Clinical Voice Disorders
Objectives
Describe what dysphonia is
Dysphonia refers to altered vocal characteristics such as voice quality, pitch, resonance, vocal effort, or loudness.
Aphonia refers to a complete loss of voice.
Understand risk factors for voice disorders
Knowledge of who is at risk and associated factors contributing to voice disorders.
Categorisation of voice disorders
Recognise the different classifications of voice disorders.
Difference between organic and functional disorders
Distinguish between disorders with anatomical or neurological causes (organic) and those related to behavior (functional).
Influence of psychological strain
Awareness of how psychological distress can impact voice presentations, and its relevance in the assessment and management of voice disorders.
What Is A Voice Disorder?
Definition: "Voice disorders describe a range of conditions affecting the larynx and upper airway… changes in the auditory perceptual characteristics of the voice and/or the laryngeal sensations associated with voicing." (RCSLT, 2019)
Aphonia: Refers to the complete loss of voice.
Dysphonia: Denotes altered vocal characteristics, which could be associated with:
Voice quality
Pitch
Resonance
Vocal effort
Loudness
Inappropriateness/ unexpected for age, gender, or culture (dialects and language) of the speaker.
Risk & Prevalence
Voice Disorder Statistics:
Lifetime prevalence: 29.9% of people report experiencing a voice disorder.
Current prevalence: 6.6% report having a voice disorder when surveyed.
Chronic problems: 21.5% of those surveyed report chronic voice issues.
Acute problems: 78.5% report acute voice issues. (Roy et al., 2005)
Children can be at risk due to the use of their voice. Consider hearing impairments, ND, learning disabilities or children in general.
If you can’t hear your voice, hard to modulate it.
Who Experiences a Voice Disorder?
Demographic Data:
Children:
Age range of 7-12 years report voice disorders more frequently.
Greater prevalence in boys than girls.
Risk increases with involvement in sports and having siblings.
Associated factors: heavy voice use, nasal obstruction, hearing loss, allergies, upper respiratory infections (Martins et al., 2012; Angelillo et al., 2008; Mudd and Noelke, 2018).
Adults:
Age group of 40-59 years more common for experiencing voice disorders (Roy et al., 2005). Menopause or menstrual cycle- important to ask this. Female voice tends to get lower and men higher (loss of testosterone).
Over 70 years also shows increased risk (Cohen et al., 2012). Not using the muscles as much. Social aspects as an impact. How they use it and the other things that happen to your body over age.
Women are more likely to experience conditions like muscle tension dysphonia, while men are more likely to experience polyps or contact abrasion (Zhukhovitskaya et al., 2014).
Professional roles at higher risk involve high vocal load (e.g., teacher, singer, actor).
25% of working adults report losing significant work time due to voice issues (BVA, 2010).
Psychological/Emotional Factors (adults):
Psychological distress is strongly linked to voice disorders (Misono et al., 2016; Gomes et al., 2019). Isolation and the feeling that connects to that that can impact the voice.
Can result from acute events (bereavement, trauma) or chronic conditions (anxiety, stress).
Poor vocal hygiene, including inadequate hydration and irritants (e.g., smoking, pollution), can exacerbate these issues.
Recent thyroid, head and neck or thoracic surgery. Important to ask if they have had recent surgery.
Any voice loss exceeding three weeks should prompt investigation to rule out serious conditions, including cancer (Cancer Research UK, 2018).
Transgender individuals. Gender affirming voice. Harder to do things to increase the pitch of the voice. Can use testosterone to deepen the voice.
Categorisation of Voice Disorders
General Categorisation (McGlashan, 2008):
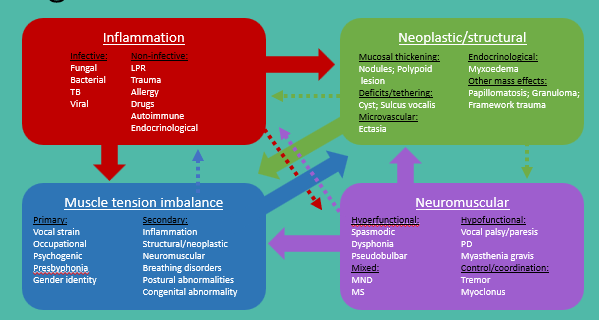
They can all influence eachother.
Typical Presentations of Disorders
Inflammatory Disorders:
LPR, laryngitis, Reinke’s edema caused by irritants, vocal load, bacterial infections, etc.
Neoplastic/Structural Disorders:
Present as cysts, polyps, nodules, granulomas, and presbyphonia.
Neuromuscular Disorders:
Includes spasmodic dysphonia, vocal tremor, vocal palsy, paresis.
Muscle Tension Imbalance:
Examples include muscle tension dysphonia and inadequate vocal cord adduction.
Functional and psychogenic issues like puberphonia and gender identity issues may arise.
Specific Factors Influencing Voice Disorders
Inflammatory:
Common causes include irritants (smoke, allergens) and exacerbated by poor vocal hygiene.
Certain medications, like antihistamines, can have a drying effect.
Vocal misuse.
Structural Factors:
Nodules & Polyps: Caused by phonotraumatic behaviors and vocal abuse.
Cysts: Result from glandular blockage or phonotraumatic behavior. Within the vocal chords. More inclidental (not drinking enough water).
Granulomas: Often arise after medical procedures (post-intubation).
Squamous Cell Carcinoma (SCC): Represents laryngeal cancer risk.
Recurrent respiratory papilloma (Acquired or congenital):
Caused by Human Papilloma Virus (HPV)
Neuromuscular Factors:
Vocal Fold Palsy/Paresis: Accounted as either congenital or acquired; can affect airway control and voice production.
Imaging will need to occur to investigate further.
Spasmodic Dysphonia: Associated with neurological dysfunction (dystonia affecting the basal ganglia) with three primary nerves: adductor (together- most common), abductor (opened), and mixed (least common).
Can’t use therapy to change it. Botox injection to the nerves.
Muscle Tension Dysphonia (MTD)
Presentation:
Commonly occurs as primary or secondary MTD.
Primary MTD: No underlying pathology but results from inefficient vocal behaviors. Pushing to get their voice heard.
Secondary MTD: Compensatory behavior due to glottal insufficiency or lesions.
Importance to distinguish between primary and secondary MTD for appropriate treatment planning (Morrison and Rammage, 1993).
Education of the role of the larynx and the use of their voice.
The limits of their voice and what they can achieve it.
Hyperfunction vs. Hypofunctional Voice Disorders
Hypofunctional Voice Disorders:
Characteristics include diminished (not enough) activity, under-adduction, reduced muscular recruitment leading to conditions such as vocal fold bowing and flaccidity.
Hyperfunctional Voice Disorders:
Present as excessive activity, over-adduction, strain, and associated issues like high laryngeal positions.
Clinical Considerations:
Understanding the underlying cause of voice disorders is essential for informed treatment, aiding in preventing exacerbation and injury.
Examples of treatment approaches include vocal exercises designed for specific dysfunctional patterns.
All about balancing everything out. Too much may overcompensate on another.

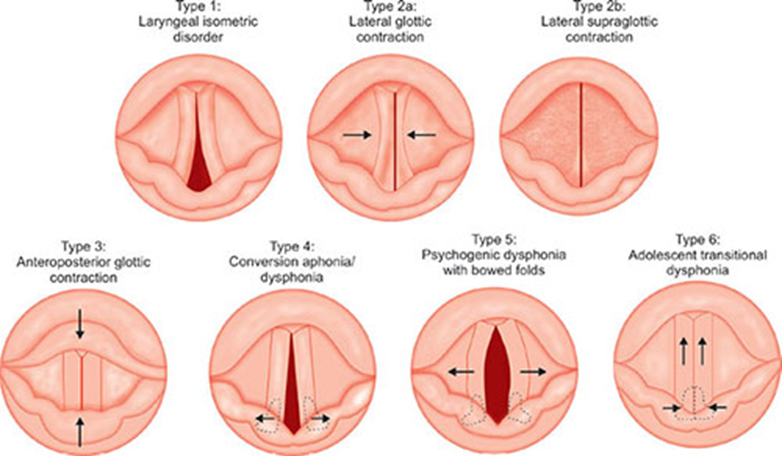
Psychogenic/Functional Dysphonia
Definition: "Loss of voice where there is insufficient structural or neurological pathology to account for the nature and severity of the dysphonia" (Baker, 2003).
Emotional Link: Explores the intrinsic relationship between emotion and voice. Input from the sympathetic nervous system may lead to physical symptoms related to perceived threats. Fight or flight. What is driving the presentation.
Biopsychosocial aspect to it. Not much of voice work is evidence based. Collaborative discussion between the therapist and the patient. Exploring what their voice feels like.
Types of Psychogenic/Functional Dysphonia:
Type 1: Classical (Hysterical) - Rare, accounting for approximately 5% of cases; involves repression and denial.
Unconscious conflict is converted into physical symptoms.
Type 2: Cognitive-Behavior Conversion - Common (approx. 95%); utilizes suppression as a coping mechanism; treatment generally easier as conflicts are nearer the surface. Awareness there is a problem but carry on. Can unpack this as there is an awareness.
High motivation for change.
Anxiety is converted into musculoskeletal tension e.g. dysphonia.
Type 3: Psychogenic-Habituated Conversion - Involves habit formation around dysphonia, often maintaining tension out of habitual response.
Uses suppression as a coping mechanism.
Category | Voice therapy | CBT | Psychiatry |
Type 1 Classical hysterical | Yes (diagnostic only) | No | Yes |
Type 2 Cognitive-behavioural | Yes | Yes | No |
Type 3 Psychogenic-habituated | Yes | Yes (preventing recurrence) | No |
Psychogenic/Functional Dysphonia goals
Goals of Treatment:
Increasing understanding of normal vs. abnormal phonation
Identifying triggers for dysphonia
Introducing phonatory techniques
Explore (carefully) potential secondary gain
Engaging multidisciplinary approaches to remove or reduce triggers.