Saliva Notes
Saliva: A Vital Fluid
Salivary Gland Anatomy & Secretions
Major Glands:
Parotids (serous, watery)
Submandibular (mostly serous, moderately viscous)
Sublingual (mainly mucous, very viscous)
Minor Glands:
Mucous secretion, except lingual serous glands (von Ebner's glands)
Locations: lower lip, tongue, palate, cheeks, pharynx
Absent in: gingiva, anterior hard palate
Saliva Composition & Production
Composition: 99% water, 0.5% electrolytes & proteins
Electrolytes: Sodium, potassium, calcium, magnesium, bicarbonate & phosphates
Proteins: Ig, enzymes (amylase, lysozyme), mucins, urea & ammonia
Average flow: 0.5 - 1.5 L/day
Production: Two-stage process
Primary saliva: Isotonic, produced in acini
Secondary saliva: Hypotonic, modified in duct network, low in sodium, glucose, bicarbonate, urea
Stimulated saliva: Hypertonic, increased Na levels
Factors Affecting Salivary Flow
Decreased flow:
Hypofunction (50% reduction)
Sleep (circadian rhythm)
Summer (circannual rhythm)
Reclined position, blindfolded, fasting
These decrease flow because they reduce the stimulation of salivary glands, leading to a lower production of saliva.
Increased flow:
Smoking, olfaction, vomiting
These cause increased flow because they stimulate the salivary glands through various mechanisms, such as the activation of taste receptors and increased nerve activity.
Control of Saliva Secretion
Salivary center in medulla
Triggers: Mechanical, gustatory, olfactory
Altered by pain, medication, disease
Parasympathetic NS stimulation: Constant low-level secretion
Sympathetic NS: increased protein (due to noradrenaline)
Parasympathetic NS: increased watery secretion (due to acetylcholine)
Nerve-mediated reflex, originating in salivary nuclei.
Saliva Functions & Components
Lubrication & protection
Buffering & clearance
Maintenance of tooth integrity
Antibacterial activity
Taste & digestion
Bicarbonates, phosphates & urea: pH modulation & buffering
Proteins & mucins: Cleanse, aggregate/attach oral microbes, contribute to dental plaque metabolism
Calcium, phosphate, proteins: Anti-solubility factor, modulate de- and re-mineralization
Immunoglobulins, proteins, enzymes: Antibacterial action
Growth factors: Wound healing
Proteins in Saliva
Proline-rich proteins: friction protection
Amylase: begins starch digestion
Lipase: lipid digestion
Mucus glycoprotein/proteoglycan: lubrication
Agglutinins: antigen aggregation
Cystatins: inhibit proteases
Histatins: antimicrobial/ antifungal/ antiviral
Statherin: enamel recal/prevent mineral accretions/ antimicrobial
Defensins: antibacterial/ antiviral
Lactoferrin: chelates iron
Growth factors EGF & VEGF: wound healing
Urea: raises pH
Lysozyme: damages microbe cell walls
Acquired Pellicle
Thin acellular film on surface epithelium and enamel
Protein/CHO/Lipids
Selectively binds salivary glycoproteins
Functions: Lubrication, remin/demin, influences early microbiome
Mucins (glycosylated protein)
Lubrication & Protection: Coating soft & hard tissues, barrier against irritants, carcinogens, chemicals, desiccation, diffusion barrier against acids, antibacterial, supports commensal bacteria
Complex protein molecules (glycoproteins) with low solubility, high viscosity/elasticity/adhesiveness
Adsorbs to tooth, contributes to pellicle, protects from acid, complexes with other proteins, binds to enamel, easily dislodged, aggregation & clearance of oral bacteria, predominates in caries-resistant patients
Buffering & Clearance
Most important functions for caries prevention
Bicarbonate (most important), phosphate, urea & amphoteric proteins neutralize acids
Clearance related to saliva flow rate; high flow rate = reduced caries risk
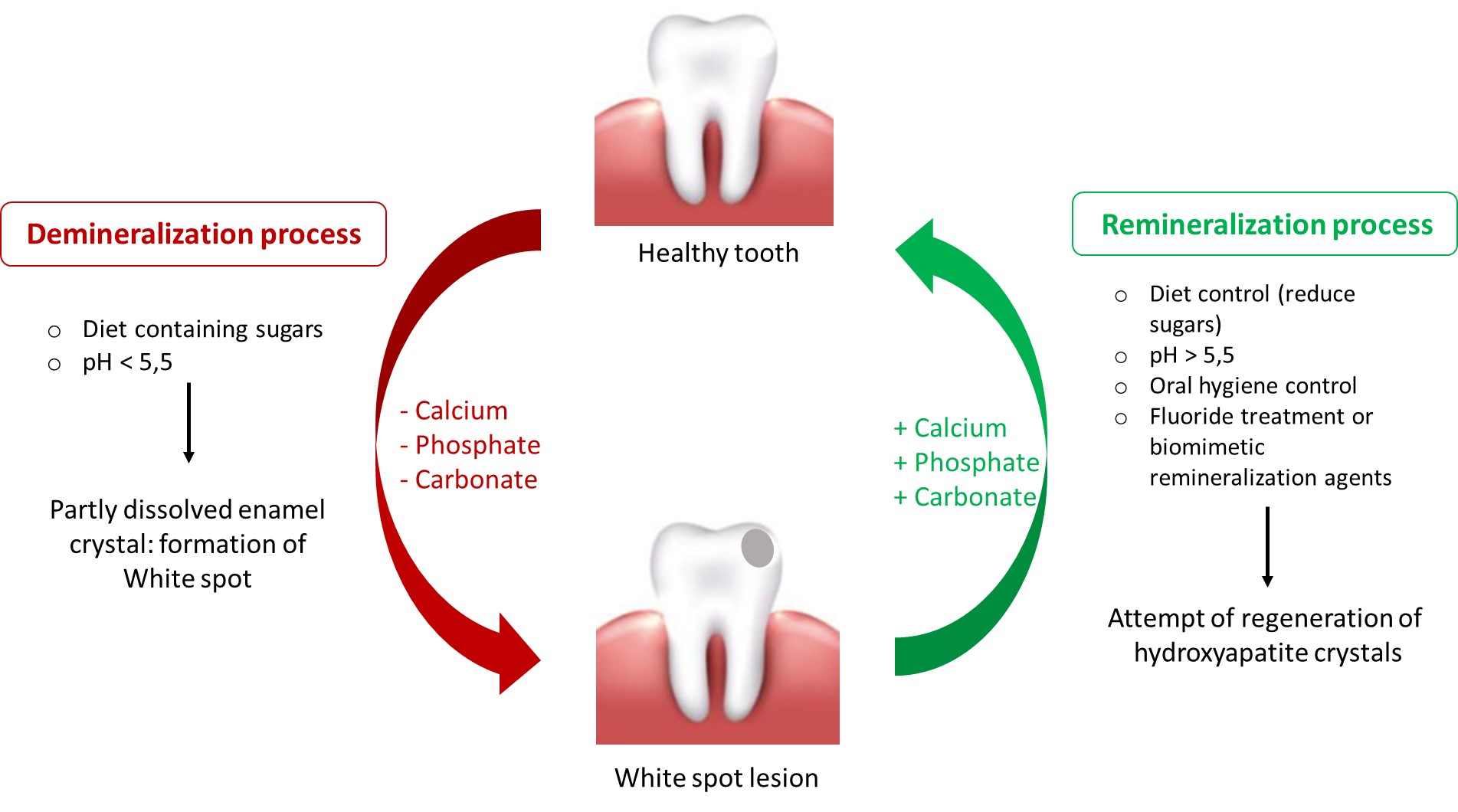
Maintenance of Tooth Integrity
Demineralization: Acids dissolve enamel crystals (pH 5-5.5)
Remineralization: Replacing lost minerals, supersaturation of salivary mineral, proteins bind to enamel surface, fluoride increases crystal precipitation