voice Therapy
Focus on psychosocial and emotional factors that caused voice disorder. Once that is treated, then the voice will improve.
Physiological Voice Therapy
Vocal function based on objective voice assessment (laryngeal function study)
Strives to improve the balance among voice respiratory support, laryngeal muscle strength, control and stamina, and supraglottic modification of the laryngeal tone
Promotes a healthy vocal fold cover
concentrates on the modification of the underlying physiology of the voice producing mechanisms: respiration, phonation, resonance
Direct exercises are used to activate the laryngeal muscle and work other subsystems, such as respiratory and supraglottal systems
Examples:
Vocal Function Exercises-helps with hypo-hyperfunction voice disorders.
Vocal warm up, pitch glides, prolonged vowel /o/ at selected pitch
Lessac-Madsen Resonant Voice Therapy-helps w/ hypo-hyperfunctional voice disorders
Goal is for patient to use least amount of respiratory effort and stress on vocal folds
45 min sessions, 1-2 per week, for 6-8 weeks
Sounds→words→phrase→chant→conversation
***patient must be able to feel the vibrations in the first session, otherwise choose different tx method
Lee Silverman Voice Treatment-Increase loudness by increasing effort and coordination during speech production
4x/week, 4 weeks, 1 hr per session
Used with Parkinson’s Disease
Inspiratory and expiratory muscle strength training
Semi Occluded Vocal Tract Exercises- Some backflow of air which may help entrain better vibration of vocal folds
Can be used with lip/tongue trills, blowing bubbles with a straw, or bilabial fricatives
Call Technique- open throat and mouth like a megaphone and shout functional phrases. Emphasize the consonant and stretch the vowels.
Eclectic Voice Therapy
Uses a combination of other approaches to provide the most effective therapy.
What happens to the larynx if infected with human papilloma virus? What are the treatments?
Associated with an increase in cancers located in tonsils and base of tongue
First reported in 1983
Treatments associated:
Surgery alone
Transoral robotic surgery (TORS)
Full course radiation therapy (XRT)
Combination radiation and surgery
Chemotherapy before or during radiation
What are psychogenic disorders? Who are appropriate referrals for these patients?
Unexplained physical symptoms without relevant organic pathology
Accounts for about 45% of visits to clinics
Psychogenic and neurogenic symptoms can co-occur
May manifest as a speech/voice disorder
Voice is most common type
Speech: fluency, pseudo foreign dialect, infantile speech, prosodic
Differential diagnosis: the symptoms must fit the”rules” of a motor speech or voice disorder
Many psychogenic disorders can be treated by SLP’s
Prognosis is good
Patient’s belief that problem is organic must be addressed
Appropriate referrals
Behavioral therapy
Respiratory therapy
What are typical problems of singers? How are their complaints different?
Common complaints of singers include:
Loss of upper notes
Loss of flexibility
Prolonged warm-up
Difficulty singing loudly or softly
Difficulty with register changes (passagio)
Considerations for working with singers:
Singers may be prone to reflux
Problem may be in the speaking voice
Voice issues may be subtle, not readily visible on strobe exam
While under a scope, have them sing for you and see what you notice
What is irritable larynx syndrome?
1st described in 1999
Hypothesis is: ILS develops as a reaction to changes in the central nervous system, leaving sensorimotor pathways in hyper-excitable state. Adaptation to chronic noxious stimuli results in an altered response
Review the function of the intrinsic laryngeal muscles.
Responsible for the movements of the laryngeal cartilages and finer control of the laryngeal structures
Total of 5- all of which are paired
These muscles work together to regulate the tension in the vocal ligament and the size and shape of the glottal space
Define vocal fold mobility.
The degree of vocal fold movement during phonation
Define stroboscopy. How is it different from true slow motion?
Digital Laryngostroboscopy:
Imaging the larynx using a strobe light
Provide great image quality:
Allow retrieval of the images for later examination
Allow pre to post comparison of the laryngeal image
Videostroboscopy:
Most commonly used visual imaging for voice disorders
Parameters that are rated:
Glottal closure
Supraglottic activity
Vertical level of approximation
Vocal fold edge
Vocal fold mobility
Amplitude of vibration
Mucosal wave
Non-vibration portion
Phase closure
Periodicity
Overall laryngeal function
Laryngostroboscopy and videostroboscopy is different from true slow motion because true slow motion allows us to view the vocal fold movement in slow motion and stroboscopy does not allow us to see this or only allows us to review it frame by frame