Cranial Nerves, Sensation, and Pathways
Vocabulary:
Cranial nerve: Can be sensory, motor, or mixed. Organized into 12, each named and with a roman numeral based on rostral/caudal connection to the brain
Sensory: Synapse in the brain
Motor: Have cell bodies in the brainstem
Transduction: How a signal is converted, a stimulus energy is converted into electrical signals
Encoding: The process of conveying information abut a stimulus’s characteristics, like nature and intensity. Includes labeled lines, population encoding, and AP frequency
Labeled line: The path a signal takes from receptor to cortex, indicates the nature of the stimulus
Population encoding: The integration of multiple signals required to identify nature of stimulus. Patterns of neuronal activation
Perception: The conscious awareness of sensation, for all sensations except olfaction things have to synapse in the thalamus to do this
Sensation: Comprised of stimuli, receptors, central pathways, and cortical processing
Special sensation: Requires an organ with supporting cells for the transducing cells. Include vision, audition, vestibular, and chemical (olfaction/gustation)
Somatosensation: General sensation, like touch. Due to pressure, tension, or stretch. Leads to proprioception. Also includes nociception and thermosensation. Detects mechanical stimuli, extreme temperatures
Proprioception: Our sense of where we are in space, axons have the widest diameter as signals need incredibly fast transmission
Nociception: Pain sense due to mechanical stimuli, extreme temperature, or chemicals. Happens when something is potentially damaging
Crude touch: Travels with temperature/nociception
Fine touch: Doesn’t travel with crude touch
Receptor potential: Occurs with receptors for stimuli located in epithelial cells, occur when receptors can “generate” APs. Stimulus strength reflected in the magnitude of potentials, weak stimuli don’t get encoded but stronger stimuli are encoded with many APs. Receptors can additionally adapt to the stimulus to stop sending APs
Tonic receptors: Slowly adapting, give spatial information. Detailed information
Phasic receptors: Rapidly adapting, give temporal information and information about changes in ongoing stimuli
GPCRs: Used within receptors to transduce stimuli, including specialized epithelial cells, free nerve endings, and encapsulated nerve endings
Free nerve ending: Dendrite ends with no specialized other surrounding cells or coatings
Protein channels: Used within receptors to transduce stimuli, including specialized epithelial cells, free nerve endings, and encapsulated nerve endings
CNS: Gets input about a stimuli’s location, physical characteristics, and onset/offset (where, what, when)
Pseudounipolar neuron pathway: Pseudounipolar neurons synapse in the CNS (separate from face and rest of body entering CNS). Found in all tactile receptors
1st order neuron: The first neuron that a sense travels through, synapses in the spinal cord ganglia
2nd order neuron: Neuron that carries sensation from the spinal cord to the CNS
3rd order neuron: Carries information in the CNS to the cortex for conscious perception
Spinal nerves: How non-facial sensations enter the CNS, each carries information from distinct areas. Loss of sensation can indicate level of spinal cord injury. Spinal cord divided into regions based on vertebrae anatomy
Cervical: 8 of them
Thoracic: 12 of them
Lumbar: 5 of them
Coccygeal: 1 of it
Dermatome: Describes how information enters the spinal nerves and CNS from distinct areas, one area is the dermatome for a given neuron’s dendrites
Receptive field: The physical region something corresponds to, smaller receptive fields yield more precise location
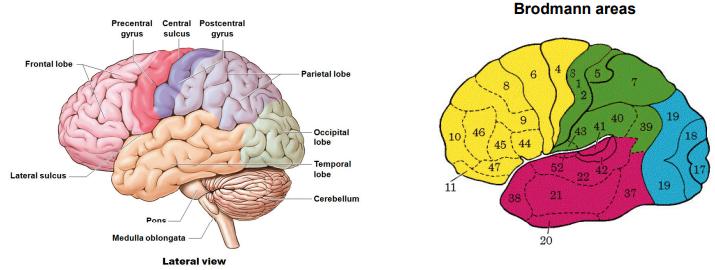
Postcentral gyrus (S1): In the parietal lobe, receives conscious somatosensations, thermosensations, and proprioception. Can also discriminate aspects of nociception. Acts as the primary somatosensory cortex, has Brodmann areas 3, 2, and 1 that reflect histologically similar areas with similar functions
Central sulcus: Where all conscious somatosensory pathways end up, within S1
Spinal cord (know locations)
White matter: High in axon density (myelin is white).
Dorsal/posterior columns: Fasciculus gracilis (lower body) and fasciculus cuneatus (upper body). Have A-beta fibers to discriminate touch, pressure, and vibration
Anterior/ventral and posterior/dorsal spinocerebellar tracts: Unconscious proprioception from lower body from type I and II fivers (A-alpha), muscle spindles, go to cerebellum
Anterolateral system: For nociception, temperature, itch, and non-discriminative touch from A-delta and C fibers. A-delta for cold and C for warm. Unmyelinated ascending
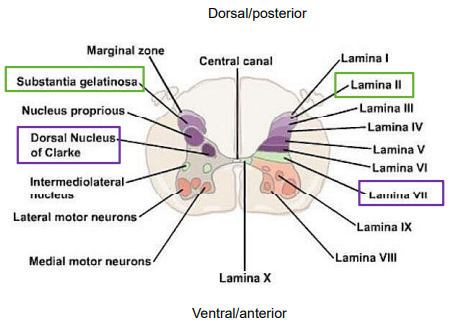
Gray matter: Histologically divided into Rexed’s laminae (know where)
Substantia gelatinosa
Lamina II
Lamina VII
Dorsal Nucleus of Clarke
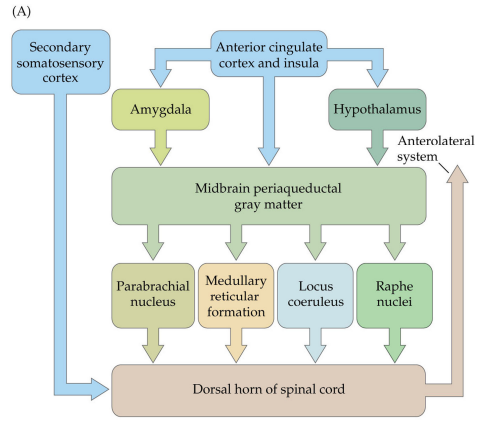
Periaqueductal gray (PAG): Along with endocannabinoids, can produce analgesia. Noxious stimuli here increase endocannabinoid amounts
Midbrain: Develops from the mesencephalon
Gate theory of pain: The flow of nociceptive information is that the dorsal horn modulates activation of low threshold mechanoreceptors, basis of “scrambler therapy” that stimulates nearby dermatomes. Flow of ascending pain information is modified by stimulation of LTMRs
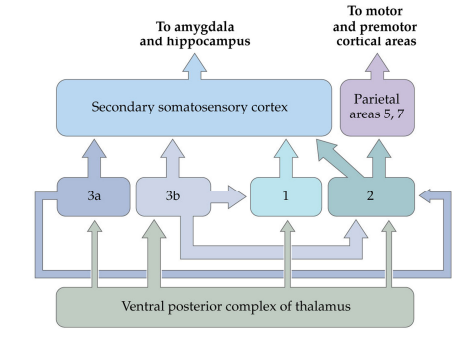
Somatic sensory cortex: VPL and VPM project to layer 4 of S1, different types of information go to different areas, sensations to area 2, proprioception to 3a (travel mostly A-alpha), and somatosensations to 3b (travel mostly A-beta) and 1. Information is segregated by origin. Displays plasticity, if a digit is amputated, regions specialized to process one sense will shift (observed via cortical mapping). Layer 5 is the main output layer
Peripheral hyperalgesia: Lower threshold for pain perceptions, peripherally there is inflammatory soup including products of tissue damage, immune cells, and axon collateral terminals. These released substances bind to nociceptors and ion channels of nociceptive fibers. They include neurotransmitters like substance P and calcitonin gene-related peptide (CGRP), cytokines like IL-1beta TNFalpha and activate the MAP kinase pathway (increasing Na+ channel activity), and prostaglandins that have their synthesis stimulated by bradykinin and requiring COX and blocked by NSAIDs like aspirin/ibuprofen. Prostaglandins phosphorylate TTX-resistant Na+ channels to enhance APs in C fibers
Central sensitization: Rapid onset, high nociceptor activity, decreases the threshold of the dorsal horn neurons (secondary hyperalgesia), displays allodynia (generalization to nonpainful stimuli)
Central pain modulation sensitization: During build up there is increased discharge dorsal horn neurons, due to summation of slow synaptic potentials, build up of Ca2+ in NDMA channels, and opening of voltage-dependent L-type calcium channels. This is perceived as intensity of low frequency, identical stimuli become more painful. This only lasts during the time of stimulation. There is LTP-like enhancement of post synaptic neurons (NMDA dependent Ca2+ increase in second order neurons), reduced GABA inhibition in second order neurons (due to K/Cl transport, and GABA depolarizing instead), microglia releasing proinflammatory cytokines (IL-1B to decrease threshold and TNFalpha to enhance excitatory transmission and decrease inhibition), and astrocytes releasing cytokines
Neuropathic pain: Maladaptive plasticity is associated with remodeling, in terms of receptive field expansion, lowered threshold for central neurons, and recruitment of non-nociceptive fibers. There is demyelination of axonopathy peripheral or central somatosensory pathway. This can happen spontaneously, due to a mild stimulus, or disease like diabetes, shingles, AIDS, MS, trauma, or stroke. There are also burning sensations interrupted by bouts of shooting/stabbing, electric-shock jolts
Pain perception: Context dependent, injured soldiers often feel little pain, also susceptible to the placebo effect
Spinal cord lesions: Can lead to dissociated sensory loss, with contralateral pain, temperature, and non-discriminative touch loss a couple segments below the lesion. There is ipsilateral pain, temperature, non-discriminative touch at the level of the lesion, and ipsilateral discriminative touch and pressure loss below the level of the lesion.
Discriminatory path: First order pseudounipolar neurons synapse onto second order neurons in the CNS, dorsal horn of the spinal cord to nuclei in the brainstem. Information, to be perceived, must decussate (cross sides) and synapse from the second order neuron to the thalamus. Third order neuron synapses in the contralateral postcentral gyrus (S1), somatosensory pathway
Dorsal column-medial lemniscus path: Central branches of the first order pseudounipolar neurons enter the spinal cord and ascend to dorsal (posterior) columns. In fasciculus cuneatus, only above T6 and lateral to fasciculus gracili (lower body). Lower body information enters first, so it is more medial than upper body information. The first order neurons synapse on dorsal column nuclei in caudal medulla, the gracile nucleus and cuneate nucleus, LTMR with A-beta fibers, central “Non-face” pathway. From the gracile to cuneate nuclei, second order neurons travel as internal arcuate fibers, that decussate to become medial lemniscus (same axons contralaterally) and synapse in the nuclei of the ventral posterior lateral (VPL) in the thalamus. They finally synapse in S1, with lower body medial and upper body lateral (face out) information. When dysfunctional, two point discrimination thresholds are increased and there is impaired ability to identify objects by touch alone
Trigeminothalamic system: LTMR with A-beta fibers, central pathway carrying face information. Sensory (first order) neurons travel in CN V to the pons with cell bodies that form the trigeminal ganglia, the principal nucleus of the trigeminal complex of the pons. Second order neurons decussate and travel in the trigeminal lemniscus to the ventral posterior medial nuclei of the thalamus (VPM). Third order neurons travel in the internal capsule to most lateral areas of the postcentral gyrus
Proprioception pathway: Multiple paths, though targets the primary somatosensory cortex (conscious), also targets the cerebellum (unconscious)
Conscious: Targets S1 (same as discriminatory) in a 3 neuron path synapsing in the thalamus contralateral to S1. First order neurons of muscle spindles and GTOs follow dorsal column-medial lemniscus path. Lower body, first order neurons ascent gracile fasciculus to synapse gracile nucleus. Upper body first order neurons ascent cuneate fasciculus to synapse in the cuneate nucleus. Second order neurons travel as internal arcuate fibers before decussating, then travelling in the medial lemniscus and synapsing in the VPL nucleus of the thalamus (distinct from discriminative touch synapses). Third order neurons ascend in internal capsules and synapse in S1
Unconscious: In a 2 neuron path with no thalamic synapses. In the ipsilateral cerebellum. Body source wise,
Lower body enters via spinal nerves T1 or below, and upper body enters via cervical spinal nerves. First order neurons of muscle spindles and golgi tendon organs for the lower body synapse Clarke’s nucleus (Lamina VII, in dorsal horn), second order neurons form dorsal spinocerebellar tract.
Upper body: A-alpha and A-beta, first order neurons of muscle spindles and Golgi tendon organs travel via fasciculus cuneatus to synapse external cuneate nucleus, where secondary neurons form the cuneocerebellar tract (only in brain stem, not spinal cord)
Both: Upper and lower body collaterals ascend/descent and synapse in ventral horns for reflexes. Ventral/anterior spinocerebellar tracts to enter the cerebellum via superior cerebellar peduncle with decussates (double decussation), then synapse in cerebellum on the same side as the stimulus
Lower: Golgi tendon organs and type II fibers of muscle fibers, the first order neurons synapse in the dorsal horn, second order neurons decussate and travel in ventral/anterior spinocerebellar tracts to enter the cerebellum via superior cerebellar peduncle with decussates (double decussation), then synapse in cerebellum on the same side as the stimulus
Face: First order neurons synapse in the mesencephalic trigeminal nucleus of the trigeminal complex via CN V, eventually reaching the thalamus and somatic sensory cortices, part of reflexive chewing. Trigeminal nerve → pons, ascends the midbrain and synapses in the mesencephalic nucleus trigeminal complex. From here, the second order neuron decussates to synapse in the VPM nucleus. Then the third order neuron is in an internal capsule to the primary somatosensory cortex
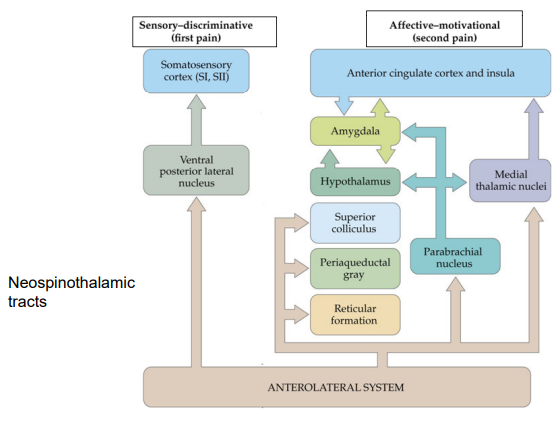
Nociception pathway: Anterior cingulate cortex, S1, and S2 may be involved
Neospinothalamic: Travel in A-delta fibers laterally, first order neurons enter via dorsal root. Branches ascend and descend several segments in Lissauer’s tract. Synapse on second order neurons in the dorsal horn, like Rexed’s lamina I and lamina V with wide-dynamic range neurons (also get pain from internal organs, maybe possible for refered pain). Second order neurons decussate and ascent contralateral neospinothalamic trans to synapse the VPL nuclei of the thalamus. Third order neurons synapse of the primary somatosensory cortex via internal capsule. Contralateral in brain to side of nociception in the body, decussates in the spinal cord
Facial: Uses A-delta fibers, enter the pons via CN V. Descend ipsilaterally in the spinal trigeminal tract and synapse the spinal nucleus of the trigeminal complex in the medulla. Second order neurons decussate in the medulla and ascend the trigeminothalamic tract, to synapse VPM nucleus of thalamus. Third order neurons synapse in the lateral S1
Affective/motivational: Non-discriminative, uses C fibers that synapse in lamina I, lamina II, and lamina V. This follows substantia gelatinosa. Interneurons from lamina II project diffusely other laminae, polysynaptic pathways arise in lamina V. Postsynaptic neurons decussate before ascending anterolateral system, of the paleospinothalamic spinoreticular and spinomesencephalic tracts. For targets, reticular formation = autonomic responses (cardiovascular and breathing), periaqueductal gray = pain modulation, superior colliculus = multisensory integration and orienting reflexive responses, hypothalamus = activation of sympathetic division of visceral motor system and neuroendocrine responses, amygdala = fear, parabrachial nucleus = relay station, insula = perception and modulation
Types of sensory receptors:
Fine touch: Discriminate to touch, pressure, and vibration. Low-threshold mechanoreceptors (LTMRs), mostly on peripheral ends of pseudounipolar A-beta fibers
Crude touch: Non-discriminate to crude/affective touch, pain, and thermosensations, on free nerve endings and A-delta (small diameter and lightly myelinated) or type C (unmyelinated) fibers. Higher threshold for APs. Adaption speed varies, large receptive fields. Not found on fingertips and palms
Root hair plexus: Have different arrangements of pseudounipolar free nerve endings surrounded by 3 types of hair follicles. Have A-beta, A-delta, and C fibers. Rapidly adapting with low thresholds, detect hair movement. Bending of the hair excites the cells surrounding it
Mechanoreceptor afferents: Ionotropic, respond to touch/pressure/stretch/vibration. Na+ enters to create generator/receptor potential. If threshold is reached, AP travels through peripheral and central branches of the neuron
Proprioceptors: Detect mechanical stimuli within the body itself. Interoreceptors, LTMRs, found in muscle spindles, golgi tendon organs, and joint receptors. In the heart, blood vessels they are part of the visceral sensorimotor system
Muscle spindles: 4-8 intrafusal muscle fibers surrounded by connective tissue, have free nerve endings coiled around the center. Stretch when the muscle contracts and opens piezo2 channels. Low threshold, with rate of change being Ia (A-alpha) afferent rapidly adapting and static length being II (A-beta) afferents slowly adapting. Gamma motor neurons innervate intrafusal fibers and contract to maintain sensitivity
Golgi tendon organs: Signal changes in muscle tension, formed by branches Ib afferents woven in collaged. Slowly adapting, high threshold. Have piezo2 channels opened by tension in collagen fibers
Tactile receptors: For discriminative touch/pressure/vibration
Merkel cell-neurite complex (tactile disk): Release glutamate to depolarize a neuron (A-beta fibers), LTMRs. In the epidermis, concentrated in glabrous skin, enrich fingertips, sparse in hairy skin around root hair plexus. Slow adapting, have piezo2 channels, most sensitive,
Meissner corpuscle (tactile corpuscle): LMTRs, only in glabrous skin. Enriched in fingertips, also found in dermis. Covered by lamellated Schwann cells, lower threshold for AP generation than Merkel cells. Rapidly adapting, have small receptive fields (larger than Merkel cells), have piezo2 channels
Ruffini (bulbous) corpuscle: Found in hairy and glabrous skin, throughout the dermis. Encapsulated by collagen fibers, entwined with free nerve endings. Detect stretch of skin, slow adapting, broadest receptive field
Pacinian (lamellated) corpuscle: In hairy and glabrous skin, especially hand and feet. Found in the deep dermis, lamellated free nerve endings. Detect vibration and are rapidly adapting, broad receptive field
Thermosensation: Cold use A-delta fibers, warm use C fibers, and TRP channels are permeable to Na+ and Ca2+
Nociceptors: Free pseudounipolar nerve endings categorized by axon type. Anesthetized based on type
A-delta fibers: Lightly myelinated, for sharp pain, higher threshold that A-alpha and A-beta. Different types are more sensitive to particular modalities of pain
C fibers: Unmyelinated, signals less than 2 m/s. Diffuse, delayed, longer acting pain like aching and burning. Higher threshold than A-delta, polymodal for all modalities. Involved in paleospinothalamic tract, spinoreticular tract, and spinomesencephalic tract. Achy pain
Piezo2: For mechanical stimuli
Acid-sensing ion channels (ASIC): For chemical stimuli, like proton-gated channels permeable to Na+
Transient receptor potential family (TRP): Mechanical, chemical, and thermal stimuli. Permeable to cations
Pruritus receptor: For itch, free unipolar nerve endings, A-delta fibers and C fibers
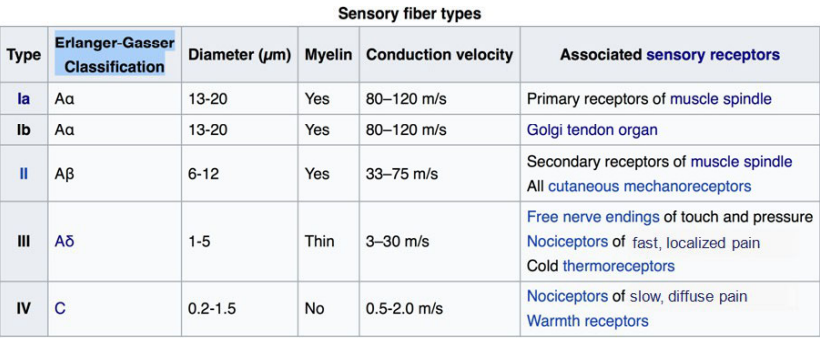
Sensory Fiber types:
Free pseudounipolar nerve endings:
A-alpha (Ia + Ib): Widest diameter
A-beta (II): Root hair plexus, pruritus. Tactile, slightly slower transmission than more heavily myelinated and wider A-alpha fibers, encapsulated (modified by ECM). Have lower thresholds for AP generation than free nerve endings
A-delta (III): For crude touch, root hair plexus, cold temperature, fast/discriminate nociception, pruritus. Narrow and not much myelination
Type C (IV): Unmyelinated, for crude touch, root hair plexus, warm temperature, slow/diffused nociception, pruritus
The Nerves:
Olfactory I: Sensory, for sense of smell
Optic II: Sensory, for vision
Oculomotor III: Motor, for eye movements, pupillary constriction and accommodation, muscle of upper eyelid
Trochlear IV: Motor, for eye movements like intorsion or downward gaze
Trigeminal V: Sensory and Motor, for somatic sensations from the face, mouth, cornea, and muscles of mastication
Abducens VI: Motor, for eye movements like abduction and lateral
Facial VII: Sensory and motor, controls the muscles of facial expression, like taste from the anterior tongue, and lacrimal and salivary glands
Vestibulocochlear VIII: Sensory, For hearing and sense of balance
Glossopharyngeal IX: Sensory and motor, for sensation from the posterior tongue and pharynx, taste from the posterior tongue, carotid baroreceptors and chemoreceptors, salivary gland
Vagus X: Sensory and motor, for autonomic functions of the gut, cardiac inhibition, sensation from the larynx and pharynx, muscles of vocal cords, swallowing
Spinal accessory XI: Motor, for the shoulder and neck muscles
Hypoglossal XII: For tongue movements
Overall, the body uses the anterolateral system with nociceptive signals, and the face uses spinal trigeminal tract and trigeminothalamic tract with nociceptive signals
Wkst 12/13: CDAAB DB(A?)CC CCCAA ADADA