Lecture 2 – Reproductive Tract of Females
Overview of Female Reproductive Organs
the primary organs of the female reproductive system are the ovaries, fallopian tubes, uterus, and vagina.
their functions are tightly coordinated by hormonal signals
the ovaries are paired organs that are responsible for producing oocytes and secreting the key female sex hormones, estrogen and progesterone
the fallopian tubes are muscular tubes that transport the oocyte from the ovary to the uterus
typical site where fertilisation occurs
the uterus is a muscular, pear-shaped organ where a fertilised egg implants and develops into a fetus
provides mechanical protection, nutrition, and waste removal
its powerful contractions are essential for childbirth
the vagina is a muscular canal that receives the penis during intercourse, serves as the passageway for menstrual fluid, and forms the lower part of the birth canal
Anatomy & Support Structures
the organs aren’t rigidly fixed but are suspended within the pelvic cavity by a network of ligaments, which allows for some movement while maintaining their relative positions this is important because the fallopian tubes aren’t directly connected to the ovaries
board ligament
a large, double-layered fold of peritoneum that ‘drapes’ over the uterus and encloses the uterine tubes and ovaries
acts as a primary stabiliser, preventing lateral movement
suspensory ligament
extends from the lateral surface of the ovary to the pelvic wall
contains the ovarian artery and vein, providing the major blood supply to the ovary
ovarian ligament
connects the medial surface of the ovary to the lateral wall of the uterus
uterine ligament
uterosacral, round, cardinal
stabilise the position of the uterus, limiting its range of motion
usually is anteverted position (angled forward over the bladder)
a retroverted uterus (tipped backward) is found in 20–25% of women and is considered a normal variation
The Ovary: Structure and Cycle
the ovary is a small organ with a complex internal structure
general epithelium
a single layer of cuboidal cells covering the surface
tunica albuginea
a layer of dense connective tissue beneath the epithelium
cortex
the outer region containing ovarian follicles at various stages of development
medulla
the central region, consisting of loose connective tissue and blood vessels
The Ovarian Cycle
females are born with their entire lifetime supply of oocytes. these oocytes are arrested in prophase I of meiosis. from puberty to menopause, a cyclical process occurs:
follicle development
waves of primordial follicles are recruited. it takes ~85 days for a follicle to progress from the primordial stage to the point of antrum formation. the stages are:
primordial follicle
oocyte surrounded by a single layer of flattened granulosa cells
primary follicle
oocyte surrounded by a single layer of cuboidal granulosa cells. the oocyte begins to grow
secondary follicle
granulosa cells proliferate to form multiple layers
tertiary follicle
a fluid-filled space called the antrum forms
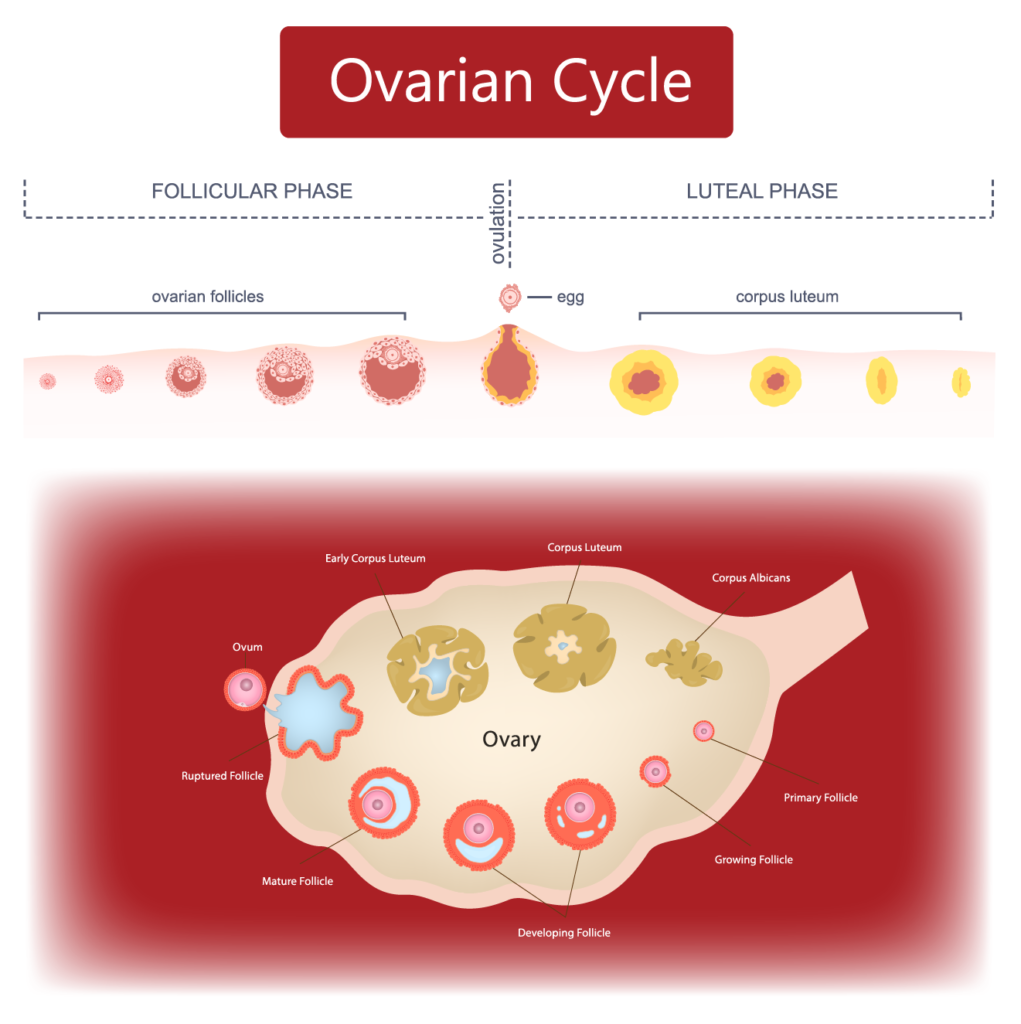
during the follicular phase of each menstrual cycle, a cohort of developing follicles responds to FSH. one follicle is selected to become dominant and continues to mature while the others undergo atresia. this dominant follicle will eventually ovulate
The Uterus: Structure & Cyclic Changes
the non-pregnant uterus is a pear-shaped organ with a small luminal volume. it's wall is composed of three layers:
perimetrium: the outer protective layer
myometrium: the thick middle layer of smooth muscle. it’s responsible for:
proliferative phase: gentle ‘upward’ contractions that may aid sperm transport
secretory phase: ‘downward’ contractions that may aid embryo transport
labour: powerful, coordinated contractions for fetal explusion
endometrium: the inner mucosal layer, which is highly dynamic. it’s subdivided into:
functional zone: the thick, superficial layer that is shed during menstruation if pregnancy doesn’t occur. it’s rich in glands and spiral arteries
basal zone: the thin, deep layer adjacent to the myometrium. it’s not shed and serves to regenerate the functional layer after each menstruation
The Menstruation Cycle
this cycle describes the changes in the endometrium, driven by hormones form the ovary
menstrual phase
if no pregnancy occurs, the corpus luteum degenerates, causing a sharp drop in estrogen and progesterone. the spiral arteries constrict, causing ischemia and necrosis of the functional zone, which is then shed as the menstrual flow
proliferative phase
rising estrogen from the developing dominant follicle stimulates the regeneration and thickening of the functional zone. glands proliferate, and the spiral arteries elongate and become coiled. this phase ends at ovulation
secretory phase
after ovulation, the corpus luteum produces progesterone. this hormone transforms the endometrium, making it secretory. the glands produce a glycogen-rich fluid to nourish a potential embryo. the decidual reaction also occurs during this phase
:max_bytes(150000):strip_icc()/the-menstrual-cycle-3520919-TEXT-FINAL-1-1-d28f721ef9c34f93ac97b55b09114e10.png)
The Decidual Reaction & Window of Implantation
a change in the endometrial stroma where fibroblasts swell and accumulate glycogen and lipids. in humans, this occurs spontaneously during the secretory phase, preparing the ‘soil’ for a potential embryo. in most other mammals, it only occurs after implantation
a short ~48 hour period when the endometrium is receptive to the implanting blastocyst. this receptivity is mediated by the expression of specific adhesion molecules
The Fallopian Tubes: Transport & Fertilisation
the tube is ~13 cm long and has three distinct regions:
infundibulum
the funnel-shaped end with finger-like projections called fimbriae. the fimbriae sweep over the ovary to capture the oocyte after ovulation
ampulla
the longest and widest part. this is the typical site of fertilisation
isthmus
the narrower portion that connects to the uterus
the oocyte/embryo is moved along the tube by a combination of ciliary beating and peristaltic contractions of the smooth muscle wall
The Cervix: Gateway & Barrier
the lower portion of the uterus that projects into the vagina
a critical feature is the change in epithelial type at the squamocolumnar junction
endocervix: lined by a single layer of columnar epithelium
ectocervix: lined by multi-layered squamous epithelium
transition zone: the area where these two meet. this is the site where most cervical cancers arise
functions:
sperm regulation: secretes cervical mucus that changes from thick and impenetrable to thin, watery, and alkaline to facilitate sperm passage
barrier: protects the upper reproductive tract from infection
pregnancy & birth: remains tightly closed during pregnancy to retain the fetus. during labour, it thins and opens to allow passage of the fetus
Ectopic Implantation
implantation of the embryo outside the uterine cavity
the fallopian tube, often due to scarring or damage that impedes the embryo’s transport to the uterus
can occur anywhere in the abdominal cavity, including the ovaries, cervix, or even on the peritoneum, as demonstrated by the remarkable case study of a woman who had an abdominal pregnancy after a hysterectomy
Cervical Cancer & Prevention
almost all cervical cancers are caused by persistent infection with high-risk strains of the HPV, primarily serotypes 16 & 18
screening
the pap smear is a screening tool that collects cells from the transition zone to detect pre-cancerous changes
regular screening every three years can reduce the risk of developing cervical cancer by up to 90%
prevention
HPV vaccines are highly effective at preventing infection with the most common high-risk HPV strains