Short Term and Long Term Control of Blood Pressure
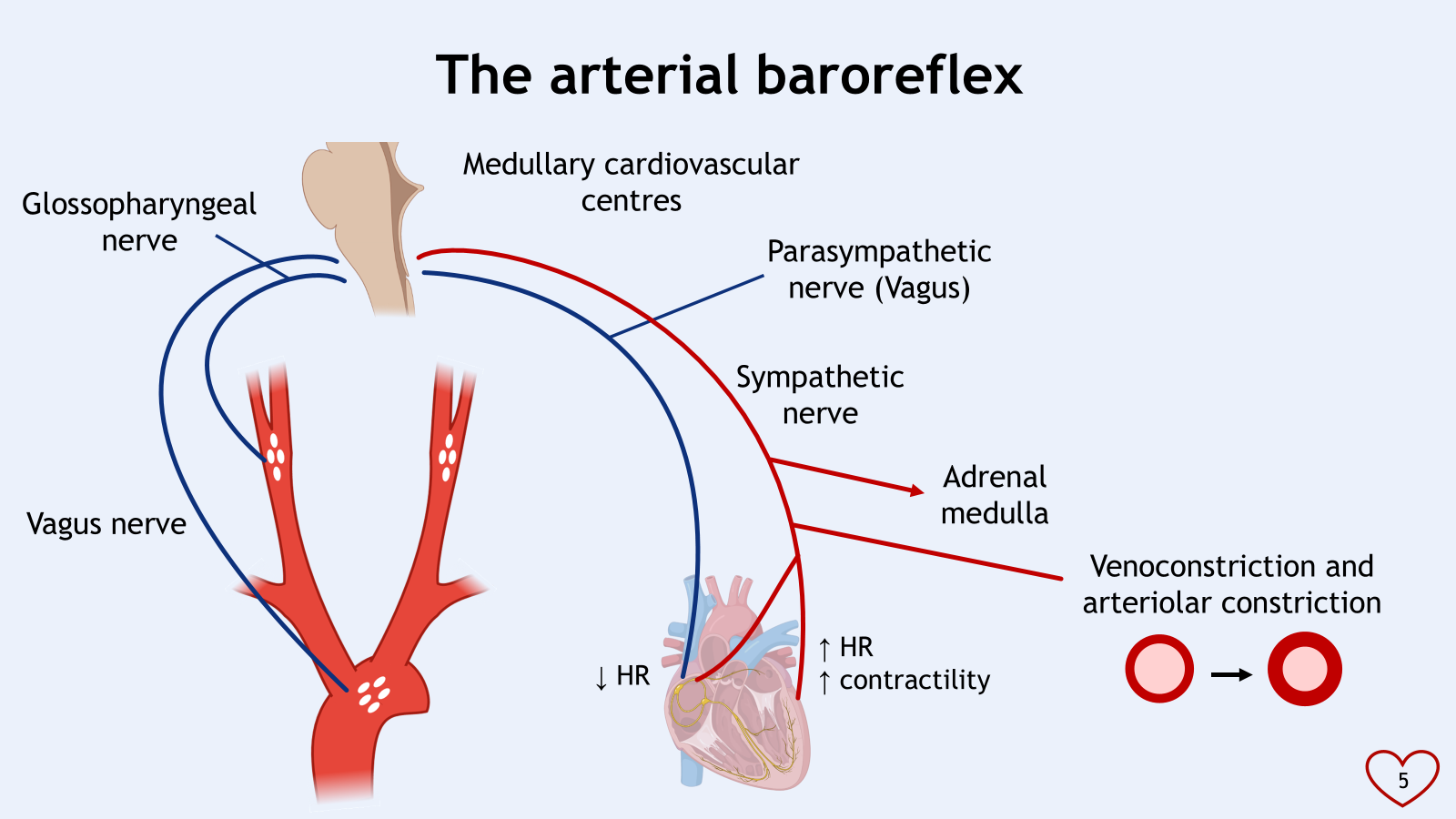
Other inputs to the medullary cardiovascular centres
•Cardiopulmonary baroreceptors
-Sensing central blood volume
•Central chemoreceptors
-Sensing arterial pCO2 and pO2
•Chemoreceptors in muscle
-Sensing metabolite concentrations
•Joint receptors
-Sensing joint movement
•Higher centres
-Hypothalamus and cerebral cortex
•Mean arterial pressure must be kept in the right range
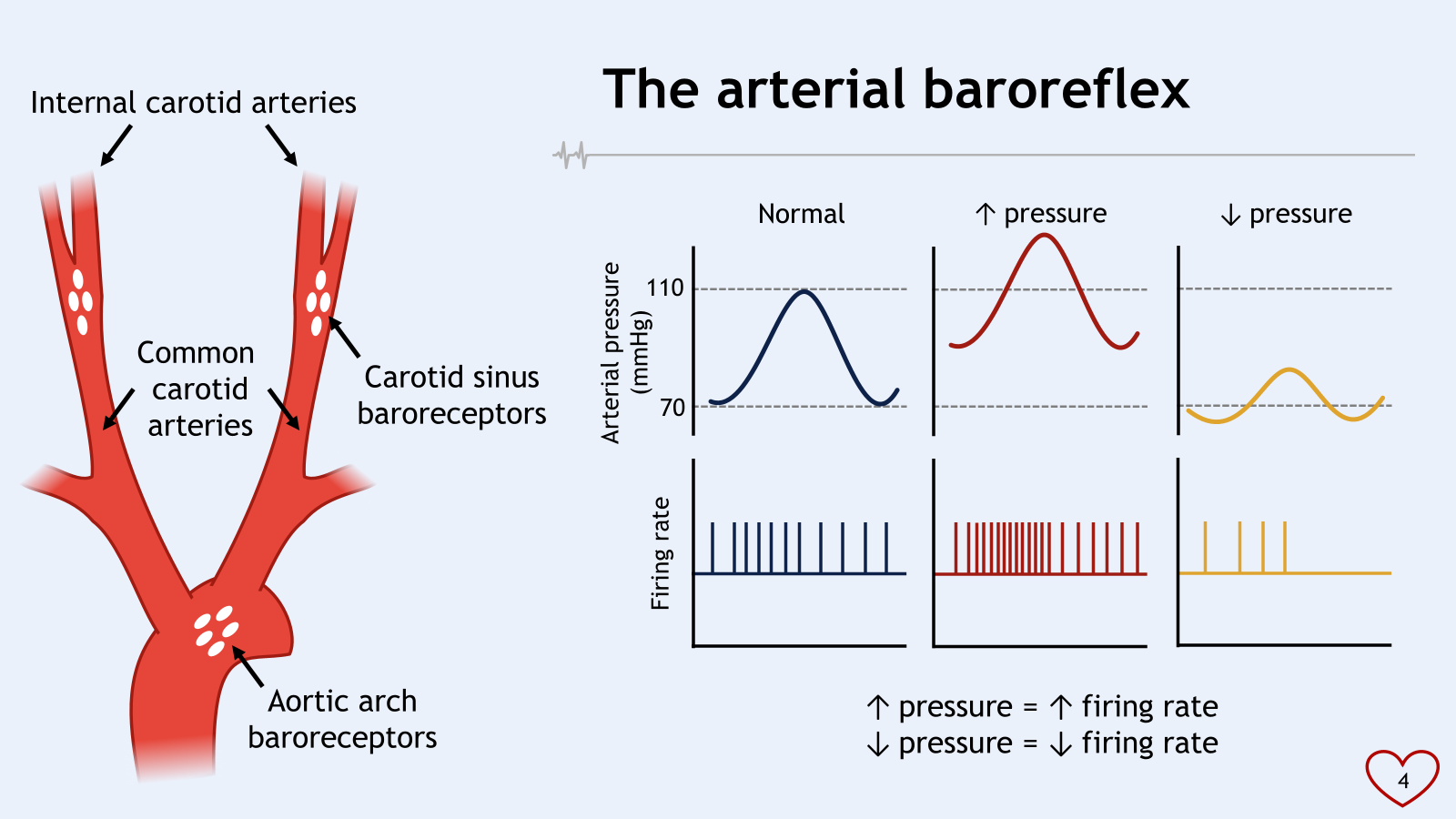
•The arterial baroreflex is responsible for the short term control of arterial blood pressure
•The medullary cardiovascular centres listen to other inputs as well though
•Long term control of blood pressure is different
*carotid body are chemoreceptors
*aortic arch and carotid sinus are baroreceptors
increased sympathetic tone generally leads to increased contractility, increased heart rate, vasoconstriction (of veins and venules and arterioles)
increased parasympathetic tone generally leads to decreased heart rate, no effect on contractility or venoconstriction
vasoconstriction increases MAP
arteriolar constriction increases TPR
venoconstriction increases VR (venous return) and CO (cardiac output)
Valsalva manoeuvre = forced expiration against a closed glottis
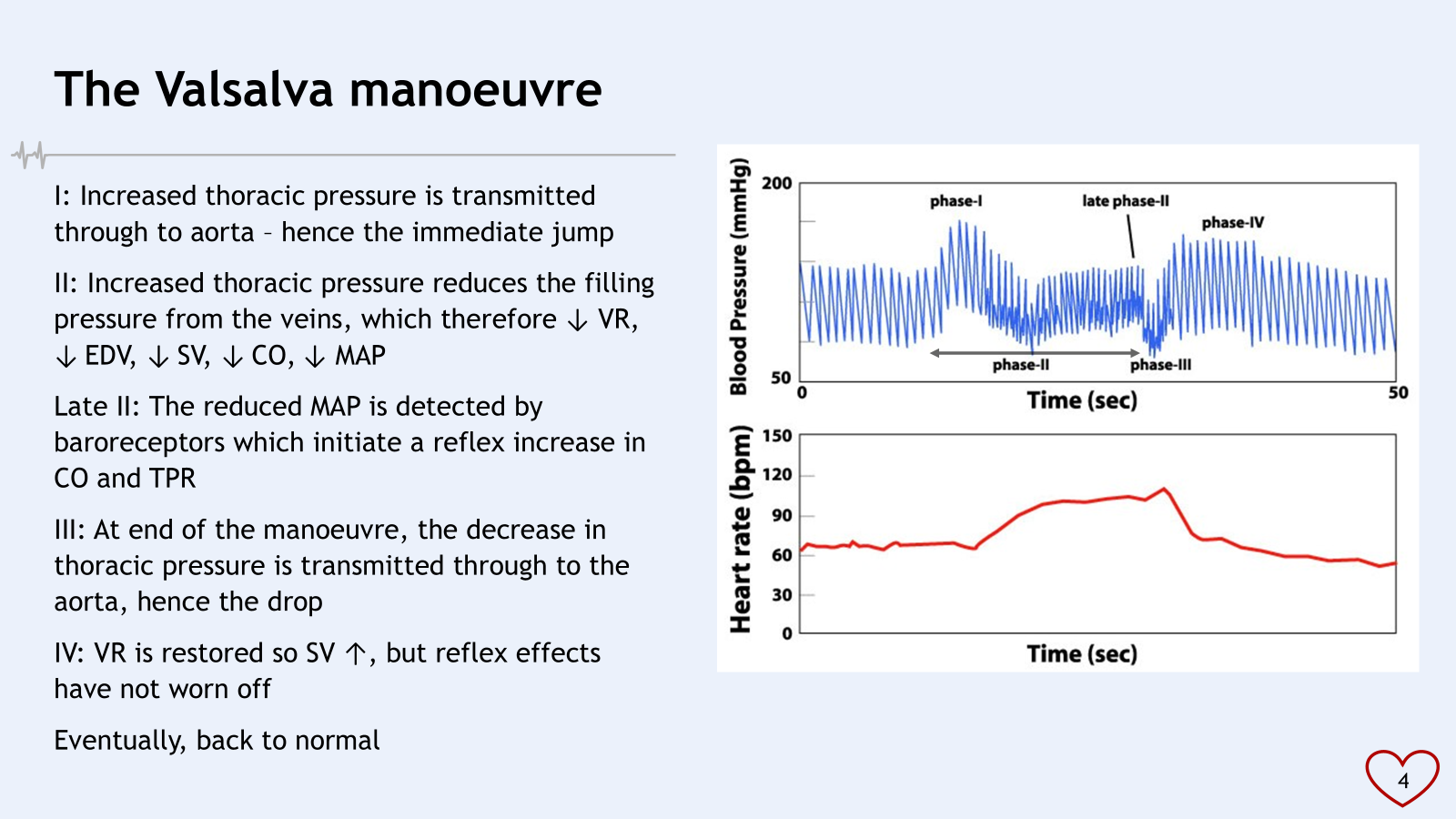
late phase II : constriction to increase VR and arteriole resistance?
IV : big increase in EDV, SV therefore large increase in MAP
baroreceptors reflex still active, send info to medullary cardiovascular receptors to bring pressure down
causes activation of muscarinic centres to slow down pacemaker cells
gradually BP comes down to baseline levels
valsalva manouevre used as a test of autonomic function
reduced in older people and autonomic neuropathy
unable to detect changes in MAP
during Phase II BP continue to fall as no detection
if they do valsalva manouevre on the toilet causes strain to heart
can increase risk of myocardial infarction
control of supraventricular tachycardia
changes in posture and the Valsalva manoeuvre are both good examples of the arterial baroreflex in action
baroceptor reflex becomes activated between phase I and phase II
blood flow through the capillaries is large total cross sectional area and low velocity (from previous lecture)
billions of capillaries causing large cross sectional area
skeletal muscle pump
respiratory pump (exercise increases depth of respiration, negative thoracic pressure increasing driving force pushing blood back to venous and venules increases venous return therefore increasing EDV)
increased venomotor tone
patterned flight socks
^all increase end diastolic volume
Long Term Control of Blood Pressure
kidney controlled
functions of kidney:
excretion of waste products
maintenance of ion balance
regulation of pH
regulation of osmolarity
regulation of plasma volume
controlling plasma volume is used to regulate MAP
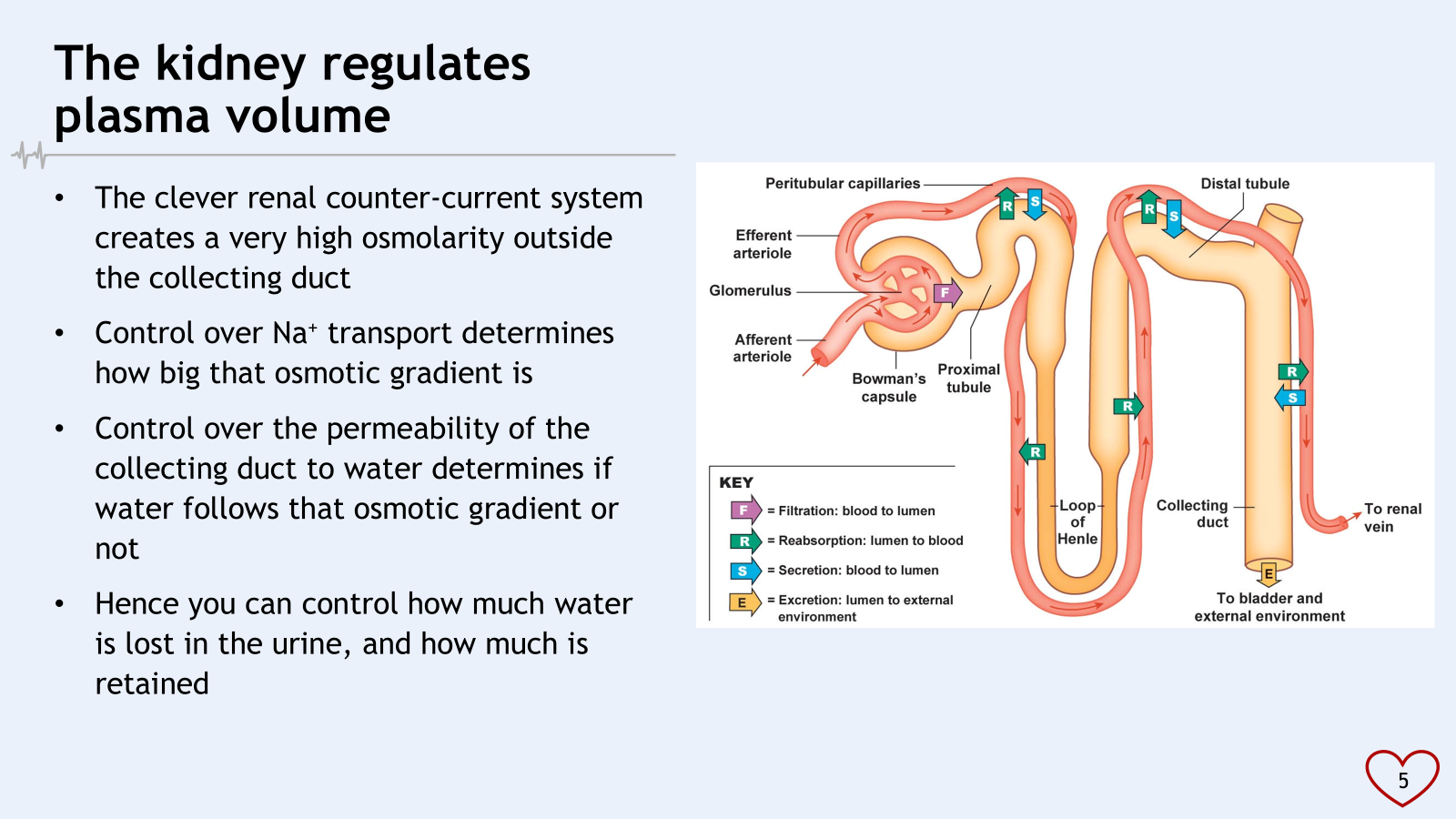
reabsorption : water and ions moving from the tubule into capillaries
secretions is opposite way, from blood to filtration?
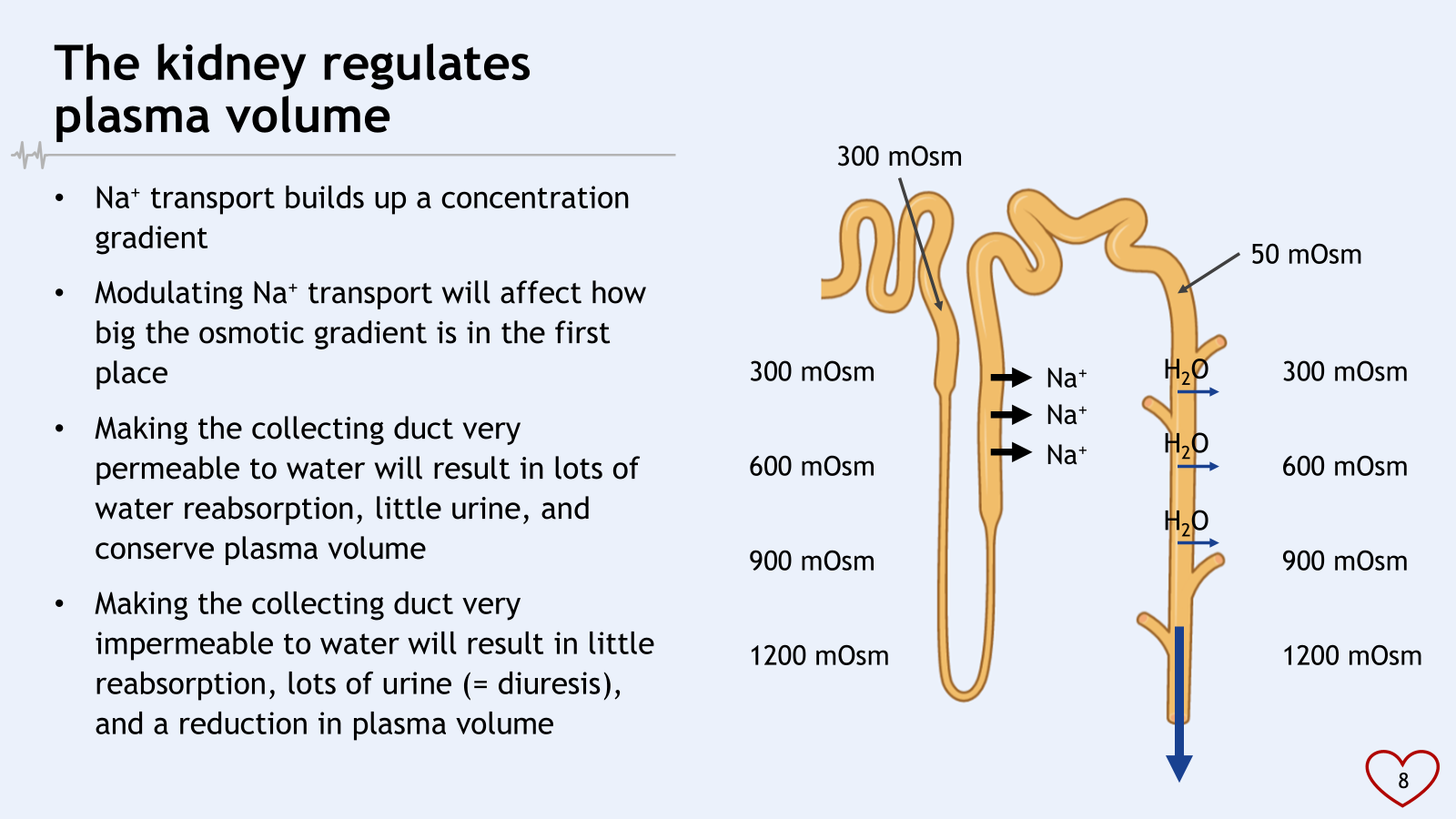
less water, left behind is solutes in loop of henle = high osmolarity
descending limb water going to stay there
how permeable we make the duct determines how much water will be reabsorbed
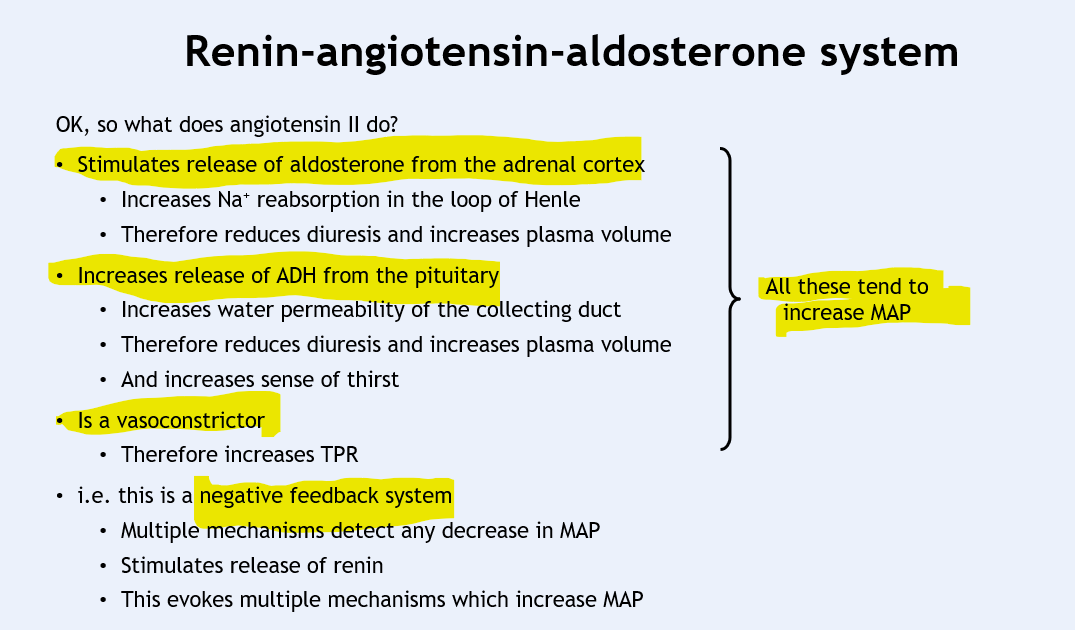
renin-angiotensin-aldosterone system (RAAS)
juxtaglomerular (granular) cells release renin
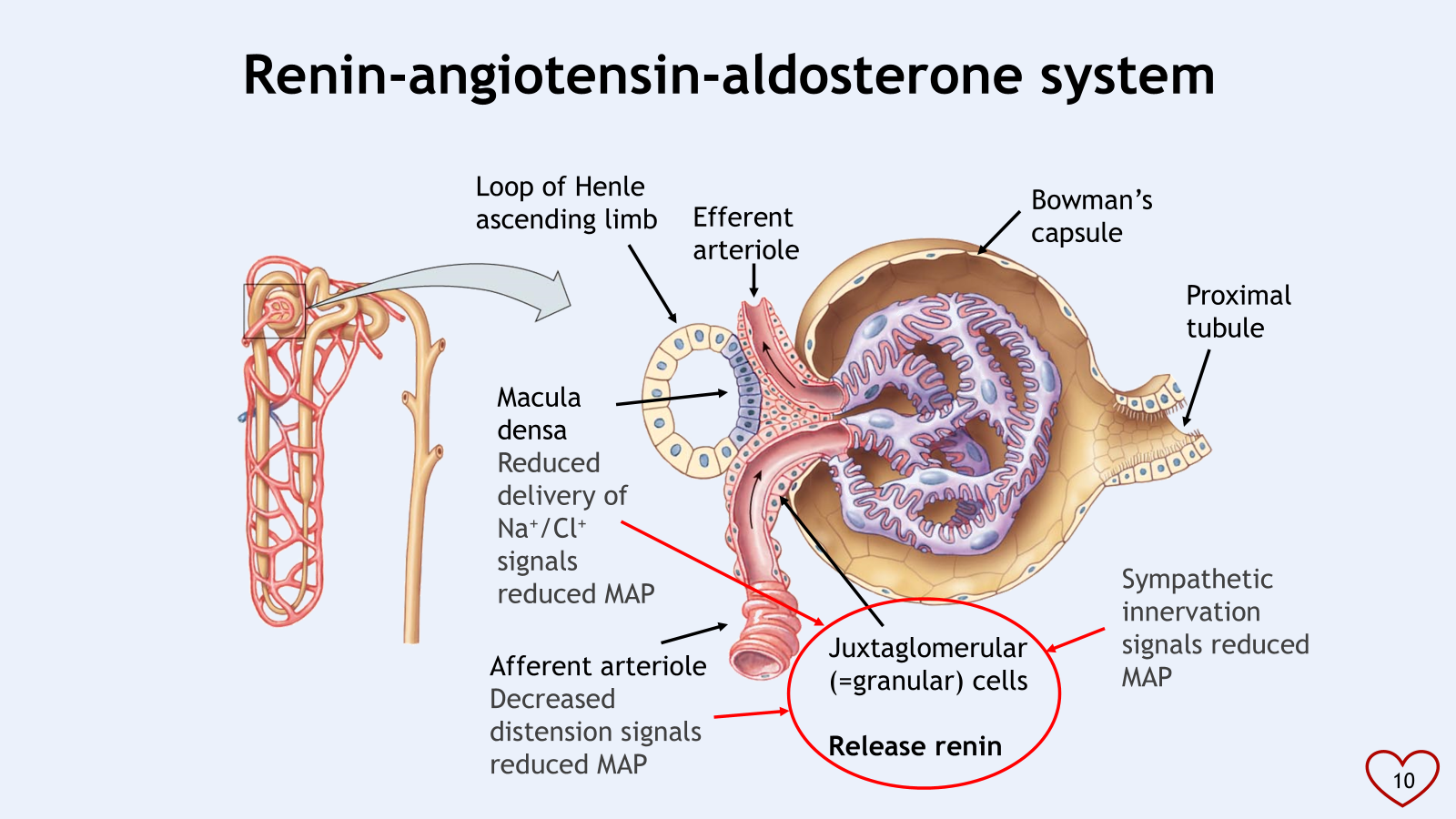
macula densa detects changed in Na+/Cl+
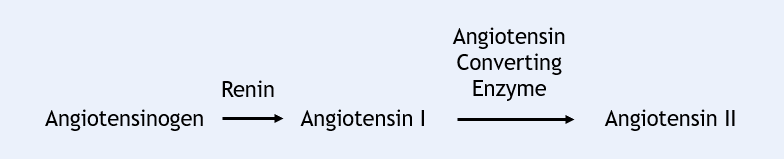
renin converts angiotensinogen (inactive) to angiotensin I to the more active angiotensin II
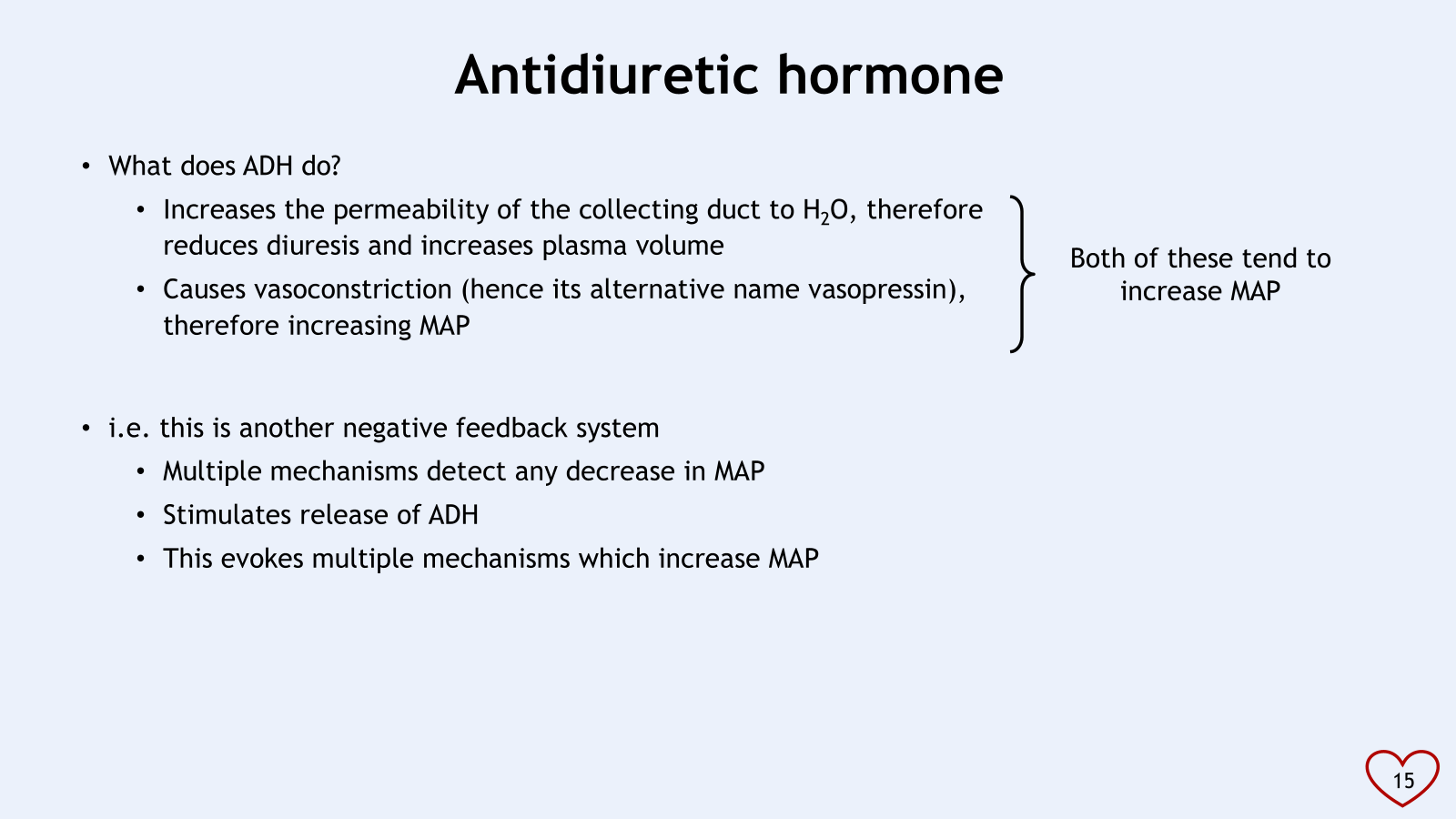
ADH synthesised in hypothalamus and released from posterior pituitary
Decrease in blood volume
Increase in osmolarity of interstitial fluid
Circulation angiotensin II
^all trigger ADH release, these are all signs of low plasma volume and/or MAP
alpha one, a1 receptors cause smooth muscle contraction and arteriolar constriction and increase total peripheral resistance,
binding of adrenaline and noradrenaline to alpha one causes arteriolar constriction?
the arterioles supplying cardiac muscle and skeletal muscle mostly express B2 receptors
preload is described as stretch on the myocardium before contraction
how much blood filling into ventricles before contraction, how stretched?