↑↓Dysrhythmias pt.1, pt.2, drugs
Dysrhythmias— problem with impulse formation or conduction → ↓ CO (primary problem) and poor perfusion
Nsg priority: identify cause and treat underlying problem.
What causes Dysrhythmias:
MI: when the heart tissue dies → irritates/block normal conduction
electrolyte imbalance
K: Resets each beat (repo)
↓K → ↑ cadiotox → PVC—extra heartbeats in the lower chambers of the heart
Mg: maintain steady heartbeat
Ca: SA node fire; AV node speed; Allows for the heart muscles to contract AKA for Squeezing
hypoxia (starve the heart of energy it needs to contact) & hypovolemia (force the heart to beat abn fast)
Hormonal changes (thyroid and stress hormones): ↑ stress = ↑ SA node firing
Meds, caffince, nicotine, alcohol are stimulants → interferes in timing, irritates heart muscle → extra/ misplaced beats
Contributing Factors: H | T |
Hypovolemia: heart has nothing to pump → heart starts beating more → ↑ HR | Toxins |
Hypo/Hyperkalemia: impacts repolarization → Electrical chaos | Trauma |
Hypothermia → slows body metabolism & electrical conduction → heart stops | Thrombosis: blocks blood flow creating tissue death and electrical failure |
Hypoxia: starves the heart of the enegry it need to maintain steady heart rhythm | Tension Pneumothorax: creates pressure on the heart, squishing it to prevent it from beating |
Hypoglycemia: deprives heart cells of fuel→ starves | Tampande (fluid build up in the sac around the heart) : squeezes the heart so tightly that it cannot fill up w/ blood |
H ions: ↑ acid level in the blood → chemical changes in the blood make it difficult for electrical impulses to travel correctly |
S/S:
↓ | Rapid slower, irregular pulse | Reflects disturbed/conduction of heart impulses |
↓ | Hypotension | Decreased amount of blood that is pumped out |
PP | Pallor clammy, or cyanotic skin | Body poles blood from the skin to supply vital organs |
PP | Decreased U/O | Decreased perfusion to the kidneys |
PP | Feeling of impending doom | Decrease in blood flow to the brain signaling that it is in crisis |
SA node → P wave: | atrial depolarization → atrial contraction (squeezing) |
PR interval: | 0.12 to 0.20 sec |
QRS complex: | ventricular depolarization → ventricular contraction (squeezing) , and atrial repolarization → atrial filling; 0.04 to 0.10 sec |
T wave: | ventricular repolarization → ventricles filling |
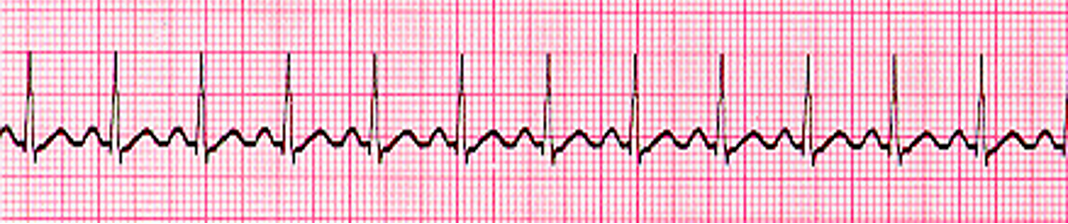
Sinus Tachycardia: HR > 100
Key feature: Normal rhythm, just fast (SA node firing rapidly)
Why: 1. pain, fever, anxiety: release of stress hormones → forces SA node to fire quickly
2. Hypovolemia: force the heart to beat faster when blood volume is low
Trx. 1. treat underlying cause
meds: 1. Beta blockers (Propranolol): ↓ firing of SA node + ↓ contractility
2. Calcium channel blockers (Verapamil + diltiazem): slows SA node + delay electrical signals as they passed through the heart
Nursing priorities: monitor vital signs and EKG
Assess perfusion (↑ HR, ↓ BP): pale skin, decrease U/O
Labs and electrolyte imbalance: mg, ca, k

Sinus Bradycardia HR <60
key feature: normal for athletes, but medical concern when symptomatic:
dizziness (indication of ↓ CO)
weakness
hypotension → fewer squeezes per minute → less pressure in the arteries to push blood through the systemic circulation
Trx:
non symptomatic: O2: address hypoxia
symptomatic PRIMARY TRX.: Atropine: block the “brakes” of the heart → ↑ HR
IN ATROPINE FAILURE use Dopamine or epinephrine
Temp pacing if needed
Nsg priorities: monitor EKG + vitals for poor signs of perfusion

Supraventricular Tachycardia (SVT) rapid ATRIA rhythm 100-280 bpm
key feature: fast atrial HR w/ no P waves (heart is beating so fast that there is very little time in between beats so it get hidden in the T wave)
Trx.
Vagal maneuvers- natural way of stimulating the vagal nerve—acts as brakes to help it slow down → ↓HR
Adenosine: chemical rest button that has a short life span of 1.5-10 sec sos it must be injected close to the heart to slow down electrical signal as the pass through the AV node
Recurrent SVT long term treatment: radiofrequency catheter ablation
most effective for SVT
Identifies using EPS and destroys the cardiac tissue cause the SVT by using radiofrequency waves to destroy irritable focus
complication: damage to the normal conduction or cause heart blocks
UNSTABLE MEDICAL EMERGENCY( signs of poor perfusion—↓BP, LOC): Cardioversion: shocking heart
Nursing priorities: ↓ CO: when the heart beats this fast it doesn’t have enough time to fill w/ blood in btwn beats → ↓Bp & s/s of poor perfusion

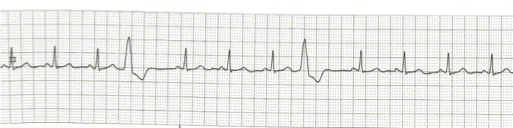
Atrial fibrillation CHAOTIC ATRIAL activity 350-600 bpm
key feature: most common dysrhythmias where the Atria quivers from receiving hundreds of electrical signal instead of 1→ failure to pump blood effectively to the ventricles → blood pools in chambers causing clots that travel to the brain → stroke
Trx: to control rate: BB,CCB, digoxin: Block chemical signals from reaching the AV node
PREVENTION: Anticoag
EMERGENCY: cardioversion or ablation
nursing priorities: Antidysrhythmic Meds
monitor signs of poor perfusion or clot related complications (stroke symptoms)
monitor K due to digoxin or amiodarone → hypokalemia → digoxin toxicity
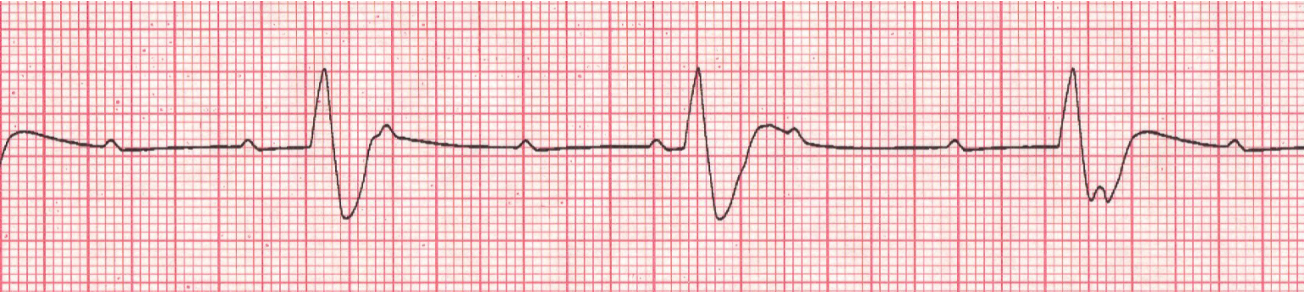
Premature Ventricular Complexes (PVCS)
key feature: early ventricular beat for irritable focus (sends out a signal before it is supposed to) → heart has less time to fill with blood → weak beat → ↓ amt of total volume being pumped to the rest of the body aka ↓ CO
Trx. correct underlying cause: caffeine, nicotine, alcohol, stress
Replace K or Mg because they act as electrical stabilizers so when it is low its not stable and contribute to excess firing
FREQUENT: BB (propranolol): ↓ firing and ↓ irritability
Nursing priorities: Identify cause
monitor poor perfusion (↓ BP or dizziness) → ↓CO

Ventricular Tachycardia Rapid VENTRICULAR rhythm >140 bmp
Key feature: electrolyte imbalances of K & Mg → Chambers don't have enough time to fill with blood between beats → dangerous drop in CO → cardiac arrest
This is serious because regular rhythm can quickly turn into ventricular fibrillation (VFib)—state of total electrical chaos where there is no organized beat and provides NO BLOOD FLOW to the body
Trx:
elective cardioversion if stable (no signs of severe poor perfusion yet)
Amiodarone: delay, the reset button on repolarization of the heart cells
MEDICAL EMERGENCY IF pulseless: Defibrillation: delivers high energy shock to stop the electrical chaos
Nursing priorities: Assess for pulse
Monitor vitals + electrolytes (K, Mg)
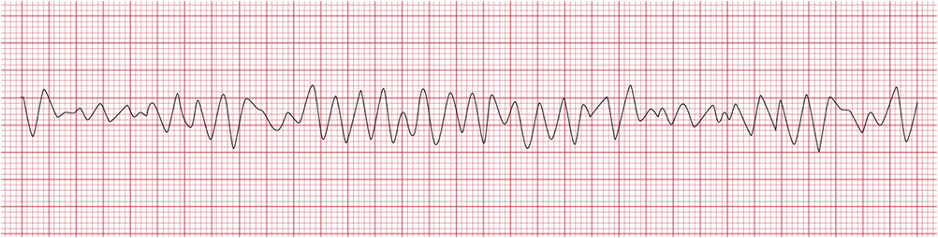
Ventricular fibrillation: MOST DANGEROUS
Key features: electrical chaos ventricles, where instead of one organized signal telling hard to beat hundreds of disorganized impulses fire at once → ventricle quivers → total failure of the hearts pumping system—no pulse and 0 CO due to organize contraction
Trx: immediate defibrillation — give SA node opportunity to take back control
CPR while waiting for dfib
Epinephrine: stimulate the heart to reset
antidysrhythmic med (amiodarone/lidocaine): stabilize a hearts electrical system, and prevents chaotic rhythm from occurring
Nursing priorities:
Call for help and start CPR immediately while preparing for D fib
Once stabilized long-term therapy such as implantable cardioverter defibrillator (ICD) will be used to shock the heart if Vfib happens again
One or more episodes of spontaneous sustained VT or VF (not caused by a MI)
Education: avoid magnets & sources of electromagnetic interference, cell phones, sit/lie down if dizzy
Heart block: impaired conduction through the AV Node or conduction system

Firstdegree AV block PR > .2 sec (five small boxes)
Key feature impulse that has difficulty moving through the AV NODE
Trx:
Check medication
On going monitoring
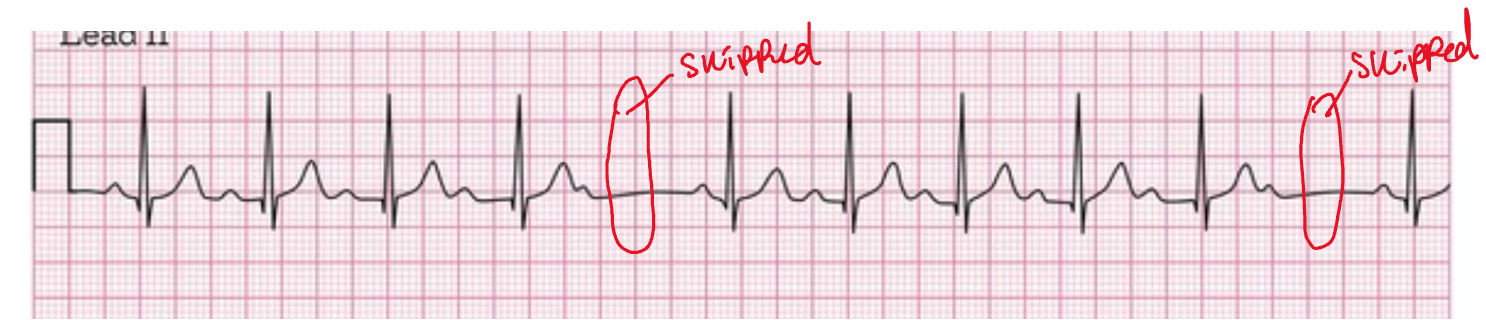
Second-degree AV block Mobitz type I (wenkeback) —WARNING PR
progressively length until a ventricle beat is skipped
Key features: not all of the atrial poses are conducted through to the ventricles
Trx:
ASYMPTOMATIC: ongoing monitoring
SYMPTOMATIC: atropine .5 mg to max three

Second-degree AV block Mobitz type II — RAPIDLY PROGRESS TO COMPLETE HEART BLOCK not all atrial pulses are conducted to the ventricles
Key features: PR intervals are the same (fixed) vs type I has prolongation
Trx:
Pacing (transcutaneous/trans Venus): until permanent base can be placed
Consider epinephrine or dopamine infusion to maintain BP until the pacing is started
Third- degree AV block (complete heart block)
Key features: complete block of the AV node, the bundle of his or the branches → disassociation of impulse between atria and ventricles → ventricles fire independently at a slower rate
Trx:
Temporary facing until you can get a permanent one
Dopamine and epinephrine to accelerate ventricular rhythm
Atropine is not effective because the block is below the AV node
Pacemakers
for symptomatic bradycardia or heart block to pace and sense
Types:
Temporary (non surgical) — electrical stimulus spread throughout the heart to depolarize the cells
transvenous
Invasive (subclavial) and inserted in an emergency
transcutaneous—used as an emergency measure until invasive pacing can be used or until HR returns to normal
Non-invasive and external electrodes that electrical impulses→ stimulate ventricular depolarization when HR is lower than the set heart rate on the base maker
Permanent implanted pacemaker
atrial pacing | ventricular pacing | A-V sequential pacing |
to cause atrial depolarization (delivering impulses that will travel to the AV node to then travel down to the ventricles for contraction | ventricular depolarization | Delivers impulse at atria first for contraction and then ventricle |
one spike → Abnormal P wave (atrial capture) → normal QRS | One spike → abnormal P wave (atrial capture) → second spike → a wide QRS (ventricular capture) |
Pacemaker Malfunctions:
failure to sense
oversensing: The pacemaker incorrectly detects non-cardiac electrical signals (like muscle movement or outside interference) as actual heartbeats. Because it "thinks" the heart is beating fine, it stays quiet, resulting in not enough paced beats
undersensing: The pacemaker fails to see the heart's natural beats. Because it doesn't know the heart has already fired, it sends out its own signal anyway, leading to extra, unneeded paced beats
failure to capture: You will see the pacemaker’s electrical spike, but it is not followed by a P wave or a QRS complex. The signal happened, but the heart did not contract.
failure to pace: no impulse initiated (no pacer spikes) during a time when the heart rate is slower than the pacemaker's set limit
causes: hardware or power issue: broken lead, battery failure, a displaced lead, or a total generator failure
Nursing focus: monitor rhythm and device function
possibly monitor for poor sign of perfusion
Dizziness, weakness, and ↓ HR are the primary signs of battery or device failure
Nursing edu:
Lifting restrictions (4 weeks) so leads won’t dislodge
Teach pulse taking: ONE FULL MIN + REPORT ANY PULSE LOWER THAN THE SET
Learn symptoms of battery failure (Bradycardia, dizziness, weakness)
Avoid MRI, ESWL, therapeutic radiation; Large magnets & motors, TENS; Close contact with cell phone; Antitheft devices in stores
Antidysrhythmic drugs
class I: sodium channel blockers: slows the movement of Na into the heart cells | class IA: Quinidine (PO) | Class IB: Lidocaine (IV) | Class IC: Flecainide & Propafenone |
Action | slows impulse conduction; delays repolarization (the reset) | blocks sodium channels to slow conduction; accelerates repolarization | reduce the speed of electrical conduction; dely repo |
effect on EKG rhythm strip | widens QRS, prolongs QT | no change | widen the QRS; prolong the PR interval |
use | MAIN: Atrial fibrillation other: SVT, atrial flutter, sustained VT; Severe malaria | short-term for ventricular dysrhythmias | severe supraventricular dysrhythmias |
adverse effects | Cinchonism (a specific type of poisoning) tox dose: cardiotoxicity | drowsiness, confusion, and paresthesia (tingling) tox dose: seizures or respiratory arrest → need resuscitation equipment | N/V/D can: create new dysrhythmias or make existing ones worse ↓ Contractility → worsen HF |
drug interactions | doubles digoxin levels (so the digoxin dose must be reduced if taken together.) |
Class II: BB | Propranolol (PO) |
action | ↓ SA firing, : ↓ contractility slows down electrical signal as they pass through the AV node |
EKG | prolonged PR interval |
Use | Fast Rhythms: Sinus Tachycardia and Paroxysmal Atrial Tachycardia triggered by emotion or exercise Rate Control: AFib Irritable Beats: severe recurrent VT, exercise-induced rhythms, and frequent PVCs |
AE | Beta1 blockade: HF, AV block, sinus arrest Beta2 blockade: bronchospasm (caution w/ asthma) |
Do NOT use for | sinus bradycardia, high-degree heart block, or existing HF |
Class III: Potassium channel blockers | Amiodarone (PO) | Amiodarone (IV) |
Action | Delays repolarization by blocking potassium channels | Slows AV conduction and prolongs AV refractoriness |
EKG changes | QRS widening; prolongs PR & QT intervals | same as PO |
Use | Long-term for recurrent VF and unstable VT | initial treatment/prophylaxis for recurrent VF and unstable VT; used in shock-resistant VF |
AE | Pulmonary toxicity (cough, dyspnea), liver injury, thyroid dysfunction, and vision loss (blindness); don't use in pregnancy or breastfeeding; CNS reactions (dizziness, tremors)—Depo/repo | Hypotension, bradydysrhythmias, and phlebitis (via central line/CVAD) |
drug interactions | Increases levels of digoxin, warfarin, and statins; grapefruit juice increases drug levels; CYP3A4 reduced levels; diuretic prolong QT; BB & CCB excessively ↓ HR | Risk of excessive HR slowing when combined with BB / CCB |
nsg priorities | long half-life (600–2640 hours) stays in the body for months | lifesaving emergency medication in ACLS (bolus followed by infusion) |
Class IV: CCB | Verapamil / Diltiazem |
action | slows SA firing; delays AV node conduction, ↓ contractility |
use | manage AFib, Aflutter; terminate SVT |
AE | cardiac calcium channels: Bradycardia, AV block, HF vascular smooth muscle calcium channels: Hypotension, peripheral edema intestinal smooth muscle calcium channels: Constipation |
digoxin | risk for AV block |
BB | bradycardia, AV block, HF |
Adenosine | Digoxin | Atropine | |
action | ↓ SA node impulses really slows conduction through the AV node | ↓ conduction through AV node; ↓ impulses in SA node ↑ impulses in Purkinje fibers | blocks cardiac muscarinic receptors to directly ↑ HR |
EKG | prolongs PR interval |
| ↑ HR |
Use | primary treatment for terminating Paroxysmal SVT | Atrial Fibrillation, atrial flutter; chronic therapy to prevent the return of SVT INEFFECTIVE: ventricular dysrhythmias | first for symptomatic sinus bradycardia |
AE | Bradycardia, dyspnea, hypotension | cardiotoxicity Other: GI disturbances; CNS responses like fatigue and visual disturbances | tachycardia, dry mouth, and visual impairments |
Nsg consideration | short half-life (1.5–10 sec) given as a rapid IV bolus as close to the heart as possible |