Insulin Dosing
1. Components of an Insulin Regimen
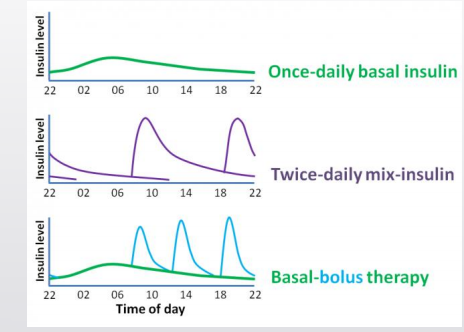
Insulin regimens mimic (or fail to mimic) the way a healthy pancreas delivers insulin. A pancreas provides:
Basal insulin - continuous, low-level insulin secretion (day and night to control hepatic glucose release, especially overnight).
Goal: smooth background effect, ideally no peaks.
Examples: glargine (Lantus, Toujeo, Semglee, Basaglar), detemir (Levemir), degludec (Tresiba).
Dosed once daily (some, such as Levemir, may require BID).
Bolus insulin - surges of insulin around meals or in response to glucose spikes.
Goal: cover meals and correct hyperglycemia in real time.
Examples: lispro (Humalog, Admelog, Lyumjev), aspart (Novolog, Fiasp), glulisine (Apidra), regular insulin (Humulin R — slower, less commonly used).
Practical Considerations
50/50 rule: As a starting point, total daily insulin is roughly split into 40-50% basal and 50-60% bolus.
Real life variation: Many patients creep into “overbasalization” (≥70% basal insulin, <30% bolus) if afraid of hypoglycemia or avoiding carb counting.
Rounding & devices: Syringe (nearest 0.5–1 unit), pens (nearest 1 unit), pumps (decimal dosing possible).
2. Determining an Appropriate Insulin Regimen
Basal only
Once daily long-acting insulin.
Usually for early type 2 diabetes, as patients still make some endogenous insulin.
Pros: simple, only 1 injection/day.
Cons: does not cover food or prevent post-meal hyperglycemia in type 1.
Not sufficient for type 1 diabetes (unless honeymoon period or terminal care).
Two-injection regimen (premix insulin or split mixed)
Mix of intermediate/rapid (e.g., NPH + Regular or NPH + Rapid) at breakfast and dinner.
Covers basal + meals together, but inflexible: patient has to eat consistently timed meals in consistent amounts.
Best for: patients with structured schedules, limited resources, who cannot carb count.
Less common in modern type 1 management.
Basal-bolus regimen (modern standard of care for type 1)
Long-acting once daily for basal needs.
Rapid insulin before each meal, guided by carb ratio and ISF.
Flexible, physiologic, allows adjusting doses depending on carbs/activity.
Fixed dose regimen
Provider prescribes set insulin doses with each meal (e.g., 5 units breakfast, 10 units lunch, 8 units dinner).
No flexibility: patient must eat to match insulin rather than insulin matching food.
Historically common, but less optimal for active patients.
Sliding scale
Reactive: bolus insulin only given based on glucose level (e.g., “Give 4 units if glucose is 200-250”).
Lacks proactive carb coverage, often leads to highs and lows.
❌ Outdated if used alone, but can be used in hospital or layered on top of basal-bolus for corrections.
3. Calculations
Total Daily Dose (TDD) = - 0.5 × body weight (kg) = TDD 50% → Basal, 50% → Bolus
Carb Ratio (ICR) = Rule of 500 (rapid insulin).
amount of bolus insulin to dispose 4-30 g of carb based on insulin sensitivity
lower ratio means more insulin needed to cover type 1 diabetes
500 ÷ TDD = grams of carb covered by 1 unit.
Rounding - Whole numbers unless <5, Decimal end round in direction of easier numbers
Insulin Sensitivity Factor (ISF) = Rule of 1800 (rapid insulin).
estimated point drop in mg/dL of BG for every correction taken in type 1 diabetes
1800 ÷ TDD = glucose drop per 1 unit insulin.
typically goal is somewhere between 100-120 mg/dL for us 120
Rounding
should end in a 0 or 5 if not round in direction of easier math