Bone IMS - Cassani
Remember
Correct periosteum, nor periostium
Same with endosteum, not endostium
Bone tissue is a type of connective tissue, together with cartilage they are specialized connective tissue
Is a structural component of the bones
Has a mineralized ECM
Is continously remodelled
Functions of bone tissue
Provide a scaffold for our body
protects some organs
We have insertion of ligaments and tendons in the bone allowing for locomotion
stores minerals, mostly calcium and phosphate
Hematopoiesis happens in the red bone marrow
Site of energy storage - yellow bone marrow, rich and abundant in lipids
Common features among bone and cartilage
cells embeded in ECM
cells trapped within lacunae
have a bilayered connective tissue covering - perisotium supplying it
Differences among bone and cartilage
in cartilage we have perychordium, while in bone we have ostechordium
cells more abundant compared to ECM
the bone tissue is vascularized
higher metabolic rate and better regenerative properties than cartilage
Composition of ECM
Inorganic:
Crystals of hydroxyapatite - calcium and phosphates, their presence is responsible for rigidity and stiffness, also storage of minerals
Organic (35%):
mainly composed by collagen fibers:
mostly type I
but also type V present
proteoglycans
assembled in
multiadhesive proteins
stabilise the structure of ECM
Most different is:
osteonoctin
osteopontin
bone specific protein
osteocalcin - binds ca2+ ions, inhibits calcification of blood vessles
growth factoes and cytokines
Without the organic components the bone becomes very fragile
Without the inorganic components the bone becomes noodly
Bone tissue cells
osteogenic cells (osteoprogenitors) - give rise to osteoblasts
line the periostium
located at the surface of the bone
derived from mesenchymal stem cells in bone marrow
the expression of TF Runx2 is crucial for osteoblast differentiation
after knock-out of the gene the osteoblasts are not present in the skeleton
several proteins and enzymes are also required for osteoblast maturation
collagen
alkaline phoshpatase
BMP
Wnt
osteoblasts
synthetise and secrete all the components of ECM
located on the surface of the bone
after secreting ECM most of osteoblasts die, small portion differentiates
look like large polygonal or cuboidal cells
abundant RER and GA and secretory vesicles
Secretory vescicles are especially important during calcification
bone-lining cells
located near osteoblasts
secretory activity can be reaquired when needed
lose the secreting ECM ability
can sense the osteocy
Osteocytes
mature cells of the bone
Osteocytes can regulate the pre-osteoblasts activity
they use mechanosensors
secrete a number of factors to regulate the activity
derived from osteoblasts
trapped in lacunae
They have a globular or flattened body
have dendrytes, which extend on the ECM and allow for contact in between the osteocytes and other cells
have reduced ability to synthetise proteins
osteoclasts
cells responsible for resorbtion of the bone
canaliculi - cavities in which the prolongement of the cells are located
between them are gap junctions,which allows for the exchange of info and molecules
destroy the tissue, during a process called bone remodelling
are derived from the hematopoietic mononuclea cells (GMP)
made from the fusion of different cells
not derived from mesenchymal origin, they derive from cells of hematopoietic origin
when concentration of CA2+ is low in blood, calcitonin is produced stimulating the differentiation of osteoclasts and degradation of the bone, releasing calcium into the blood
osteolasts can be found below
podosomes are a structure that allows osteoclasts to adhere to the bone surface
Osteoclastogenesis
M-CSF acts on receptors in progenitors, which leads to proliferation and differentiation to monocytes and then osteocytes
RANKL - produced mainly by osteoblasts, stroma cells and immune cells, able to act with the receptor determining the differentiation onto osteoclast
Organic components are called osteoid
Mineralisation need to elaborate
We can distinguish 3 states of the osteocytes
quiescent
very little cytoplasm around nucleus
GA and RER low in abundance
formative
characterised by the central position at the basal part of the nucleus in the cells
cells usually aquire the ability to secrete
resorptive
increased GA and RER occupying most of the volume of the cells
cells able to secrete things into the ECM
There are 3 specialize membrane domains
Ruffled border- formed at the level of the cells, by microvilli like processes, where bone resorption happens
sealing zone/clear zone
corresponds to the area of the membrane that firmly attaches to the tissue,
devoid of organells
basolateral region
exocytosis happens of digested materials into the blood
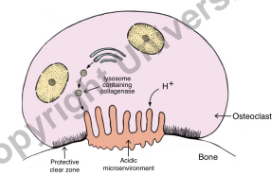
Bone resorption
starts the deminoralisation of the bone occurs
at the ruffle border pH decreases
this dissolved the crystals
release of calcium and phosphate
Resorption lacunae also called Howship lacunae
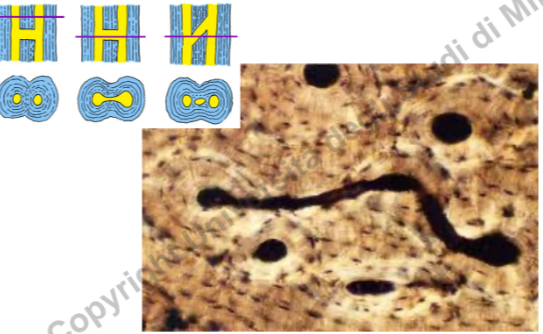
TRAP Staining
TRAP staining stands for tartrate-resistant acid phosphatase staining.
It is a histological staining technique used to identify and visualize osteoclasts, which are cells responsible for bone resorption.
Osteoclasts contain high levels of tartrate-resistant acid phosphatase (TRAP) enzyme, which is the target of this staining method.
TRAP staining is commonly used in bone research and pathology to study bone remodeling, osteoporosis, and other bone-related diseases.
The staining procedure involves the use of a TRAP-specific substrate that reacts with the TRAP enzyme present in osteoclasts.
The substrate is usually a diazonium salt, which forms a colored precipitate upon reaction with TRAP.
The stained osteoclasts appear as dark purple or red cells under a microscope, allowing for their identification and quantification.
TRAP staining can be performed on tissue sections or cultured cells, depending on the experimental setup.
The staining results can be further analyzed using image analysis software to measure osteoclast number, size, and activity.
TRAP staining is often combined with other staining techniques, such as hematoxylin and eosin staining, to provide additional information about the bone tissue and surrounding cells.
Overall, TRAP staining is a valuable tool in bone research, providing insights into osteoclast biology and the pathogenesis of bone diseases.
If the osteoclast activity is increased the pathologies may occur
osteoporosis
Paget disease of the bone
first phase of significatn reduction of bone density
followed by dramatic deposition of bone mass
results in bone deformities
rheumatoid arthritis
autoimmune disease
If the osteoclast activity is decreased the pathologies may occur:
osteopetrosis
opposite to osteoporosis
huge increase in bone mass
May be hereditary:
Autosomal recessive osteopetrosis (ARO)
reduced osteoclast activity
no cure and therapy
main defects:
bone defects
increase in the mass of the bone
hematological defects
neurological defects
there are types of ARO
osteoclast-poor - osteoclasts are very few
due to genetic defects in the RANK and RANKL genes
osteoclast-rich - osteoclasts are present
HSCT in RANKL-dependent ARO
Types of bones
long bones
middle portion shaft - diaphysis
two ends - epiphysis
short bones
flat bones
irregular bones
Bone classification
sponge bone (cancellous bone)
made by traveculae
spaces occupied by blood vessels and bone marrow
compact bone
the outer layer of the bone
higher bone mass
Long bone structure:
diaphysis
eppiphysis x2
sometimes on the surface cartilage may occur
inside the diaphysis is a cavity,through which goes
bone marrow
blood vessels
covered on the external surface by periosteum
the cavities are covered by connective tissue called endosteum
Blood supply of the long bone
arteries enter the bone at the level of diaphysis through foramina
they divide forming a network of blood vessels
Bone membranes
periosteum
dense regular connective tissue
outer layer - more fibrous
inner layer - whith osteogenic layer
rich in blood vessels and nerves, also lymphatic
this is as far as lymphatic system goes
bound to the bone through Sharpey’s fibers
endosteum
thinner thatn periosteum
possess osteogeneic cells
Bone marrow cavity
red bone marrow
hematopoietic place
yellow bone marrow
rich in fat droplets
Microscopic mineralised bone
Woven bone (immature)
turns into lamellar bone
contains high amount of cells per volume copared to the mature bone
randomly distributed cells
less strong bone than the lamellar bone
Lamellar bone (mature)
composed by structural units called osteon
a system of circular lamellae
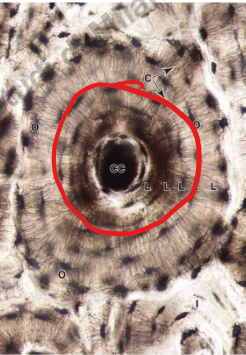 jak słoje drzewa
jak słoje drzewainside is the Haversian cannal
inside tha cannal are blood vessels and nerves
the system is also called Haversian system
Volkmann cannal
connect 2 Haversian cannals
Lamellae system
osteon
outer circuferential lamellae
located in the most peripheral part of the bone
just below periosteum
internal circumferential lamellae
line the medullary cavity
interstitial lamellae
located in between osteons
derived from remodelling of the previous osteons
How the development of the new osteon occurs
in the beginning a resorption cavity is formed
a long circular cavity, like a tunnel
blood vessels and surrounding tissue occupies the cannal
osteoblasts are formed and multiply forming a bone
we can differentiate a new bone cone and a resorption cone
Spongy bone
made by irregular lamellae
don’t have Haversian cannal and so the moelcules are supplied through the cavities
Ossification
intramembous ossification (direct)
starts from mesenchyme
mesenchymal cells proliferate and form a small cluster of cells
cells start to differentiate into the progenitors and osteoblast forming a ossification center
They secrete osteoid which traps osteoblasts
the trabecular matrix and peristeum form
endochondral ossification (indirect)
takes place starting from a template of cartilage tissue
at first a bone collar is fomed in the perichondrium region
it’s creation is parallel to initial calification of ECM in cartilage
the calcification makes the cells to become hypertrophic
that causes them to die
at the same time blood vessels make osteoblast progenitors arrive at first ossification center
then a secondary ossification center
Long bone can grow
longitudinal growth
only during puberty
appositional growth
throughout the entire life
Vascular invasion at the level of epiphyseal plate
Bone repair
release of vasodilatation of blood vessels
formation of hematoma
reqruitment of progenitors from the blood
formation of a soft callus
made by cartilage and soft connective tissue
removal of the soft callus
formation of a travecular bone (sponge bone)
remodelling of the bone fragment
deposition of compact bone at the peripheries
Optimum Ca2+ levels in blood - 9-11mg/100ml of blood
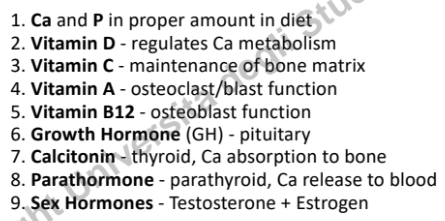
Bone deposition affected by
Ca and P
Vit D
Vit C
Vit A
Vit B12
Growth horone
calcitonin
parathormone
sex hormones