W9: Sensory Evaluation of Binocular Vision
Outline
Sensory evaluation is required in both NSBV conditions and in strabismus/anisometropia
NSBV conditions
Suppression
Stereoacuity
Strabismus or anisometropia
Sensory adaptation to diplopia (one object in two different spatial locations) or confusion (two different images in same spatial location; simultaneous arrival in visual cortex of non-fusible images from each fovea)
Binocular adaptation
Suppression
ARC - abnormal retinal correspondence.
Monocular consequence
Amblyopia - suppressed eye will have reduced VA.
Eccentric fixation - not using the fovea to fixate
Sensory Evaluation in Non-Strabismic Binocular Vision (NSBV) Conditions
Sensory anomalies in NSBV are significantly less severe compared to strabismus.
Stereopsis is generally normal or only mildly reduced.
Mild suppression can occur in heterophoria conditions.
The suppression scotoma is smaller than that observed in strabismus.
The presence of suppression and/or reduced stereopsis is crucial for prognosis and devising a sequential management plan.
A larger suppression scotoma correlates with a greater impact on stereoacuity.
Evaluation of Suppression
Suppression is evaluated based on its size and depth/intensity.
Clinically, intensity is the most critical factor.
Qualitative assessment of intensity is determined by how easily suppression can be broken down.
e.g., light vs dark room testing.
Deep suppression is diagnosed if diplopia cannot be elicited even in a dark room.
Clinical Tests of Suppression:
Worth 4 Dot test (main clinical one)
Bagolini filter bar
Mirror Pola test (vision therapy in younger children)
4BO test
Also assessed through general binocular vision testing:
Near Point of Convergence (NPC)
Near lateral phoria
Near Mallett unit (patient may not see both sets of polarising strips when wearing filters)
Fusional vergence testing
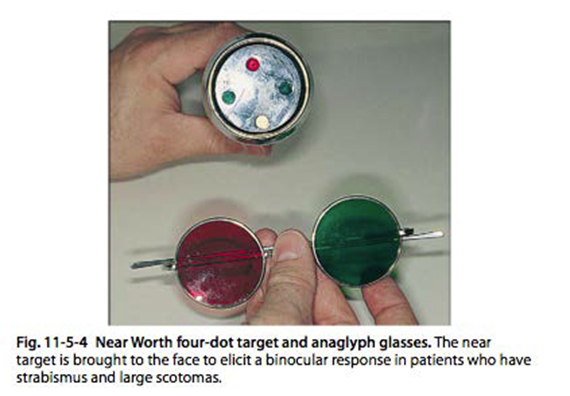
Worth 4 Dot (W4D) Test for Suppression
Distance test: Target subtends 1.25 deg at 6m
Near test: Target subtends 6 deg at 33cm
Suppression might be present only at distance.
The visual angle of the near target might be larger than the suppression scotoma, allowing fusion.
If suppression is present at 33cm, bringing the target to a very close working distance can sometimes elicit a fusion response.
Interpretation Examples:
Left suppression at distance only: Patient sees red dots (image from the right eye).
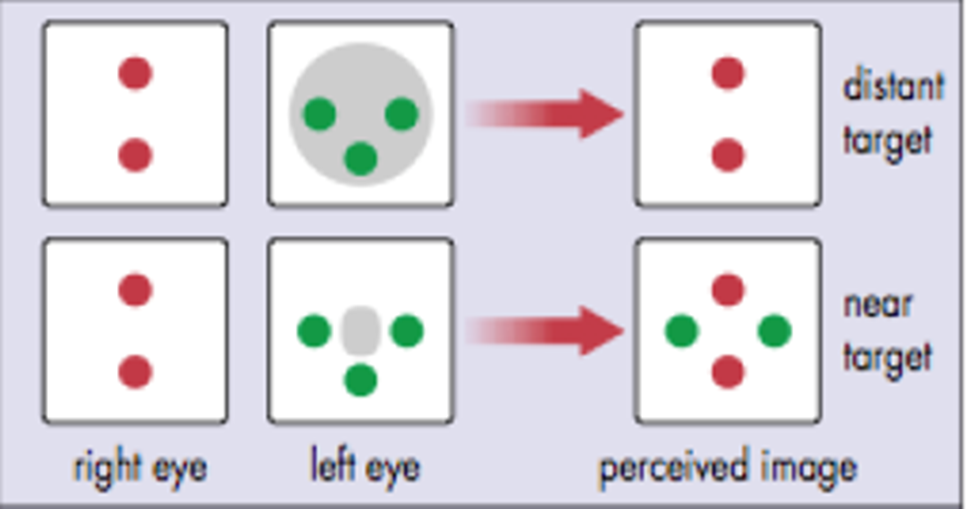
Right suppression at distance only: Patient sees green dots (image from the left eye).
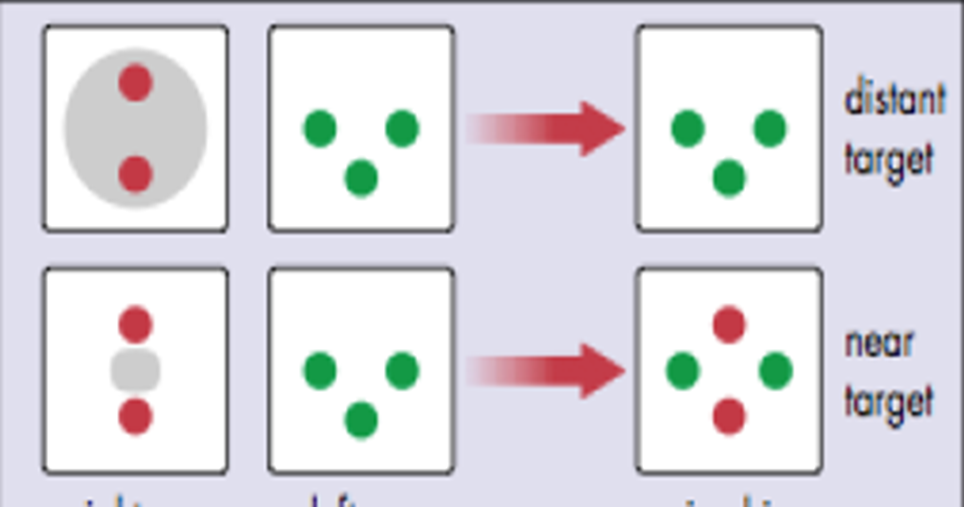
Normal fusion response or Anomalous Retinal Correspondence (ARC): Patient sees dots (the bottom dot will be the colour of dominant eye).

Diplopia: Patient sees dots (e.g., red and green spatially separated).

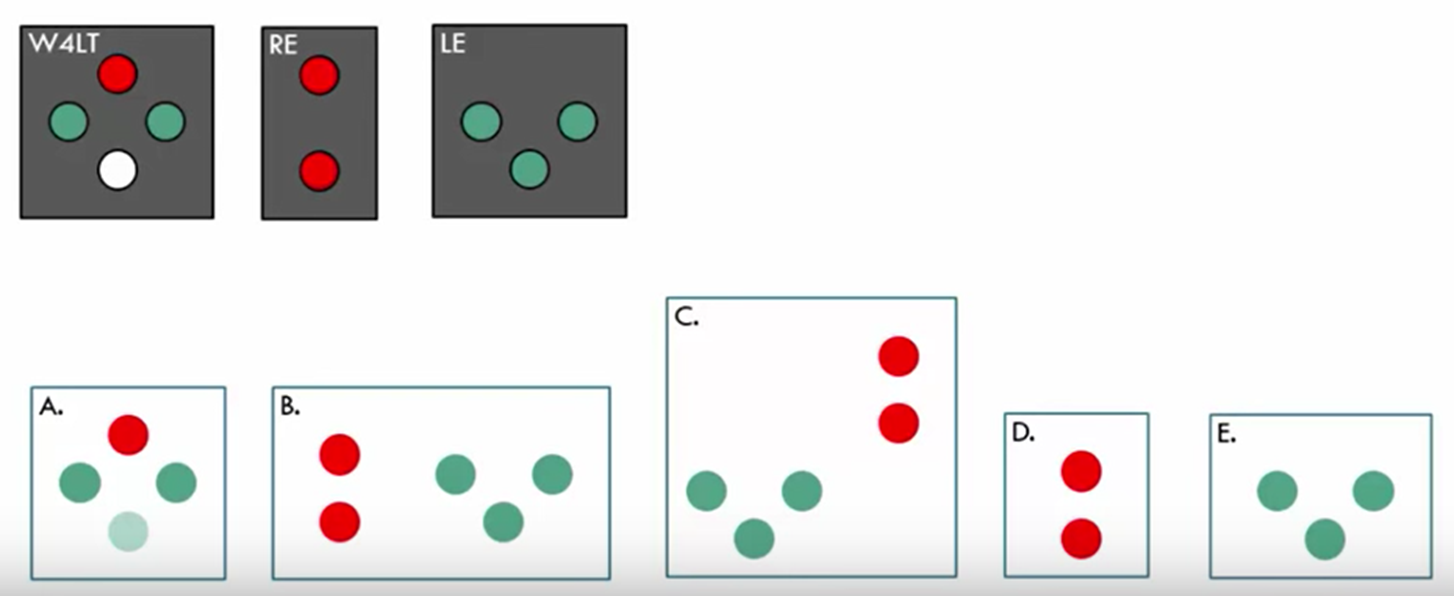
Koklanis, Latrobe School of Orthoptics (YouTube instructional video) W4D interpretations:
A: Normal fusion (if cover test shows alignment) OR ARC (if strabismus is manifest) - implies left eye dominance.
B: Horizontal diplopia (left eye image is perceived to the right, indicating crossed diplopia - exotropia)
C: Vertical and horizontal diplopia (left eye image is perceived to the left, indicating uncrossed diplopia).
D: Left suppression.
E: Right suppression.
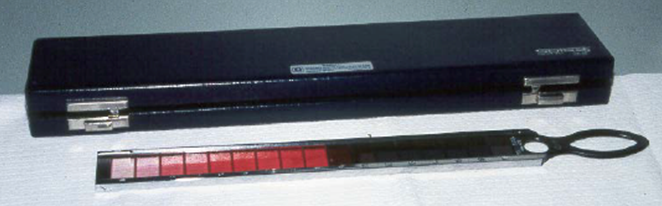
Bagolini Filter Bar for Suppression
Used to measure the depth of suppression.
The retinal luminance of the fixing eye is gradually reduced until the patient becomes aware of the image perceived by the suppressing eye.
by moving to deeper red colour.
Consists of filters, ranging from (light pink) to (dark red).
If suppression persists with filter to , it indicates deep suppression.
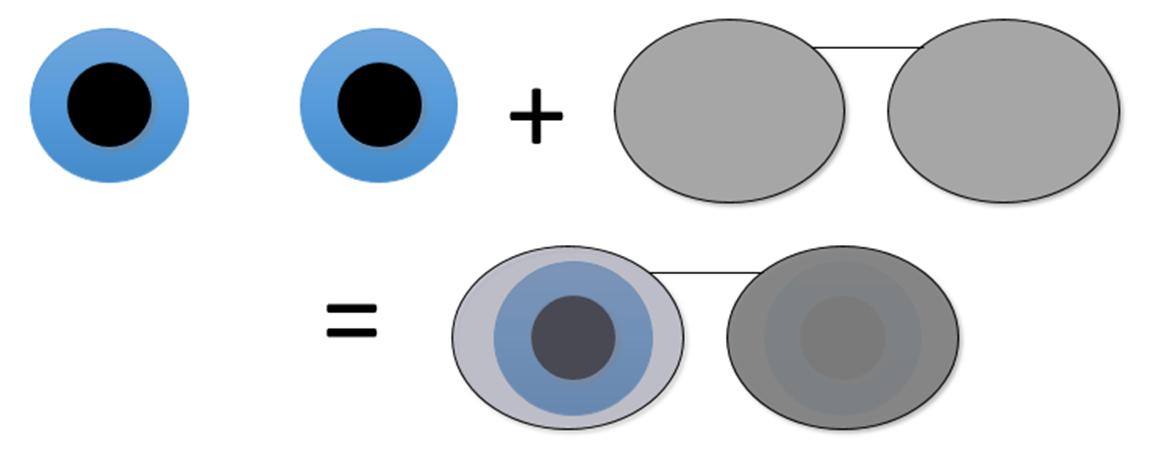
Mirror Pola Test for Suppression
A qualitative assessment for suppression.
Each eye views its own reflection in a mirror.
The darker reflection corresponds to the suppressing eye.
4BO (Base Out) Test for Suppression
A 4BO prism is held over one eye while the patient fixates on a distant spotlight target.
The examiner observes the movement of the fellow eye.
Procedure and Interpretation:
If no suppression: When the prism is placed over either eye, the fellow eye makes a small saccade outwards, followed by fusional convergence which turns the eye back in.
If suppression (prism over 'non-suppressing' eye): The fellow eye makes a small saccade outwards and then remains turned out, as the fusional convergence movement is absent due to suppression.
If suppression (prism over 'suppressing' eye): Neither eye moves because the prismatic displacement of the target is not detected by the suppressing eye.
The procedure is repeated by placing the prism over the other eye.
A positive 4BO prism test signifies that suppression is detected.
Evaluation of Stereoacuity
Perception of three-dimensional visual space resulting from binocular disparity cues.
Occurs when image components fall on closely separated non-corresponding retinal points within Panum's fusional area.
Stereopsis testing is a quick and effective method to assess sensory fusion status.
Grading stereoacuity allows for the assessment of severity
useful for monitoring progression or the effect of treatment.
seconds of arc () is the expected normal stereoacuity in normal binocular vision.
A disparity in dichoptically presented images will be detected as having depth.
Types of Stereopsis
Global Stereopsis:
Requires bifoveal fixation.
at the point of testing, the px does not have a strabismus.
Involves a larger area of retinal stimulation with no monocular contours.
Cannot be present if strabismus is manifest at the time of testing.
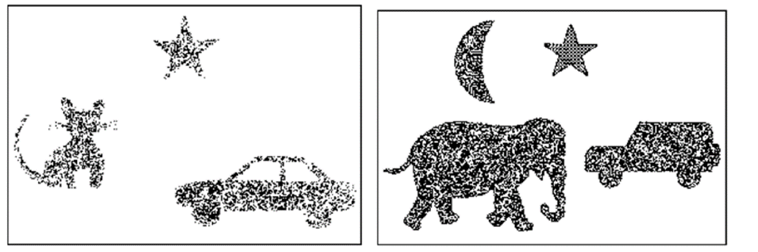
Assessed with random dot stereo (RDS) tests (e.g., Randot, TNO, Frisby, Lang).
Local Stereopsis:
Can occur without bifoveal fixation.
Involves a localized area of retinal stimulation.
Assessed with Titmus stereotest (e.g., fly, animals, Wirt circles).
Monocular contours within the test (e.g., circles in Titmus) can confound results, as the patient might not truly be seeing depth but rather using monocular cues.
used for a threshold - useful for vision therapy.
Clinical Tests of Stereoacuity
Most clinical tests utilize cross-polarization to dichoptically present patterns with disparity, creating the illusion of 3D
Specific Tests:
Randot Preschool Stereotest: Vectographic (uses polarised filters).
Titmus Stereotest: Vectographic.
TNO Stereotest: Anaglyphic (uses red and green filters).
Frisby and Lang Stereotest: Do not require filters.
useful for young children
Randot Preschool Stereotest
Designed as a matching game for children as young as years old.
Each of the test books contains sets of random dot shapes (one is blank) that can be named or matched to easily visible black-and-white shapes on the opposite page.
Stereoacuity is defined as the smallest disparity at which the child can correctly identify at least of shapes.
Procedure:
With full room illumination, place polarised filters on the patient over their best correction.
Present the test booklet at40cm. Crossed disparity is created, making forms appear to “float” or pop off the page
present the test booklet at 40cm
Book 1 is presented first to test 200 arcsec and 100 arcsec levels of disparity
if the child is able to correctly identify 3 of 3 shapes, proceed to book 2
if the child is unable to identify 2 of 3 shapes, proceed to book 3.
Book 2 is presented to test 60 arcsec and 40arcsec disparity
book 3 is presented to test 800 arcsec and 400 arcsec
Recording:
record the best stereoacuity achieved by the patient
record any added lenses or prisms used for testing.

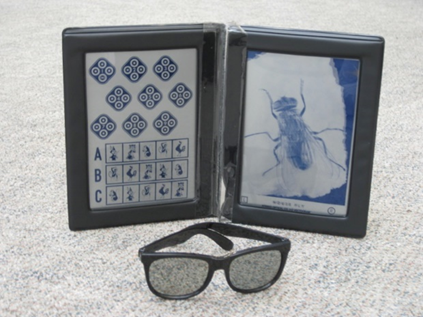
Titmus Stereo test
Purpose: Assesses stereopsis using disparity targets.
Sections: Three main sections for different types of disparity targets.
Gross Stereopsis: Presented as a housefly, with an acuity of approximately 3000\'' (seconds of arc).
Graded Stereopsis (Younger Child): Three rows of animal figures.
Graded Stereopsis (Older Patient): Nine diamonds, known as Wirt rings.
Procedure:
Place polarizing glasses on the patient over their best correction in full illumination.
Present the test booklet at .
Direct the patient's attention to the housefly. If appreciated, gross stereopsis is present.
For young patients, present animal targets and ask them to point to the animal that "pops out" or is "out of line."
Cat: 400”
Rabbit: 200”
Monkey: 100”
For older patients (or after animals for young patients), proceed to Wirt rings. This step can be used directly for adult patients.
Direct attention to diamond 1 and describe that one of the circles should appear to be "floating out."
Ask the patient to identify the floating circle by reporting its position (top, bottom, right, or left).
Continue through all nine diamonds if responses are consistently correct.
If a patient misses one but then continues with correct responses, recheck the missed diamond.
If a patient misses several consecutively, the last correct response is recorded as the stereoacuity.
Recording:
Record the presence or absence of gross stereopsis.
Record the quantitative level of stereopsis based on the best response from animals or Wirt rings.
Note any added lenses or prisms used during testing.
Lang Stereotest
Purpose: A simple test for random dot stereopsis that does not require polarized filters.
Procedure:
Position the test at approximately under full room illumination.
Ensure the test is held exactly at right angles to the visual axis.
Ask the child to point to the location of the test targets or match them with a corresponding card.
Lang II Specific: Includes a star figure with no disparity, which can be seen monocularly. This helps confirm the child understands the test instructions.
Recording:
A positive result is indicated by correct localization and naming of objects, attempting to grasp them, or shifting fixation between objects.
Record the best stereoacuity level achieved.
Frisby Stereotest
Purpose: Measures stereoacuity using random dot stereograms without the need for filters.
Design: Consists of three Plexiglas plates with patterns printed on both sides. The stereo threshold is created by the thickness of the plates and the working distance.
No Filters: Polarized filters are not necessary for this test.
Procedure:
Conduct the test with full room lighting, with the test plate aligned squarely to the patient, and against a plain white background.
Hold the thickest plate () at a convenient distance for demonstration.
Point out the "floating circle" or "hole."
Ask the patient to locate the circle by verbally reporting or pointing. Once correctly located, rotate the plate to a new position.
Ensure there is no head movement during the test.
To assess stereoacuity, begin by presenting the , , and plates sequentially at a test distance.
Present each plate at least four times, randomizing the circle's position with each presentation.
If the patient correctly identifies the circle's position in each plate at at least three out of four times, this indicates a stereoacuity of at least 55\'' (seconds of arc).
Continue testing using the plate at greater test distances to find the threshold.
Recording:
Record test distances, plate thickness, and the number of correct responses out of the total presentations given.
Example: , plate, 3 of 4 correct.
Record the resulting stereo threshold using a provided table.
Sensory Status in Strabismus and Anisometropia
Conditions Affecting Visual Development
Strabismus: Misalignment of the eyes.
Can lead to diplopia (seeing the same object in two different spatial locations).
Anisometropia/Deprivation: Significant difference in refractive error between the eyes, or an obstruction to vision (e.g., ptosis, congenital cataract).
Can lead to confusion (seeing different objects in the same spatial location).
Sensory Adaptations
Overview
Sensory adaptations may occur if strabismus and/or anisometropia are present early in life.
Binocular (when both eyes open)
Suppression = ignoring unwanted second image (avoids diplopia and confusion)
Anomalous retinal correspondence = aberrant neural wiring of binocular information
Monocular consequences (present when fellow eye covered)
Amblyopia = degraded development of visual pathways
Eccentric fixation = loss of foveal viewing preference
Binocular Adaptations (Both Eyes Open)
Suppression: The brain ignores the unwanted second image to avoid diplopia and confusion. While helpful binocularly, it can lead to amblyopia or eccentric fixation.
Developed to manage retinal image differences:
Differences in image clarity (anisometropia).
Differences in image size (aniseikonia).
Occurs in zones:
Foveal suppression avoids confusion.
Foveal suppression of the non-fixating eye occurs in strabismus.
Foveal suppression of the blurred image occurs in anisometropia.
Can be intermittent or constant.
Anomalous Retinal Correspondence (ARC): An aberrant neural wiring of binocular information. A non-foveal area of the deviating eye acquires a common visual direction with the foveal area of the fixating eye.
In the central retina, normal retinal correspondence is more likely, otherwise suppression or amblyopia tends to occur.
In the periphery, binocular function is more resistant to loss, increasing the chance of ARC.
Monocular Consequences (Present When Fellow Eye Covered)
Amblyopia: Degraded development of visual pathways, resulting in poor vision even with optimal refractive correction.
Eccentric Fixation: Loss of foveal viewing preference, where fixation of an object occurs by a point other than the fovea, which then adopts the principal visual direction.
Evaluation of Anomalous Retinal Correspondence (ARC)
Clinical Tests for ARC
Bagolini Striated Lenses
Worth 4 Dot (W4D) Test
After-image Test
Comparison of subjective and objective angles of deviation (strabismus)
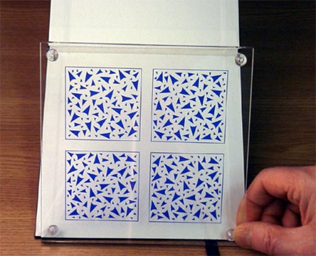
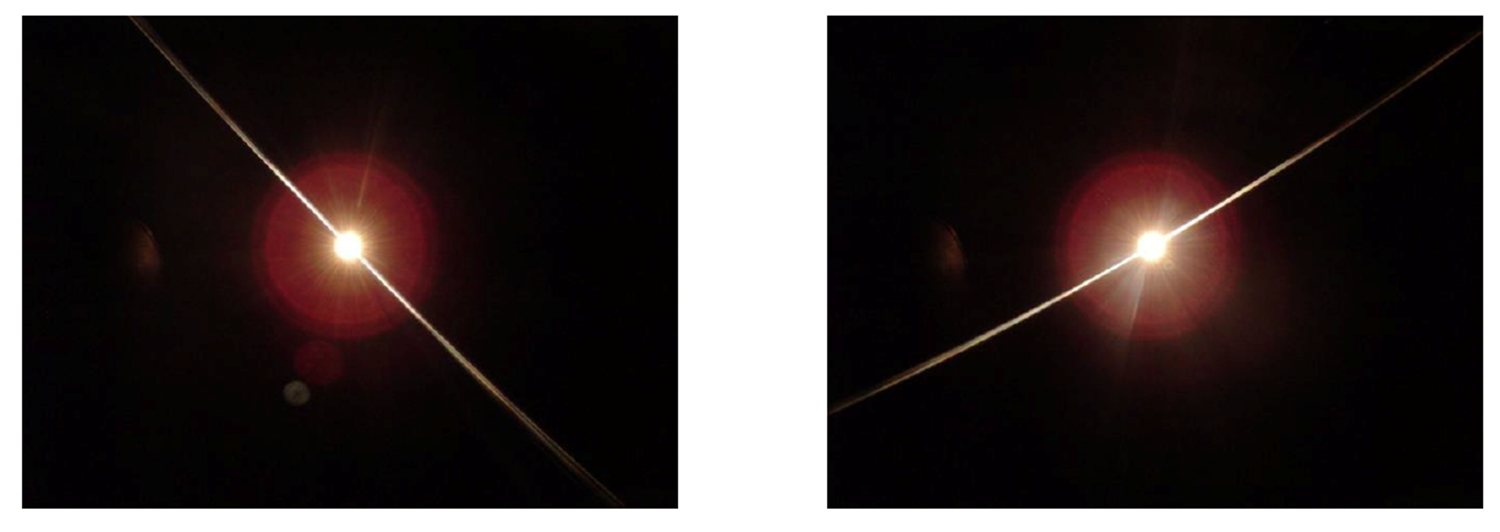
Bagolini Striated Lenses
Principle: Lenses with fine parallel striations (at and ) are placed before both eyes. When viewing a spotlight, each lens produces a line image perpendicular to its striations.
Testing Conditions: Performed under relatively natural conditions (normal room lighting) to allow fusion of surrounds.
Patient Report: Patient reports the number of line images and spotlights seen, and the form the lines make.
Interpretations:
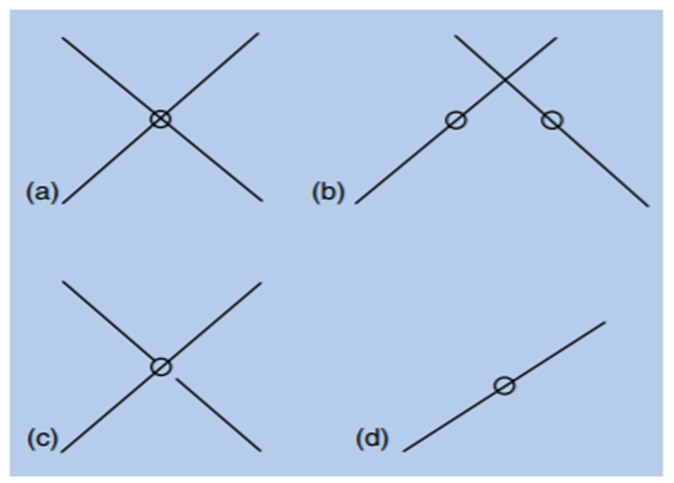
A = Normal or abnormal retinal correspondence (in presence of strabismus)
B = Strabismus with diplopia
C = Normal or abnormal retinal correspondence with a suppression scotoma
D = Suppression of fellow eye
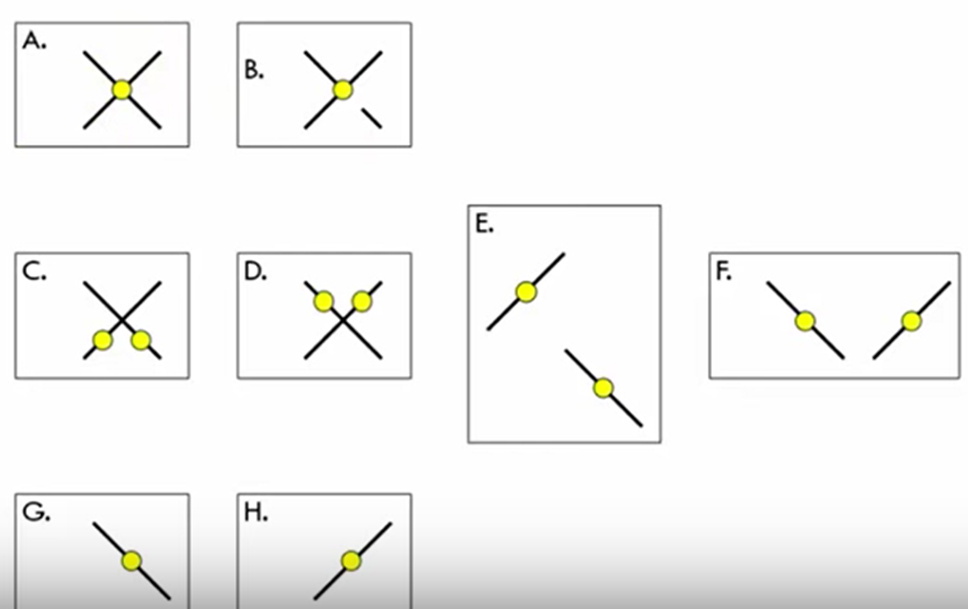
A = Normal Fusion or ARC (with manifest strabismus): Two lines crossing through a single spotlight. If a cover test shows alignment, it's normal fusion. If strabismus is present with a cover test, it's ARC.
B = Normal Fusion or ARC with Central Suppression of Left Eye: A single spotlight with one continuous line (from the right eye) and a broken line (from the left eye, indicating central suppression).
C = Horizontal Diplopia (Left eye on right = Crossed Diplopia): Two spotlights and two lines, with the line from the left eye appearing to the right (crossed).
D = Horizontal Diplopia (Left eye on left = Uncrossed Diplopia): Two spotlights and two lines, with the line from the left eye appearing to the left (uncrossed).
E = Vertical Diplopia: Two spotlights and two lines, with one line appearing above or below the other.
F = Horizontal Uncrossed Diplopia (Large Angle): Similar to D, but implies a larger separation, often with the lines visible but widely separated.
G = Right Suppression: Only the line from the left eye is seen, indicating suppression of the right eye.
H = Left Suppression: Only the line from the right eye is seen, indicating suppression of the left eye.
Worth 4 Dot (W4D) Test
Used to assess fusion, suppression, and ARC. A normal fusion response or ARC result (in the presence of strabismus) is indicated by seeing four dots.
After-image Test
Principle: Uses a bright flash of light (e.g., electronic flash gun, synoptophore) to create after-images on the fovea/foveal projection of both eyes. It demonstrates the relationship between the foveal projections.
Purpose: It is a test of retinal correspondence, comparing retinal areas that have the same visual direction during binocular single vision.
Procedure:
A horizontal line image is presented to the fixating eye first.
A vertical line image is presented to the deviating eye.
Interpretation:
Normal Retinal Correspondence (NRC): The horizontal and vertical after-images intersect centrally, forming a cross with the center at the fixation point.
Anomalous Retinal Correspondence (ARC): The horizontal and vertical after-images do not intersect centrally, or the intersection is displaced, indicating that the fovea of the deviating eye is not corresponding with the fovea of the fixating eye.

Subjective and Objective Angles of Strabismus
Objective angle: cover test
subjective angle: Maddox
rod - Anomalous retinal correspondence.
If the subjective angle is equal to the objective angle, then Normal Retinal Correspondence is present.
Formulaic Representation: \text{Objective Angle} - \text{Subjective Angle} > 0 \implies \text{ARC}
Example:
Alternating cover test measures (prism diopters) esotropia (objective angle).
Maddox rod is aligned without prism (subjective angle = ).
20\Delta - 0\Delta = 20\Delta > 0, therefore, Anomalous Retinal Correspondence is present.
Amblyopia
Definition: A monocular consequence of binocular adaptation (suppression), characterized by poor vision due to abnormal visual development.
Diagnosis Criteria:
Visual acuity (VA) deficit in one or both eyes, with optimum refractive correction in place (typically line difference between eyes).
Presence of an amblyogenic factor is essential for diagnosis:
Strabismus.
Significant refractive error (including anisometropia).
Deprivation (e.g., ptosis, congenital cataract).
Fixation preference with the non-amblyopic eye.
NO signs of other ocular pathology (e.g., retinal disease, optic nerve abnormalities).
Clinical Importance: Cycloplegic refraction is crucial to confirm any refractive contribution to amblyopia and for a thorough examination through dilated pupils.
Eccentric Fixation
monocular consequence of suppression.
Definition: A uniocular condition (present when the fellow eye is covered) in which an object is fixated by a point other than the fovea.
This non-foveal point then adopts the principal visual direction.
Characteristics:
Fixation is parafoveal (rather than central).
Can be steady (one preferred fixation location) or unsteady (fixation location changes over time, e.g., wandering).
The degree of eccentric fixation is defined by its distance from the fovea in degrees.
Clinical Significance:
Strong association with strabismus, amblyopia, and ARC.
Reduces the prognosis for successful amblyopia treatment.
Can complicate the accurate measurement of the objective angle of strabismus, which affects ARC determination.
Markedly reduces best-corrected visual acuity (BCVA) due to the resolution limitations of para-foveal areas compared to the fovea.
Clinical Assessment: Performed with visuoscopy.
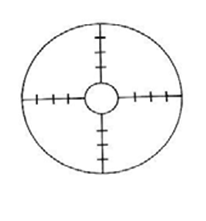
Visuoscopy
Instrument: A visuoscope is essentially an ophthalmoscope with a graticule (a four-pointed star with a clear central area) that serves as a fixation target. Some visuoscopes include a green filter.
Procedure:
Occlude the patient's other eye.
Ask the patient to look at the central target (the graticule's center).
Dim the room lights.
Observe the position of the foveal reflex in relation to the graticule.
Determine if the target is steadily on the fovea:
If the foveal reflex is steady and centered within the graticule, it indicates central, foveal fixation (not eccentric).
If not, determine the magnitude (in degrees) and direction (e.g., superior nasal, inferior temporal) of the eccentric fixation.
Note: Each target notch typically corresponds to (prism diopter) or approximately (degrees), though this can vary by ophthalmoscope brand.
Assess the stability of the eccentric location over time (is it steadily maintained, unsteady, or wandering?).
Recording: Assess and record in terms of:
Position: Central, parafoveal, macular, peripheral.
State of Fixation: Steady, unsteady, wandering, or eccentric.
Example Visuoscopy Images:
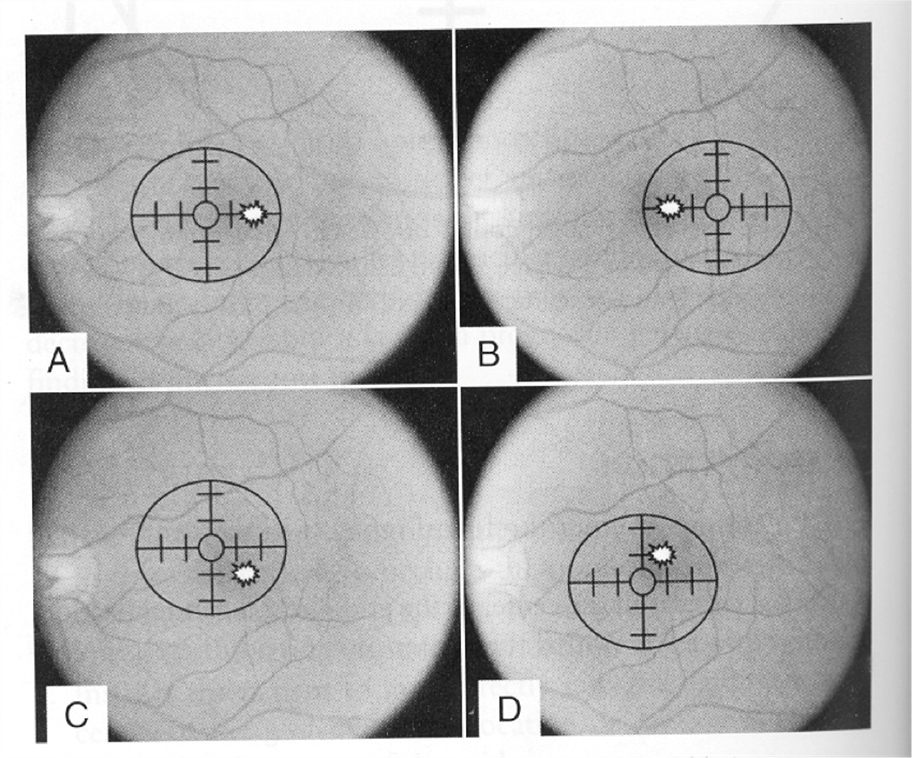
A = Nasal EF: Fovea is temporal to the fixation target.
B = Temporal EF: Fovea is nasal to the fixation target.
C = Superior Nasal EF: Fovea is inferior temporal to the fixation target.
D = Inferior Nasal EF: Fovea is superior temporal to the fixation target.
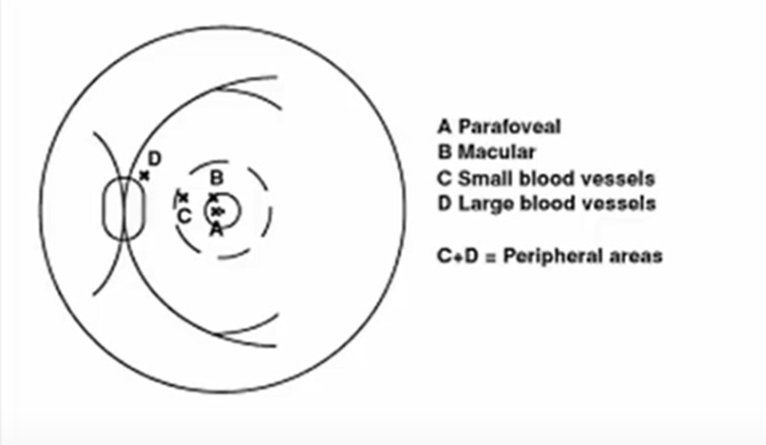
A (Image Labeling) = Parafoveal: Fixation close to the fovea but not central.
B (Image Labeling) = Macular: Fixation within the macula but not necessarily foveal.
C+D = Peripheral Areas: Fixation outside the macular region, potentially near small or large blood vessels.
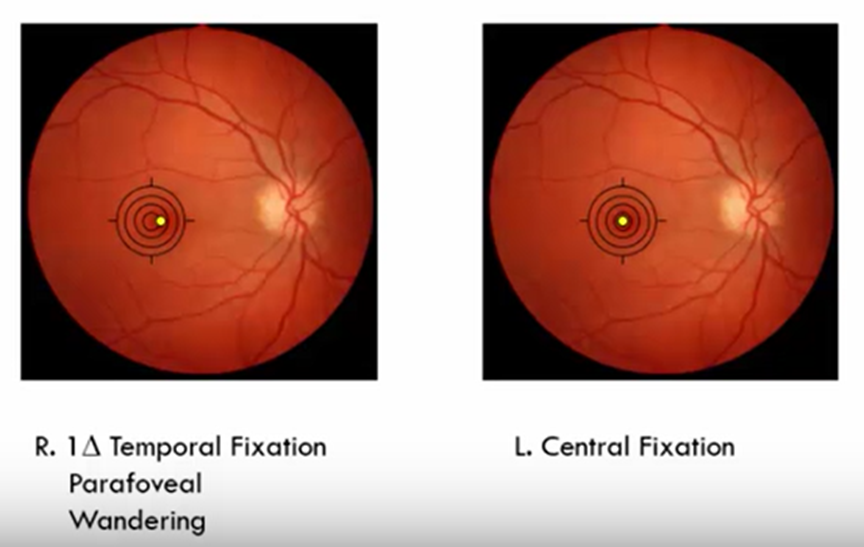
Example Record: "R. Temporal Fixation, Parafoveal, Wandering. L. Central Fixation."
Graphical Analysis - Vergence and Accommodation Criteria
ANSWERS IN POWERPOINT FOR PRACTICE!!!!!!!!
Case 1 Example
Patient: 10yo, IPD
Findings:
Distance (D): exophoria
Near (N): exophoria
D: PFV 4/10/8; NFV -/10/8
N: PFV 12/20/14; NFV 15/20/16
NRA:
PRA:
NPA:
NPC:
Question: Are Percival's and Sheard's criteria met?
Case 2 Example
Patient: 15yo, IPD
Findings:
Distance (D): Ortho
Near (N): esophoria
D: PFV 4/20/16; NFV -/4/2
N: PFV 8/25/20; NFV 4/6/4
NRA:
PRA:
NPA:
NPC:
Question: Are Percival's and Sheard's criteria met?
Fixation Disparity Curve (FDC) Analysis
Case 1 Example
Patient: 20yo, IPD
Fixation Disparity Data:
Baseline: exo (mins of arc)
: exo
: exo
: exo
: exo
: exo
: exo
: exo
: Diplopia
: Relative exo
: -
Curve Type: Type III Curve.
Characteristics of Type III:
Adapts well to Base-In (BI) prism.
More commonly observed in exophores.
Management often prioritizes prism as a first option, followed by vision therapy (VT).
Case 2 Example
Patient: 30yo, IPD
Fixation Disparity Data:
Baseline: eso (mins of arc)
: eso
: eso
: eso
: eso
: eso
: eso
: Diplopia
: Diplopia
: -
: -
Curve Type: Type II Curve.
Characteristics of Type II:
Adapts more to Base-Out (BO) prism.
More commonly observed in esophores.
Responds better to prism or plus lens addition.
Integrative Analysis - Exophoria Case Study
Case 1: University Student (22 years old)
Symptoms: Headaches when doing near work (after >2 hours), diplopia at the end of the day when tired.
Current Spectacles: Low hyperopic/astigmatic correction (SVN - single vision near).
Clinical Findings:
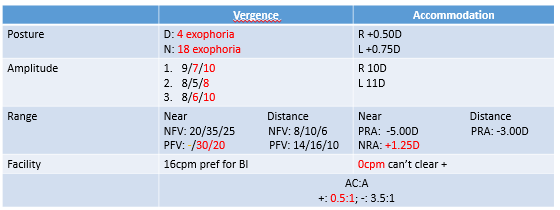
Analysis for Exophoria Patient (Focus on PFV group data):
PFV (Smooth/Step): Reduced (consistent with exophoria).
PFV (Vergence Facility): Reduced when adapting to BO prism.
NRA (Negative Relative Accommodation): Reduced. Can’t relax there accommodation → over accommodating.
can’t clear plus on facility.
BAF (Binocular Accommodation Facility): Reduced when clearing plus lenses.
NPC (Near Point of Convergence): reduced
MEM/FCC (Monocular Estimation Method Retinoscopy/Fused Cross Cylinder): Lead of accommodation observed.
not fulfilling the PFV → treatment.
Integrative Analysis - Esophoria Case Study
Case 2: School Student (11 years old)
Symptoms: "Feels cross eyed."
Current Spectacles: Low hyperopic/astigmatic correction with near add (PALS - progressive add lenses).
Clinical Findings:
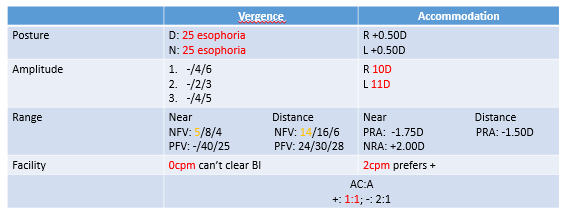
Analysis for Esophoria Patient (Focus on NFV group data):
NFV (Smooth/Step): Reduced (consistent with esophoria).
NFV (Vergence Facility): Reduced when adapting to BI (Base-In) prism.
PRA (Positive Relative Accommodation): Reduced.
BAF (Binocular Accommodation Facility): Reduced when clearing minus lenses.
MEM/FCC (Monocular Estimation Method Retinoscopy/Fused Cross Cylinder): Lag of accommodation observed.