PROTOZOA
KINGDOM PROTISTA; Subkingdom Protozoa
lowest form of life
pathogenic or nonpathogenic
unicellular, eukaryotic
animal-like protist
no cell wall
2 regions of cytoplasm
ectoplasm (outer)
endoplasm (inner)
at least one nucleus and some several nuclei
some contain vacuoles
w/ special organs for locomotion
wet environment for feeding, locomotion, osmoregulation, and reproduction
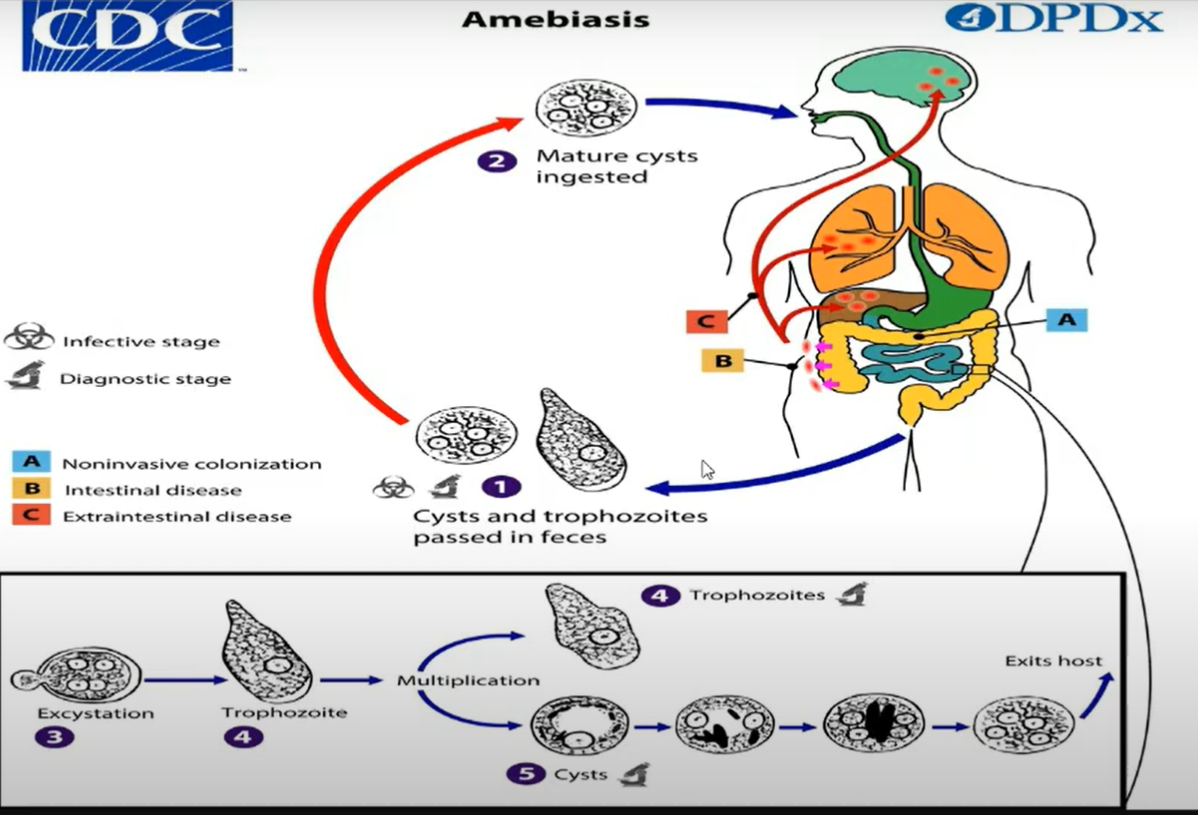
Infective stages:
CYSTS
(diagnostic stage can also be trophozoites)
Vegetative stage:
feeding stage/laagan stage
TROPHOZOITES
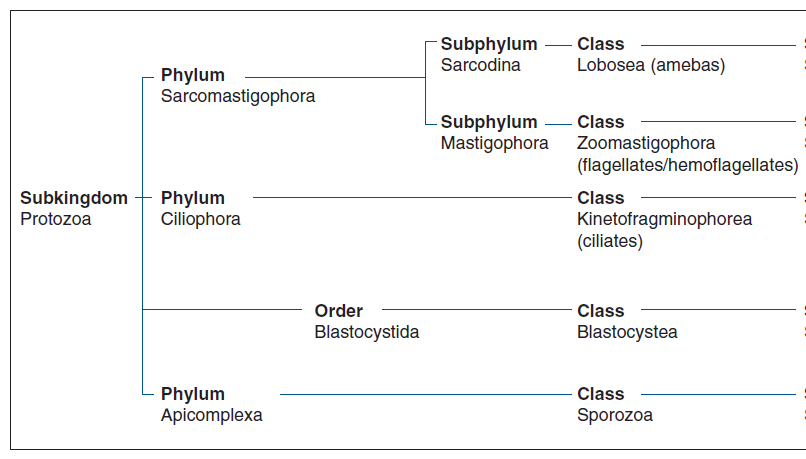
Phylum SARCOMASTIGOPHORA
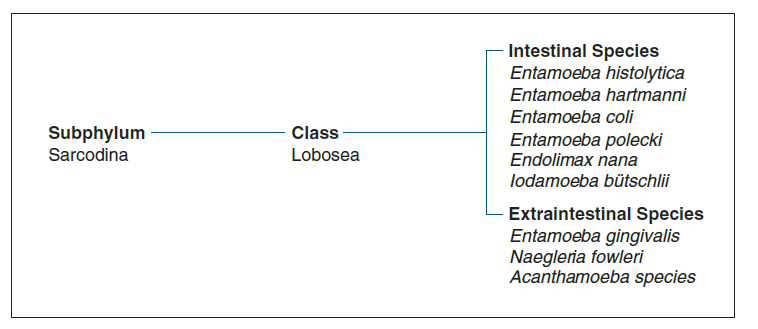
Subphylum SARCODINA
Organ: PSEUDOPODIA (false feet)
Example: AMEBAE
Acanthamoeba castellani
Endolimax nana
Entamoeba coli
ENtamoeba gingivalis
Entamoeba histolytica
Iodamoeba butschlii
Naegleria fowleri
Subphylum MASTIGOPHORA/FLAGELLATA
Organ: FLAGELLA
Example: FLAGELLATES (Giardia. etc.)
Atrial Flagellates
Chilomastix mesnili
Dientamoeba fragilis
Giardia lamblia
Trichomonas hominis
Trichomonas tenax
Trichomonas vaginalis
Hemoflagellates
Leishmania braziliensis
Leishmania donovani
Leishmania tropica
Trypanosoma brucei complex
Trypanosoma cruzi
Phylum CILIOPHORA/CILIATA
Organ: CILIA
Example: Balantidium coli
Phylum APICOMPLEXA
Class SPOROZOA
no definite locomotor organelle
(ex. Plasmodium, Babesia)
Babesia spp.
Cryptosporidium hominis
Cyclospora cayetanensis
Cystoisospora belli
Plasmodium spp.
Toxoplasma gondii
Phylum Microspora
Encephalitozoan
Enterocytozoon
Pleistophora
Nosema
Brachiola
Vittaforma
Trachipleistophora
SARCODINA
RHIZOPODA
have protoplasmic processes or pseudopodia (for locomotion)\
life cycle:
trophozoite stage → precystic stage → cystic stage → metacystic stage
most common means:
fecal-oral route
ingestion of infective cyst in contaminated food or water
w/ cystic stage and inhabits large intestine except for Entamoeba gingivalis
all commensals except for Entamoeba histolytica
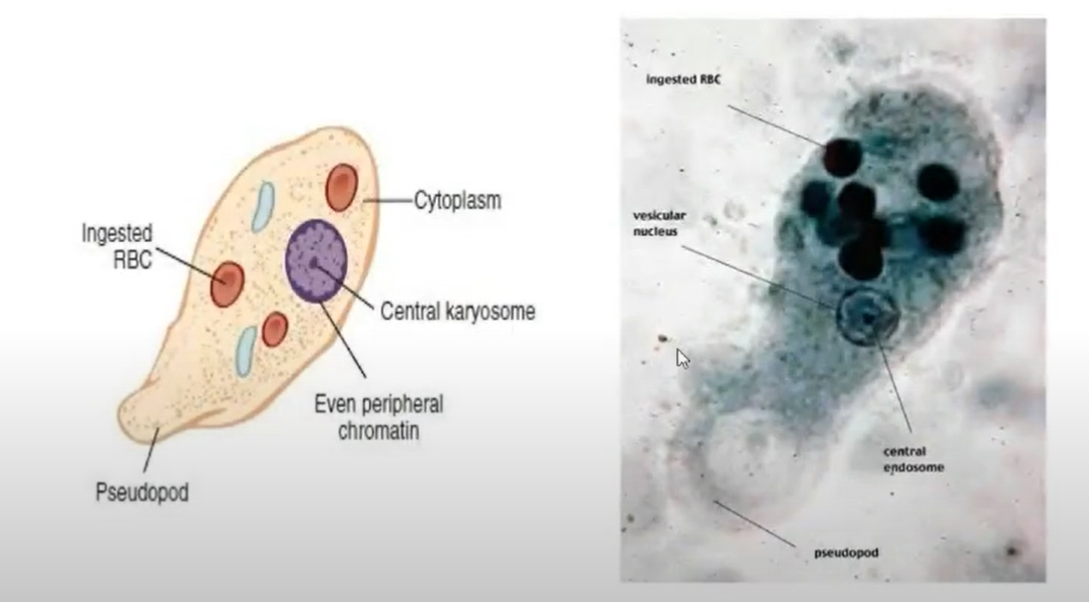
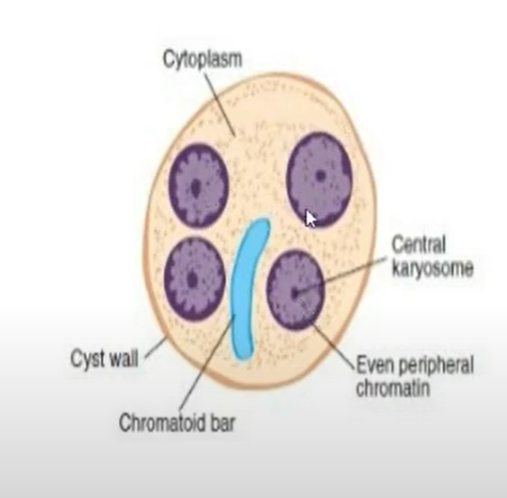
AMOEBIC NUCLEAR STRUCTURES
used for identification of amoebas; both cysts and tropphozoites
Karyosome
karyosomal chromatin
small, central mass of chromatin in the nucleus
Peripheral chromatin
chromatin material surrounding the karyosome
Chromatoid bars/ chromatoidal bodies
(not in trophozoites)
unorganized chromatin material that transforms into squared or round-ended structures
usually in young cysts
Glycogen mass
(not in trophozoites)
cytoplasmic area without defined borders that is believed to represent stored food
found in young cysts
LIFE CYCLE
similar to intestinal amebas
MOT:
ingestion of infective cysts in contaminated food or water
Trophozoites:
susceptible to environment outside host and are not usually transmitted to humans\
2 processes:
excystation
morphologic conversion from the cyst to the trophozoite in the ileocecal area of the intestine
(favorable environment)
encystation
conversion of trophozoites to cysts when environment becomes unacceptable for continued trophozoite multiplication
Morphology
CYSTS
non-motile
non-feeding stage
INFECTIVE STAGE
frequently found in formed stools
may be studied in fresh condition by staining (DFS) with D’Antoni’s Iodine stain (iodine can kill trophozoites), but more satisfactory method is to stain permanent preparation with iron hematoxylin (or trichrome)
TROPHOZOITES
motile
feeding stage
VEGETATIVE stage
found in diarrheal and liquid stools (wet environment)
ameba excreted as trophozoites cannot mature to cysts
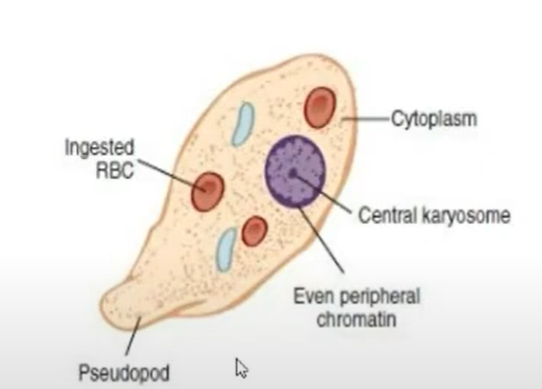 pseudopods: locomotory organelle
pseudopods: locomotory organelle
Ameba spp. (genus)
Entamoeba
true ameba
peripheral chromatin
visible nuclear membrane in both trophozoite and cyst
chromatoidal bodies
in cysts only
Endolimax or Iodamoeba
other ameba
neither possess peripheral chromatin nor chromatoidal bodies
Entamoeba histolytica
described by Losch after being isolated in Russia from a patient with dysenteric stools
ONLY PATHOGENIC INTESTINAL AMEBA
can spread to other organs
IS:
Mature quadrinucleate cyst
MOT:
Ingestion of food or water contaminated with the cysts
Pathogenesis:
ability to directly lyse host cells and cause tissue destruction
amoebic lesions show evidence of cell lysis, tissue necrosis, and damage to the extracellular matrix
trophozoites interact with the host through a series of steps:
adhesion to the target cell
phagocytosis
cytopathic effect
invasive strains of E. histolytica are resistant to compliment-mediated lysis
Compliment systems (C3)
Key virulence factors:
cysteine proteases
amebapore
Gal/GalNac lectin
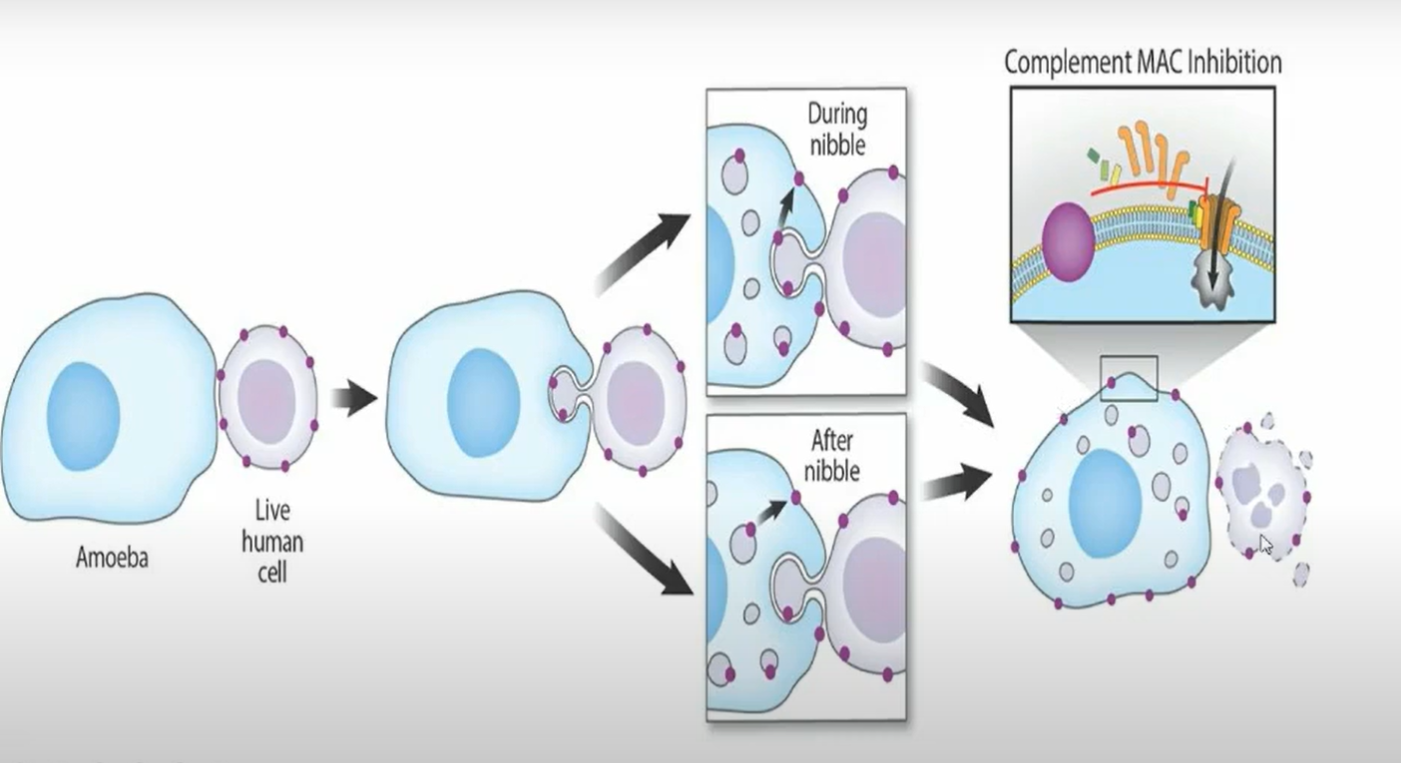 TROGOCYTOSIS (nibbling)
TROGOCYTOSIS (nibbling)
Spectrum of disease:
asymptomatic infection
negative or weak antibody titer
cysts may be detected during routine O&P examination
Incubation time:
varies but normally ranges from 1-4 weeks
Invasive INTESTINAL AMEBIASIS, generally acute:
amoebic diarrhea without dysentery
90%b of the cases
Blood-tinged mucus in stool (up to 10 per day)
dysentery or colitis
ulceration on the walls of the intestines
abdominal cramping
anorexia
fatigue
diarrhea
ameboma (amebic granuloma)
granulomatous pseudotumoral growth (develop on intestinal wall; tumor)
may be mistaken for a malignant tumor
ulcer
flask-shaped in cross section with mouth and neck being narrow and base large and rounded
confluent ulceration and necrosis of colon
amoebic liver abscess
EXTRAINTESTINAL AMEBIASIS
Hepatic involvement
liver is the most common location
most common extraintestinal complication of amebiasis
center of abscess contains thick chocolate brown pus (anchovy sauce pus)
liquified necrotic liver tissue
Amebic liver abscess
abdominal pain in upper right quadrant area and tenderness in the liver area
presence of leukocytosis
high ALP levels
elevated right diaphragm
Pulmonary amebiasis
from liver to lungs (hepatobronchial fistula)
usually very rarely
results with expectoration of chocolate brown sputum
involvement of the CNS leads to Secondary Amebic Meningoencephalitis
Primary Meningoencephalitis (Naegleria fowleri)
prepuce and plans are affected in penile amoebiasis which is acquired through anal intercourse
ulceration on the head or foreskin of the penis
DIAGNOSIS
Standard O&P examination
recommended procedure for recovery and identification of E. histolytica in stool specimens
Sigmoidoscopy specimens
at least six areas of the mucosa must be sampled
permanent stained smears should be made
Liver abscess (aspiration)
definitive diagnosis is made through identification of organisms from liver aspirate material
Culture
not routinely performed
Culture media:
Boeck and Drbohlav media
NIH polygenic media
Craig’s medium
Nelson’s medium
Robinson’s medium
TYI-S-33 medium (specific for E. histolytica)
Serological testing
rarely recommended unless the patient has true dysentery
much more relevant for patients suspected of having extraintestinal amebioasis
include:
Indirect Hemagglutination Test (IHA)
serum with antibody titer of
Indirect Fluorescent Antibody Test
serum with antibody titer of
lates Agglutination Test
Enzyme-linked Immunoabsorbent Assay (greater sensitivity)
RIDASCREEN Entamoeba histolytica
detects IgG antibodies
ProSpecT Entamoeba histolytica microplate assay
detects E. histolytica specific antigens (EHSA) in human fecal samples
E. histolytica II test
fecal antigen test (detects E. histolytica adhesin)
SREHP serine-rich E. histolytica protein and galctose-specific adhesin
Histology
histologic diagnosis can be made when the trophozoites within the tissue are identified
periodic acid-schiff staining is often used to help locate the organisms
the organisms appear bright pink with a green-blue background
CYSTS MORPHOLOGY
Entamoeba histolytica vs. Entamoeba coli
Entamoeba histolytica
10-20 microns (usually, 12-15 microns)
Coffin-shaped chromatoidal bars
Mature cyst with 4 nuclei
Peripheral chromatin
fine, uniform granules, evenly distributed
Karyosome
small, compact, usually centrally located
Glycogen
diffuse, may be absent in mature cyst
Entamoeba coli
10-35 microns (usually, 15-25 microns)
splinter-like chromatoidal bars
mature cyst with 8 nuclei
Peripheral chromatin
coarsely granular, may be clumped and unevenly arranged
Karyosome
large, may or may not be compact and/or eccentric
Glycogen
diffuse, may be absent in mature cysts

CYSTS MORPHOLOGY
Entamoeba histolytica vs. Entamoeba coli
Entamoeba histolytica
12-60 microns (15-20 microns)
moves in one direction (unidirectional)
only one pseudopod trusted out in explosive manner
Pseudopods trusted out in an explosive manner
Endoplasm
contains RBCs but no bacteria or cell detritus
Nucleus
not visible when stained
consists of thin nuclear membrane with layer of uniformly sized fine chromatin granules distributed along inside border of nuclear membrane
finely granular/ground glass appearance
karyosome
fine, centrally located
can occur free in lumen of the intestine as a commensal and is known as its minuta form
Entamoeba coli
15-50 microns (20-25 microns)
moves in several directions at the same time
sends out several pseudopods at the same time
pseudopods trusted out slowly
Endoplasm
contain bacteria, yeasts, and cell detritus
stained nucleus contains a thicker nuclear membrane with layer of variously sized chromatin granules unevenly distributed along the inside border of nuclear membrane
Karyosome:
large, eccentrically located