l8 sleep
part 1: biorhythms
- biorhythms
- a variation in a biological process that repeats or cycles over a period of time (24 hours)
- circadian refers to a day circuit/cycle
- e.g. sleep, prolactin, growth hormone, cortisol, core body temp, urine volume, melatonin
- some are influenced by sleep and aren’t
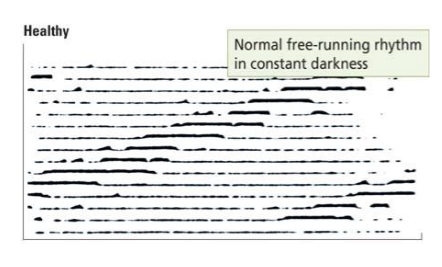
- can be internal and persist even in absence of cues
- these are called endogenous/free running rhythms
- study found leaf movement observed without much light, other examples include activity cycles in animals
- zeitgebers (time givers)
- cues that modify rhythms
- we say that a biorhythm has been entrained to that zeitgeber
- getting the cue at an innapropriate time can disrupt rhythms
- e.g. our sleep-wake cycle is entrained to light cues
- measuring biorhythms in the lab
- wheel-running behaviour shows periodic variation in rodents throughout the day, and in nocturnal rodents it is greatest at night
- biorhythms in the hamster
 * and house sparrow
* and house sparrow
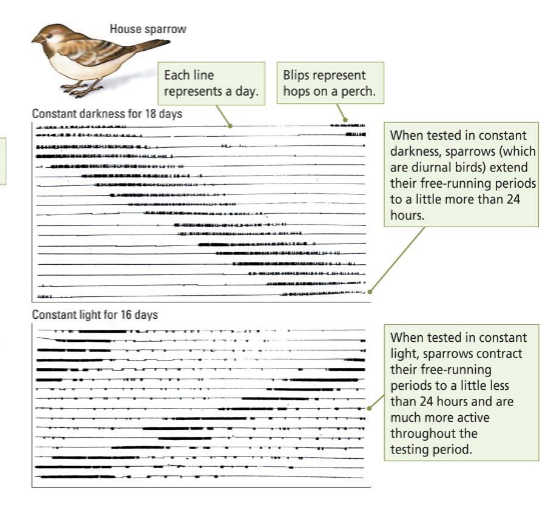 * observed in constant light and darkness
* observed in constant light and darkness
- in humans in the absence of external cues, the sleep wake cycle shifts from 24 hours to 25-27 hours
- light pollution, jet lag, graveyard shift work can disrupt light-regulated biorhythms
- biorhythms vary in length:
- circadian
- ~24 hours to repeat, e.g. sleep-wake cycles
- infradian
- 1 day < infradian biorhythm < 1 year
- e.g. menstrual cycle, also called circalunar becaue it follows lunar cycle (~28 days)
- ultradian
- eating behaviour every 90-120 minutes
- neural basis
- retinal ganglion cells (RGCs) in the eye
- entrainment begins here
- 1-3% of them express melanopsin (light-sensitive pigment)
- sensitive to certain wavelengths of blue light, and doesn’t show much adaptation
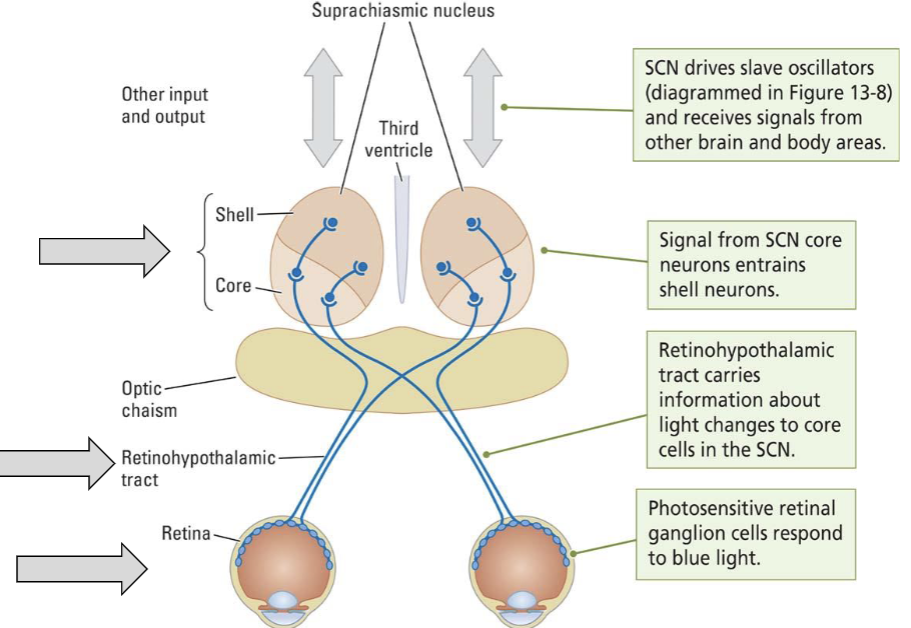
- SCN = suprachiasmatic nucleus
- located in anterior hypothalamus
- important to biological rhythms, light information affects every other rhythm in the body
- named for its proximity to the optic chiasm ( where the optic pathway decussates)
- how do we know it is involved?
- lesion abolishes many circadian rhythms
- a SCN lesioned animal can recover if it receives SCN neuron transplant from a healthy animals
- but the ‘restored rhythm’ in the lesioned animal matches the rhythm of the implanted SCN neurons!
- SCN neurons have rhythmic activity that is linked to animal’s cycle (more active during the day in diurnal animals
- SCN neurons maintain rhythm even when deprived of input or removed from brain entirely
- how do they have independent rhythms?
- CRY1 gene associated with delayed sleep phase disorder and ADHD accompanied by insomnia
- pineal gland
- key production site of melatonin
- light inhibits melatonin production
- paraventricular nucles (PVN)
- key to initiation of cortisol (CORT)
- cortisol levels rise early in the morning, during stress both when you’re unlikely to fall asleep (”cortisol awakening response”)
- \
- phase shifts
- earlier exposure to daylight
- phase advance, tired earlier
- daylight later
- phase delay, tired later
- excercising early
- phase advance, tired earlier
- excercising later
- phase delay, sleep later
- it’s not just the cue, it is the point in the cycle you recieve the cue
- earlier exposure to daylight
- reticular activating system (RAS)
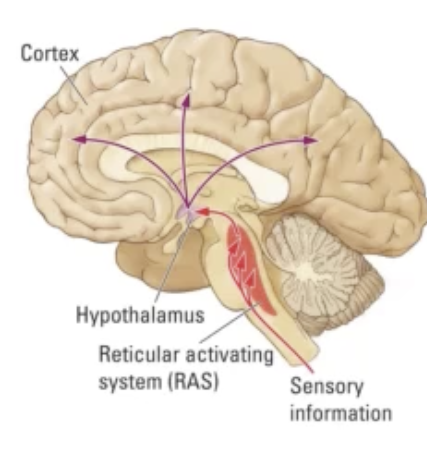
* sensitive to sensory input
* connected to the basal forebrain, providing cholinergic stimulation to the rest of the brain
* stimulation of the **reticular formation** promotes arousal
* coma can onjur with even minor injury
* evidence for its involvement in sleep:
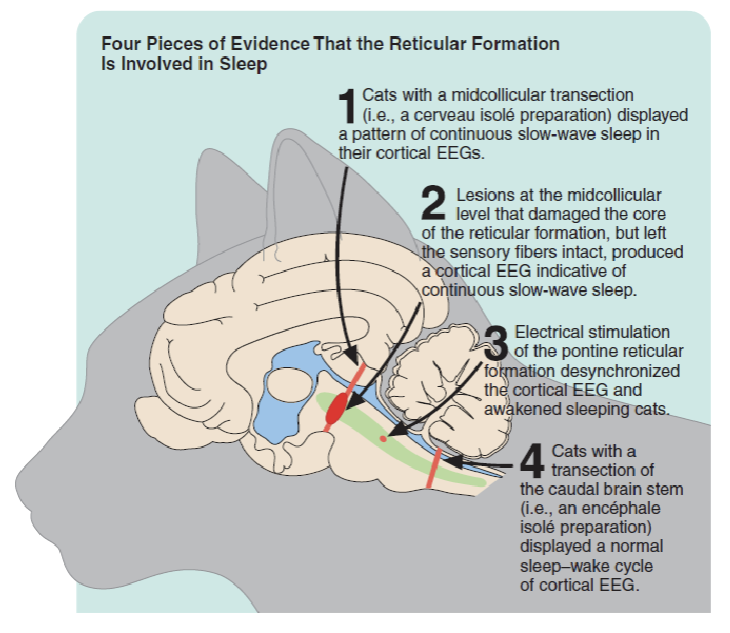 * electrical stimulation of the reticular formation wakes a sleeping cat
* lesion of it, animal is fine, lesion through it, it is in a coma
* electrical stimulation of the reticular formation wakes a sleeping cat
* lesion of it, animal is fine, lesion through it, it is in a coma
# Part 2: Sleep
- why do we need sleep?
1. maintenance of the brain (clearance of waste), restoration of injured/damaged tissue 2. ontogenetic development of the brain * the genetic changes of the brain (refer to neurogenesis) mostly occur here 3. maintenance of learning + memory process 4. energetically favourable * argues that sleep is there because there’s nothing we can do at night (dark out can’t see) 5. dreaming
- mean sleap for adults is ~7-8h
- reccomendations and social perceptions are that thisis the ‘normal’ level, but no magic number as factors such as excercise, stress + genetics all matter
- preferrably continuous because certain cycles get longer throughout the night, waking up disrupts and restarts them
- DEC2 gene, ADRB1 gene mutations are associated with less sleep in humans and animals
- more efficient sleep, less sleep still restful
- putting these genes into mice showed that they need less sleep
- chronotype
- variations in sleep-wake cycle
- morning chronotype, evening chronotype
- affected by many factors; genetics, age, gender
- shifts evident in adolescence, may be exacerbated by increasing use of electronic devices
- chronotype early when young, shifts later during adolescence, shifts back early when older
- sleeping patterns of adolescents have led to reccomendations about school start times (no eaerlier than 8:30 am)
- morningness associated with better academic performance, even though eveningness is associated with greater cognitive ability
- eveningness assoicated with poorer mental health
- chronotype related to personality
- morningness: agreeable and conscientousness
- eveningness: neuroticism in certain cases (females, adolescents), sensation seeking
- sleep has been divided into 4 distinct stages, exemplified by distinct patterns of EEG activity (great temporal resolution, measures electrical activity in specific brain regions), each one potentially serving a dif function
- 1 stage of rapid eye movement (REM)
- several stages of non REM sleep (NREM 1-3)
- sleep stages
![]() * stage NREM1 - light sleep
* alpha 7-13hz + theta waves 4-7 hz
* slightly lower frequency activity
* stage NREM2
* theta waves 4-7 hz
* sleep spindles
* k - complexes
* stage NREM 3/4 - deep or slow wave sleep
* delta waves 1-4 hz, some spindles
* contributes to feeling of ‘rest’, people who need less sleep show increased time in NREM 3 sleep
* REM - dream stage
* fast random high frequency activity, similar to eyes open wakefulness
* frequency ranges
* beta > 13 hz
* alpha 7-13 hz
* theta 4-7 hz
* delta 1-4 hz
* stage NREM1 - light sleep
* alpha 7-13hz + theta waves 4-7 hz
* slightly lower frequency activity
* stage NREM2
* theta waves 4-7 hz
* sleep spindles
* k - complexes
* stage NREM 3/4 - deep or slow wave sleep
* delta waves 1-4 hz, some spindles
* contributes to feeling of ‘rest’, people who need less sleep show increased time in NREM 3 sleep
* REM - dream stage
* fast random high frequency activity, similar to eyes open wakefulness
* frequency ranges
* beta > 13 hz
* alpha 7-13 hz
* theta 4-7 hz
* delta 1-4 hz
![]()
- sleep in the elderly
- greater sleep latency
- more arousal periods (likely awakenings)
- less REM, NREM3 (in terms of relative percentage)
- less overall sleep
- during REM
- there is atonia, lack of muscle tone
![]()
- is REM necessary?
- with REM deprivation there is REM rebound
- enter REM stage sooner, spend longer in REM stage
- lack of REM associated with reduced hippocampal neurogenesis, immune dysfunction and mood disruption
- but suppression of REM occurs w antidepressant drugs which improve mood
- REM might be a preparatory stage for wakefulness
- replacing REM states with wakeful states prevents rebounds
- with REM deprivation there is REM rebound
- memory consolidation
- process by which memory is converted into a long-term form
- part of the process may involve reaction of the memory trace (L6 replay)
- replay might occur in waking states as well as REM and NREM states
- most studies focus on replay in the hippocampus but changes in cortex might also be key
- replay in the hippampus (NREM)
- after spatial learning, (reflective of declarative memory), cells involved in the task become ‘linked’ (show correalted activity during NREM sleep
- replay in the cortex (REM)
- in humans, neurons involved in executing an implicit motor task may again become a)ctive during sleep (similar but not identical patterns of brain activity)
- sleep regularity is associated with cognitive performance
- in a study GPA is positively correlated (0.37) with the sleep regularity index (SRI)
- GPA also tends to be negatively correlated with dim-light melatonin onset
- melatonin starts being released earlier, so sleep earlier
- excercise helps with sleep regularity
- dreams
- narrative with ‘experiential resemblance to waking life’
- typically aversive >64%, rarelly happy <18% or sexual <10%
- increase in complexity with age neurocognitive theory
- REM dreams ~80% tend to be emotional, illogical, and have sudden plot shifts
- NREM dreams (~20%) are more thought-like, repetitive, centered around daily tasks
- dream theories
- dream protection theory
- Freud
- sexual + aggressive instincts are transformed into symbols, which represent wish fulfillment
- interpretation required to understand our desires
- evolutionary theory
- dreams about threats to reproductive success, to plan solutions
- activation-synthesis theory
- dreams are an attempt by the brain to interpret random activity
- dreams are not particularly important
- dream protection theory
- measuring sleep in the lab
- 2 main approaches, alone or in combination
- subjective analysis
- relies upon patient self-report
- questionnaires on sleep quality are administered to the patient and the patient responds
- e.g. Athens Insomnia Scale, Pittsburgh Sleep Quality Index, Insomnia Severity Index
- sleep diaries are used to record the patient’s sleep behaviours
- benefits
- cheap, quick, accessible (only need questionnaires and trained professionals)
- informative of patient attitudes and beliefs, may help in identifying other problems
- cons
- doesn’t address physiological function
- relies upon honest and accurate patient reports
- objective analysis
- polysomnography studies
- incorporates many techniques (EEG, EMG, EOG, ECG, breathing monitors, other devices)
- 2 main approaches, alone or in combination
# Part 3: Sleep Problems
- sleep deprivation
- has effects on cognitive function, brain structure, health
- most impacts temporary/reversible
- some effects of deprivation could last a long time (esp if it occurs during adoelscence)
- effects of deprivation on relatively greater on PFC structure and function
- sleeping and the student
- 50-60% of students report poor sleep, ~10% meet criteria for sleep problem
- poor sleep linked to less study time, lower GPA
- moderated by many factors; intrapersonal adjustment, friendship quality, academic stresses **(40%)
- insomnia
- difficult falling/staying asleep
- can be acute or chronic (>3-6 mo) may occur in recurring bouts
- primary insomnia is rare (10%)
- secondary/comorbid insomnia more common (~90%)
- heart disease, cancer, high blood pressure, diabetes etc.
- commonly comorbid with neuropsychiatric disorders (depression and axiety, ~33% insomnia cases linked)
- cataplexy
- loss of motor control (atonia) without loss of consciousness
- why?
- orexin-expressing neurons in the lateral hypothalamus may be involved in the atonia circuit
- they may inhibit other inhibitory neurons, limiting atonia to appropriate situations
- loss of orexin neurons (in narcolepsy) disinhibits them, which in turn more strongly inhibits the motor neurons (therefore atonia)
- triggered by arousing stimuli (laughing, crying, terror etc
- common in narcolepsy (70% cases)
- characterized by extreme daytime sleepiness with frequent episoes of dozing
- rapid descent into REM sleep is common
- loss of motor control (atonia) without loss of consciousness
- REM behavioural disorder
- loss of atonia during REM, tendency to act out dreams
- loss of inhibition to spinal motor neurons (poorly understood)
- somnambulism (sleepwalking)
- person leaves the bed and moves around while still sleep
- more common in childhood (12 yo) but only ~4% of adults express it
- been reports of complex, aggressive, illegal behaviours while sleepwalking
- thought to occur during NREM, not REM