Wk 7 - Drugs Acting on the Cardiovascular System
Drugs Affecting Blood Pressure
Hypertenstion
excessive high blood pressure
Is recognized as a major risk factor for several potentially lethal cardiac conditions, including myocardial infarction and heart failure.
This can damage the fragile inner lining of blood vessels and cause a disruption of blood flow to the tissues.
It also puts a tremendous strain on the heart muscle, increasing myocardial oxygen consumption and putting the heart muscle at risk
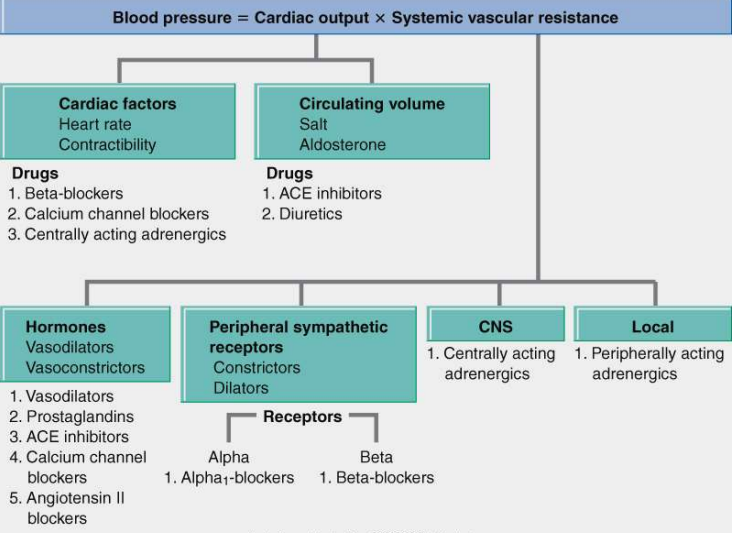
Blood Pressure = CO x SVR
- CO = Cardiac Output
- SVR = Systemic Vascular Resistance
Elements Determining Blood Pressure
Heart Rate
Stroke Volume
amount of blood that is pumped out of the ventricle with each heartbeat
Total Peripheral Resistance
resistance of the muscular arteries to the blood being pumped through
Categories Rating Severity of Hypertension
Normal: < 130/85
High Normal (Elderly): 13-=139/85-89
Stage 1: 140-159/90-99
Stage 2: 160-179/100-119
Stage 3: 180-209:110-119
Stage 4: 210 or greater/120 or greater
Classification of Blood Pressure
Hypertension can also be defined by its cause
Primary Hypertension
Essential, Idiopathic
UNKNOWN cause
90% of the cases
Secondary Hypertension
KNOWN CAUSE (Pheochromocytoma)
10% of the cases
High diastolic BP (DBP) is no longer considered to be more dangerous than high systolic BP (SBP)
Studies have shown that elevated SBP is strongly associated with heart failure, stroke, and renal failure
Thiazide-type diuretics should be the initial drug therapy for most patients with hypertension (alone or with other drug classes)
The previous labels of “mild,” “moderate,” and “severe” have been dropped
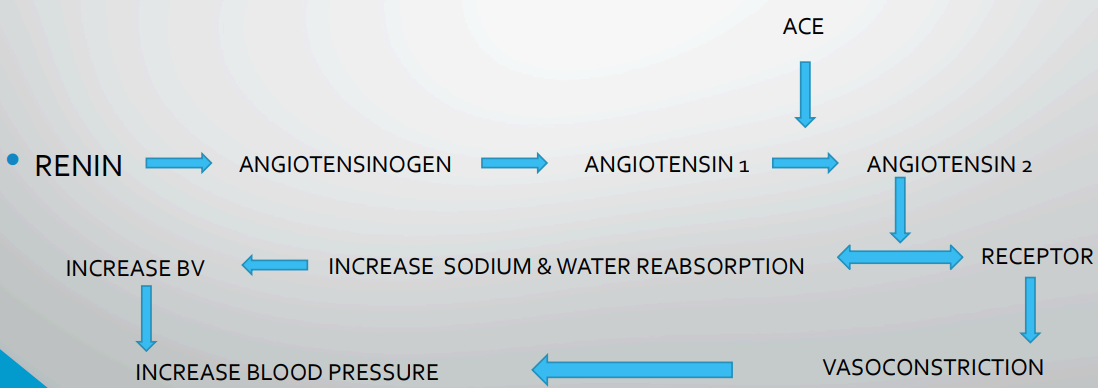
Renin Angiotensin Aldosterone System
Anti-Hypertensive Drugs
Diuretics
Diuretics are drugs that increase renal excretion of water, sodium & other electrolytes, thereby increasing urine formation & output
Used in:
management of heart failure
renal & hepatic disease
hypertension
Problems is Alteration of RAAS
Thiazide Diuretics
Decrease reabsorption of Na, water, Cl & bicarbonate in the distal convoluted tubule
Hydrochlorothiazide
Indapamide
Contraindicated: severe renal and hepatic impairment, hypokalaemia, hyponatraemia
Side effects: postural hypotension, hyperglycemia
Loop Diuretics
Inhibit Na & Cl reabsorption in the ascending loop of Henle
Furosemide
Bumetanide
ContraIndications: renal failure with anuria
Side Effects: hyponatraemia
Potassium-Sparing Diuretics
Act directly on the distal tubule to decrease the exchange of Na for K
Amiloride
Triamterene
Spironolactone
Block the Na-retaining effects of aldosterone in the distal tubule
ContraIndications: hyperkalaemia, renal failure
Side Effects: dry mouth, rashes, with spironolactone gynaecomastia can occur
ACE Inhibitors
2 Families of Drugs
The Problem is Altered RAAS (Renin Angiotensin Aldosterone System)
Angiotensin-Converting Enzyme (ACE) Inhibitors
(…pril)
Block the enzyme (ACE) that normally converts angiotensin I to angiotensin II
Decrease vasoconstriction & decrease aldosterone production, reducing retention of Na and water
Used to treat hypertension, heart failure, myocardial infarction, and diabetic nephropathy
Captopril (Capoten)
Enalapril
Lisinopril
Indications
hypertension
heart failure
diabetic nephropathy
left ventricular dysfunction after a myocardial infarction (MI).
Side Effects
Can produce serious first-dose hypotension
Cough, due to accumulation of bradykinin
Hyperkalaemia, due to inhibition of aldosterone release
Contraindications
In hypersensitivity to drug
Angiotensin II Receptor Blockers (ARBs)
(…sartan)
Compete with angiotensin II for tissue binding sites & prevent angiotensin II from combining with its receptors in body tissues
Used for hypertension, may be used as an alternative to ACE inhibitors in the management of heart failure and diabetic nephropathy.
Irbesartan
Losartan
Valsartan
Indications
hypertension
diabetic nephropathy (elevated serum creatinin and proteinuria)
Side Effects
Hypotension
Less likely to cause cough and hyperkalaemia than ACE inhibitors
ACE inhbitors and Angiotensin II receptor antagonists may cause first dose hypotension
Calcium Channel Blockers
Drugs the prevent calcium ions from entering cells
Vascular Smooth Muscle:
Calcium channels regulate contraction
If channels are blocked, contraction will be prevented and vasodilation will result
Act selectively on peripheral arterioles and arteries and arterioles of the heart (no effect on veins)
Heart:
Regulate function of myocardium, SA & AV nodes.
Myocardium
Positive inotropic effect (increases force of contraction)
Calcium is blocked, contractile force will diminish
SA Node:
Pacemaker activity regulated by calcium influx
Calcium is blocked, heart rate is reduced
AV Node:
Excitability of AV nodal cells is regulated by calcium entry
Calcium is blocked, discharge of Av nodal cells is suppressed (decreases the velocity of conduction through the AV node).
Chemical Families in CCB’s
Verapamil
Blocks calcium channels in blood vessels and in the heart
Used for:
Angina Pectoris (vasodilation)
Hypertension
Cardiac dysrhythmias
Careful administration/contraindications:
Cardiac failure, AV block, sick sinus syndrome
Diltiazem
Similar to Verapamil
Nifedipine
Relaxes vascular smooth muscle and dilates coronary and peripheral arteries
More effect on vessels less on myocardium
Used for:
Prophylaxis of Angina Pectoris (vasodilation)
Hypertension
Careful administration/contraindications:
Cardiac shock, advanced aortic stenosis, within one month of MI, acute attack of angina
Sympatholytics (Adrenergic Antagonists)
Suppress the influence of the sympathetic nervous system on the heart, blood vessels, and other structures
Increased activity in the SNS causes the hypertension
Five Subcategories:
Beta blockers
Alpha1 blockers
Alpha/beta blockers
Centrally acting antihypertensives
Adrenergic neuron blockers
Beta-Adrenergic Blockers
(…olol)
Most widely used antihypertensive drugs
Four useful actions in hypertension:
Blockade of cardiac beta1 receptors
Decreases heart rate and contractility (decreases cardiac output)
Suppress reflex tachycardia caused by vasodilators in the regimen
Blockade of beta1 receptors on juxtaglomerular cells of kidney reduce release of renin
Reduces Angiotensin II vasoconstriction, aldosterone mediated volume expansion
Long term use reduces peripheral vascular resistance
Adverse Effects:
Bradycardia, decreased AV conduction, reduced contractility
Contraindicated
Sick sinus syndrome/ AV blocks/ asthma (bronchoconstrictive effects)
Two Subgroups
Nonselective Beta Blockers (Propanolol Beta1 & Beta2 )
Reduce heart rate, decrease force of ventricular contraction, suppress impulse conduction through the AV node, suppress secretion of renin, bronchoconstriction, inhibition of glycogenolysis.
Propranolol hydrochloride
Sotalol
Timolol
Pindolol
Levobunolol
Nadolol
Metipranolol
Cardioselective Agents (Metoprolol-Beta1 only)
Reduce heart rate, decrease force of ventricular contraction, suppress impulse conduction through the AV node, suppress secretion of renin, bronchoconstriction, inhibition of glycogenolysis.
Atenolol
Acebutolol
Metoprolol
Bisoprolol
Esmolol
Betaxolol
Nebivolol
Alpha 1 Blockers
(…zosin)
Prevent stimulation of alpha1 receptors on arterioles and veins, thereby preventing sympathetically mediated vasoconstriction.
Resultant vasodilation results in lowered blood pressure
Blockade of Alpha1 receptors can cause orthostatic hypotension, reflex tachycardia.
1% of patients lose consciousness 30-60 minutes after receiving their first dose
NOT be used as first line therapy for hypertension.
Prazosin
Doxazosin
Indoramin
Terazosin
Alpha/beta blockers
Block Alpha1 and Beta receptors
Blood pressure drops:
Alpha1 blockade promotes dilation of arterioles/veins
Blockade of cardiac beta1 receptors reduced heart rate and contractility
Blockage of beta1 receptors on juxtaglomerular cells suppresses release of renin
Reduce peripheral vascular resistance
Watch for:
Bradycardia, AV heart block, asthma, postural hypotension
Prototypes:
Carvedilol, Labetalol
Centrally Acting Antihypertensives/ Alpha 2 Adrenergic Agonist
Methyldopa
Clonicine
Guanfacine
Use for management of hypertension in pregnancy
Block sympathetic activity within the brain
Adrenergic Neuron Blockers
Decrease blood pressure through actions in the terminals of the postganglionic sympathetic neurons.
Inhibit/deplete norepinephrine release
Resulting in decreased sympathetic stimulation of the heart and blood vessels
Watch for:
Severe orthostatic hypotension
Guanethidine monosulphate
Derisoquine
Contraindicated in heart failure, pheochromocytoma
Vasodilators
Vasodilators differ in respect to the types of blood vessels they affect.
Dilation of arterioles
Dilation of veins
Uses:
Hypertension, Angina, heart failure, myocardial infarction.
Adverse Effects
Orthostatic hypotension caused by relaxation of smooth muscle in veins. (dizziness, lightheadedness)
Reflex tachycardia places unacceptable burden on heart, tachycardia rises blood pressure
Expansion of blood volume-secretion of aldosterone—(diuretic may need to be added)
Hydralazine
Causes selective dilation of arterioles, has little or not effect on veins
Peripheral resistance and arterial blood pressure fall
Heart rate and myocardial contractility increase
DIRECT acting vasodilator
Uses:
Hypertension, heart failure
Adverse Effects
Reflex tachycardia, increased blood volume (sodium/water retention), Systemic Lupus Erythematosus-like syndrome (muscle pain, joint pain, fever, nephritis, pericarditis).
Sodium Nitroprusside
Potent and efficacious vasodilator
Fastest acting antihypertensive agent available
Causes venous and arteriolar dilation
IV infusion, onset is immediate
DIRECT acting vasodilator
Uses:
Hypertensive emergencies
Adverse Effects:
Excessive hypotension
Thiocyanate Toxicity (patients on med > 3 days)
Administration:
Degraded by light--cover
MIDODRINE - Reversal agent
ACE Inhibitors
Calcium Channel Blockers
INDIRECT acting vasodilator
NIFEDIPINE
AMLODIPINE
FELODIPINE
VERAPAMIL
DILTIAZEM
Sympatholytics
Nitroglycerin
Angina Pectoris
It is a coronary artery disease
Imbalance between decreased oxygen and increased cardiac workload
Types: Stable angina- no damage to heat muscle ; basic reflexes surrounding the pain rstore blood pressure: fixed at rest or with medicine
Unstable angina- episodes of ischemia occur even when at rest
Prinzmetal’s angina- caused byspasm of the blood vessel, not just by vessel narrowing
Antianginal Drugs
To increase oxygen
to decrease cardiac workload
Nitrates
Nitroglycerin
Nitrates are converted to NO (nitric oxide) in vascular smooth muscle
NO activates guanylate cyclase
Increase formation of cGMP so that the intracellular calcium levels decrease
Vasodilation
Used to treat or prevent angina
Relieves anginal pain by relaxing smooth muscles in the blood vessels (vasodilation) by several mechanisms
Dilate veins
Dilate coronary arteries
Dilate arterioles
Adverse Effects
Headache
Orthostatic hypotension
Symptoms include light headedness and dizziness
Reflex tachycardia
Examples:
Glyceryl Trinitrate
Isosorbide Mononitrate (Ismo, Imdur)
Isosorbide Dinitrate (Isordil)
Nitroglycerin (Nitro.Bid,Nitrostat)
Nitrate of choice before chest pain begins
Calcium Channel Blockers
inhibits the movement of calcium ions across the membranes of myocardial and arterial muscle cells
altering the action potential and blocking muscle cell contraction o
depresses myocardial contractility
slows cardiac impulse formation in the conductive tissues, and relaxes and dilates arteries
fall in BP and a decrease in venous return
decreases the workload of the heart and myocardial oxygen consumption
relieves the vasospasm of the coronary artery
increasing blood flow to the muscle cells (Prinzmetal angina).
Diltiazem
Beta-Adenergic Blockers
competitively blocks beta-adrenergic receptors in the heart and kidneys, decreasing the influence of the sympathetic nervous system on these tissues and the excitability of the heart;
decreases cardiac output, which results in a lowered blood pressure and decreased cardiac workload.
Metoprolol
Nadolol
Cardiotonic Agents
Cardiac Glycoside
Profound effects on the mechanical/electrical properties of the heart
Most widely used prescription drugs, they are the most dangerous (toxic—dysrhythmias)
Uses:
Heart failure, dysrhythmias
Digoxin
(Prototype - available in most counties)
Exerts a positive inotropic action on the heart (increases the force of ventricular contraction, enhancing cardiac output)
Uses:
Heart failure:
Increased cardiac output by increasing myocardial contractility
Sympathetic tone declines
→ Because Digoxin increases arterial pressure.
→ Heart rate is reduced, allowing more complete ventricular filling
Increased urine production
→ Increased cardiac output increases renal blood flow
→ Loss of water (urine) decreases blood volume which reduces cardiac distension, pulmonary congestion, and peripheral edema.
Decreased Renin Release
→ In response to increased arterial pressure, decrease in Angiotensin Decreased aldosterone decreases retention of sodium/water, reducing blood volume
Digoxin overall effects on CHF:
Cardiac output improves, heart rate decreases, heart size declines, constriction of arterioles and veins decrease,
water retention reverses, blood volume declines, peripheral and pulmonary edema decrease, weight is lost, exercise tolerance improves, fatigue is reduced.
Digoxin treats dysrhythmias:
Through a combination of actions, digoxin can alter the electrical activity in noncontractile tissue (SA & AV nodes, Purkinje fibers), as well as the ventricular muscle.
Toxicity:
Dysrhythmias: AV block, ventricular flutter, ventricular fibrillation
Predisposing factors:
Hypokalemia (usually secondary to the use of diuretics)
Elevated digoxin levels – Narrow therapeutic range
Heart disease
Side Effects: anorexia, nausea, vomiting, fatigue, visual disturbances
Administration: Count heart rate—less than 60 or change in rhythm detected HOLD THE DOSE AND CALL THE PHYSICIAN!
Phosphodiesterase Inhibitors
Inamrinone
Digoxin Antidote
Digoxin Immune Fab
Antidysrhythmics
Dysrhythmia (Arrhythmia):
Defined as abnormality in the rhythm of the heartbeat.
Associated with high degree of morbidity/mortality
Types:
Tachydysrhythmias: > 100bpm
Bradydysrhythmias:: <60 bpm
Vaughan Williams Classification:
Class I: Sodium Channel Blockers (Disopyramide, Lidocaine, Fleicanide)
Class II: Beta Blockers (Propranolol)
Class III: Potassium Channel Blockers (Sotalol)
Class IV: Calcium Channel Blockers (Diltiazem)
Class V: Other Antidysrhythmic Drugs ( Adenosine, Digoxin)
Cardiac myocyte Conduction Cycles
Phase 0: Depolarization, when voltage-gated fast sodium channels open, causing sodium to flow into the cell
Phase 1: Overshoot, when sodium channels close and potassium leaves the cell
Phase 2: Plateau, when calcium influx stabilizes the cell against potassium efflux
Phase 3: Repolarization, when calcium influx stops and potassium efflux increases
Phase 4: Resting, when sodium, potassium, and calcium are actively transported against electrochemical gradients

Class I: Sodium Channel Blockers
Sodium Channel Blockers:
Block cardiac sodium channels
Decrease conduction velocity in the atria, ventricles, and Purkinje system
Inhibits depolarization of Abnormal Rhythm
Acts on Phase 0
Class IA agents
prolonging repolarization
for atrial fibrillation, flutter; supraventricular & ventricular tachyarrhythmias
Eg: Quinidine, procainamide
SE: tachycardia, dry mouth, urinary retention, blurred vision
Class IB agents
shorten repolarization
for ventricular tachyarrhythmias (VT)
Eg: Lidocaine, Mexiletine
Class IC
minimal effect on repolarization
for life-threatening supraventricular tachyarrhythmias (SVT) and ventricular tachyarrhythmias (VT)
Eg: Flecainide, Propafenone
These drugs will be contraindicated in atrioventricular block
Class II: Beta Blockers
competitively blocks beta-adrenergic receptors in the heart and kidney, has a membrane-stabilizing effect, and decreases the influence of the sympathetic nervous system
Prolonged resting to slow down impulses and remove abnormal rhythm
acts on phase 4
Propranolol
Acebutolol
Esmolol
Class III: Potassium Channel Blockers
bind to and block the potassium channels that are responsible for repolarization
Prolong cardiac repolarization
Acts on Phase 3
Bretylium
For life-threatening ventricular tachycardia and fibrillation
can lead to hypotension
Amiodarone
Effective against both atrial and ventricular dysrhythmias (only for life-threatening because of toxicity—lung damage/visual impairment)
Dofelitide
Class IV: Calcium Channel Blockers
blocks the movement of calcium ions across the cell membrane, depressing the generation of action potentials, delaying phases 1 and 2 of repolarization, and slowing conduction through the AV node.
Acts on phase 2
Diltiazem
Verapamil
Other Antidysrhythmic Drugs
Adenosine:
Slows conduction through the AV node
Treats SVT
Short plasma half life (less than 10 seconds)
= Given IVP—closest IV site to the heart, followed by push of saline
Digoxin
Principles of Antidysrhythmic Drugs
Treat only if there is a clear benefit and then only if the benefit outweighs the risks
Treatment reduces:
Symptoms (palpitations, angina, dyspnea, and faintness)
Mortality
Bradydysrhythmias
Atropine:
Muscarinic Antagonist
Competitively block the actions of acetylcholine
Stimulation of muscarinic receptors decreases heart rate
→ Blocking these receptors will INCREASE heart rate
Isoproterenol
Acts on Beta-adrenergic receptors
Activates Beta1 receptors on the heartovercomes AV block, restarts the heart following cardiac arrest, increases cardiac output during shock
Drugs Affecting Blood Coagulation
Drugs Used to Control Bleeding
Antihemophilic Agents- Antihemophilic factor (Bioclate)
Systemic Hemostatic Agents – Aminocaproic acid (Amicar)
Topical Hemostatic Agents
Antiplatelet Drugs – Aspirin (generic)
Anticoagulants – Heparin (generic)
Low-Molecular Weight Heparins
Anticoagulant Adjunctive Therapy
Hemorrheologic Agent
Thrombolytic Agents – Streptokinase(Streptase)
Anticoagulants
Prevent formation of new clots and extension of clots already present
Heparin and warfarin (Coumadin) are commonly used
Used to prevent or manage thrombophlebitis, DVT, and PE
Main adverse effect is bleeding
Heparin
Intrinsic pathway is affected
Its major anticoagulant effect by inactivating thrombin and activated factor X (factor Xa) through an antithrombin (AT)-dependent mechanism.
Intravenous therapy
Require aPTT monitoring (Activated partial thromboplastin time)
Uses: Inhibit additional clotting, allowing body to lyse
current clot – Treatment and Preventative uses (hospital)
Pulmonary embolism (PE)
Stroke evolving
Massive deep venous thrombosis (DVT)
Adverse Effects
Hemorrhage
Heparin-induced thrombocytopenia
Hypersensitivity reactions
Contraindications
GI ulcers, blood dyscrasias
PROTAMINE SULFATE - Reversal Agent
Low-Molecular-Weight Heparin
Fixed dose schedule, don’t require aPTT monitoring
Can be used at home (unlike Heparin)
Much less likely to cause thrombocytopenia (than Heparin)
Therapeutic Use
1st line therapy to prevent and treat DVT
Prevention of DVT following surgery
Treatment of established DVT
Prevention of ischemic complications
Adverse Effects
Bleeding
ENOXAPARIN
Warfarin
Oral anticoagulant
Antagonist vitamin K
Blocks the biosynthesis of factors VII, IX, X, II
Anticoagulant effects occur 3-5 days after oral use
No effect on circulating clotting factors or platelets
Therapeutic Uses
Long-term prophylaxis of thrombosis
Prevention of venous thrombosis and associated pulmonary embolism
Prevention of thromboembolism (in patients with prosthetic heart valves)
Prevention of thrombosis during atrial fibrillation
Adverse Effects
Hemorrhage
Fetal hemorrhage and teratogenesis from use during pregnancy
Do not use during lactation
Antiplatelets
Aspirin
Suppress the production of prostaglandins and thromboxanes due to its irreversible inactivation of the cyclooxygenase (COX) enzyme
Normally COX produces prostaglandins, most of which are pro-inflammatory, and thromboxanes, which promote clotting.
Low-dose, long-term aspirin use irreversibly blocks the formation of thromboxane A2 in platelets, producing an inhibitory effect on platelet aggregation
This anticoagulant property makes aspirin useful for reducing the incidence of heart attacks
Adverse Effect
Increase risk of GI bleeding
Clopidogrel
Irreversibly inhibits ADP receptor on platelet cell membranes, which is important in aggregation of platelets and cross-linking by the protein fibrin.
Used to inhibit blood clots in coronary artery disease, peripheral vascular disease, and cerebrovascular disease
Adverse effects
hemorrhage
Severe neutropenia
Thrombotic thrombocytopenic purpura (TTP).
Aspirin and clopidogrel given orally
Fibrinolytic/Thrombolytic Drugs
First Generation – Streptokinase
Second Generation – Altepase (tPA)
Third Generation – reteplase recombinant (retavase)
Streptokinase
A protein (secreted by several species of streptococci) can bind and activate human plasminogen
Uses
Acute coronary thrombosis (acute MI)
Deep venous thrombosis (DVT)
Massive pulmonary emboli
Plugged AV shunt, central lines
Adverse Effects
Bleeding
Antibody production
Hypotension
Fever
Recombinant tissue plasminogen activator (t-PA, alteplase)
t-PA is produced by endothelial cells
It is nonantigenic and causes a more selective thrombolysis than streptokinase.
Alteplase, the recombinant t-PA, is produced by recombinant DNA technology.
Uses
Acute myocardial infarction.
Acute cerebrovascular thrombosis.
Pulmonary embolism.
Central venous catheter occlusion
Adverse Effects
Major bleeding.
Cardiac arrhythmias.
Anaphylactoid reaction.
Cerebrovascular accident.
Intracraneal hemorrhage.
Reteplase
It has an increased half life than t-PA and increased specificity for fibrin.
Its efficacy and adverse effect profile are similar to those of streptokinase and t-PA.
Antifibrinolytic Drugs
Interfere with the formation of the fibrinolytic enzyme plasmin from its precursor plasminogen by plasminogen activators
Block the binding sites of the enzymes or plasminogen respectively and thus stop plasmin formation
Aminocaproic acid and tranexamic acid
Use in bleeding tendencies
Tranexamic Acid
Aminocaproic Acid
Lipid-Lowering Agents
HMG-CoA Reductase Inhibitors – Atorvastatin (Lipitor)
Fibric acid derivatives (Fibrates)
Bile Acid Sequestrants – Cholestyramine (Questran)
Nicotinic acid (niacin)
Cholesterol absorption inhibitors – Ezetimibe
HMG CoA reductase inhibitors (Statins)
Inhibits HMG CoA reductase, the ratelimiting enzyme in cholesterol synthesis
Increase LDL receptors in hepatocytes
This enables hepatocytes to remove more LDLs from the blood
Also decrease VLDL levels and increase HDL levels
Examples
Atorvastatin
Fluvastatin
Pravastatin
Simvastatin
Adverse Effects
Headache, GI side effects (e.g. abdominal pain, flatulence, diarrhoea, nausea and vomiting)
Hepatoxicity
Myopathy
Fibric acid derivatives (Fibrates)
Increase oxidation of fatty acids in liver and muscle tissue, decrease hepatic production of triglycerides, decrease VLDL cholesterol and increase HDL cholesterol
Main indication is hypertriglceridemia (high plasma triglycerides)
Examples
Clofibrate
Fenofibrate
Gemfibrozil
Adverse Effects
Nausea, vomiting and GI upset
Cholelithiasis (stones in the gall bladder) and cholecystitis (inflammation of the gallbladder)
Myopathy
Bile Acid Sequestrants
Bind bile acids in the intestinal lumen. This causes the bile acids to be excreted in faeces and prevents them being re-circulated to the liver
Mainly used as an adjunct to Statins to decrease LDL cholesterol levels
Cholestyramine
adverse effects
Constipation, diarrhoea, nausea, vomiting, gastro-intestinal discomfort
Decreased absorption of fat-soluble vitamins
Nicotinic Acid
Inhibits mobilization of free fatty acids from peripheral tissues, thereby reducing hepatic synthesis of triglycerides and secretion of VLDL, which leads to decreased production of of LDL cholesterol
Besides reducing LDL and VLDL levels, also effective in increasing HDL levels
Adverse Effects
Flushing, itching, nausea, vomiting, diarrhea
Hepatotoxic
Hyperglycemia and hyperuricemia