1. Lesions of the Visual pathway - Optic chiasm & aneurysms
Visual Pathway Overview
Causes of Visual Pathology:
Blurred vision or visual field loss can result from several areas in the visual pathway being affected:
Anterior eye, outer retina, choroid (T1)
Optic nerve, inner retina (T2)
Optic chiasm (T3)
Retrochiasmal pathway (T4)
Optic tracts
Optic radiations
Visual cortex
Optic Nerve Pathologies
Conditions Affecting the Optic Nerve:
typically respect the horizontal midline
Includes:
Glaucoma
Optic neuritis
Anterior ischemic optic neuropathy (AION)
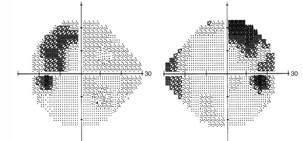
Optic Chiasmal Disease Effects:
Leading to bitemporal field defects (heteronymous). Respects horizontal midline
Example: Unilateral temporal visual field (VF) defects suggest prechiasmal optic nerve disease.
Most Common Cause: Pituitary tumour.
Retrochiasmal Disease:
Results in homonymous field defects.
More posterior lesions produce increasingly congruous defects.
Most Common Causes: Stroke, brain tumour.
homonymous = same side
heteronymous = opposite side.
congruent = VF defect similar between two eyes
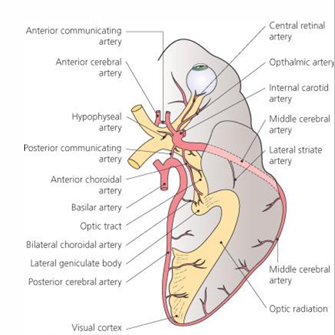
Organization of the Optic Chiasm
located posterior to orbit in the middle cranial fossa
is the place where the right and left optic nerves meet
Axonal Distribution at the Chiasm:
Delivery of axons in the optic nerve as it meets the chiasm:
Fibres:
Macula fibers are centralized.
Superior temporal (ST) retina fibers are located temporally.
Inferior temporal (IT) retina fibers are located inferiorly, etc.
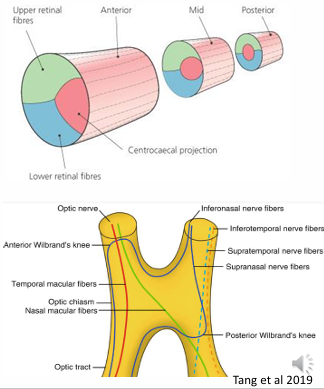
Chiasm Structure:
Superior-inferior organization remains the same.
Nasal and temporal fibers separate:
Nasal fibers completely cross to the contralateral side.
As nasal fibers cross, axons from the inferior nasal quadrant loop anteriorly to the contralateral optic nerve, then turn posteriorly to join uncrossed temporal fibers.
This structure is referred to as the Anterior knee of Willebrand.
Temporal fibers remain ipsilateral.
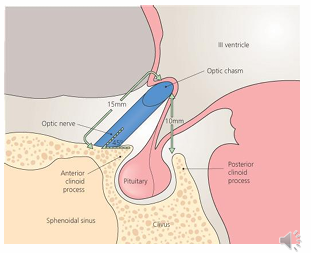
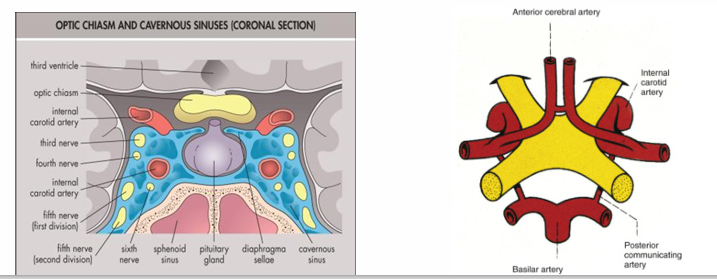
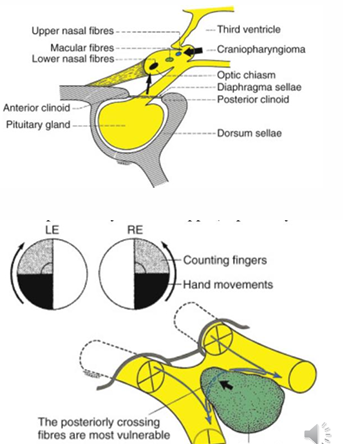
Surrounding Structures
Position of the Chiasm:
Located approximately 10 mm above the pituitary gland, which is located in the sella turcica of the sphenoid bone.
Functions and Diseases of the Pituitary Gland
Hormonal Secretions of the Pituitary Gland:
Growth hormone (GH)
Prolactin - lactating hormone
Follicle stimulating hormone (FSH)
Adrenocorticotrophic hormone (ACTH)
Thyroid stimulating hormone (TSH)
Lutenizing hormone (LH)
Beta-lipotropin
Patients with diseases of the pituitary gland may face systemic issues linked to underproduction or overproduction of pituitary hormones
Chiasm Variants and Their Effects
Central Chiasm:
Present in about 80% of normal individuals.
Found over the posterior two-thirds of the sella turcica.
Expanding tumors typically affect this region first, leading to superior bitemporal hemianopia.
Prefixed Chiasm:
Present in around 10% of normal individuals.
Positioned more anteriorly, close to the anterior edge of the sella turcica.
Expanding pituitary lesions can impact the optic tract first, leading to incongruous homonymous visual field loss.
Postfixed Chiasm:
The remaining 10% of normal individuals have this variant.
Located posteriorly over the dorsum sellae.
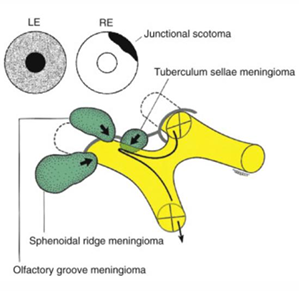
Pituitary lesions in this area are more likely to damage the optic nerve first, causing junctional scotoma.
optic nerve on one side is affected → central depression on the side of the lesion
+ supertemporal visual field defect on the contralateral side
inferonasal fibres in the anterior knee of Willibrand is affected.
general depression on one side + supertemporal VF defect on other side
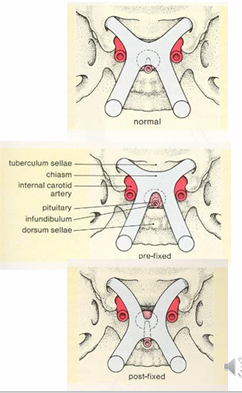
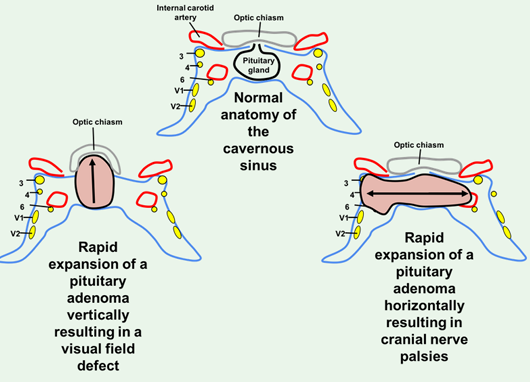
Lateral Surrounding Structures
Chiasm Adjacent Structures:
Flanked laterally by the carotid arteries and inferolaterally by the cavernous sinuses.
Tumours in the pituitary area can invade the cavernous sinus, potentially affecting cranial nerves III, IV, VI, leading to diplopia.
Aneurysms in this area may compress the optic nerve or chiasm
Optic Chiasmal Disease
Most commonly caused by tumours compressing the chiasm in the pituitary gland region.
Aneurysms can also result in chiasmal compression.
Signs and Symptoms:
Typically causes partial or complete bitemporal field loss, respecting the vertical midline.
The type of visual field loss is dependent on the location and direction of lesion enlargement, considering the anatomical relationship between the pituitary gland and the chiasm.
Potential Complications:
Mixed field defects if adjacent optic nerve or tracts are involved.
Visual acuity loss may occur if macula fibres are affected.
media opacity - VA will improve with pin hole
optic chiasm or VP defect - VA will not improve with pin hole
Px may not experience any symptoms, pupils may be normal
slow / gradual progression of visual acuity or field loss over time.
Sudden visual loss can occur due to acute expansion of compressive lesions.
pituitary apoplexy
Pituitary apoplexy:
Life-threatening event characterized by a sudden haemorrhagic infarction and expansion of a pre-existing pituitary adenoma.
Symptoms may include severe headaches, reduced consciousness levels, and binocular or monocular vision loss, along with ptosis and ophthalmoplegia.
symptoms depend on direction of pituitary adenoma
Such cases necessitate emergency hospital admission.
Clinical Signs of Optic Chiasmal Disease
Potential Presentation of Symptoms:
Relative afferent pupillary defect (RAPD) if asymmetric.
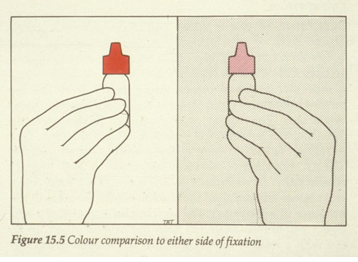
Possible colour desaturation across the vertical midline.
Diplopia due to compression of cranial nerves III, IV, or VI within the cavernous sinus.
Abnormal corneal and facial sensation from compression of cranial nerve V in the cavernous sinus.
Loss of binocular vision due to complete bitemporal hemianopia.
Normal optic discs may be observed, but optic atrophy is also a possibility in pituitary lesions.
Prognosis for visual recovery tends to be poor
although there are rare cases of disc swelling linked to raised intracranial pressure (ICP).
A vague and steadily worsening headache may also accompany these visual field defects.
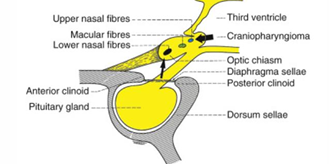
Visual Field Defects of Optic Chiasmal Disease
Field Defect Characteristics:
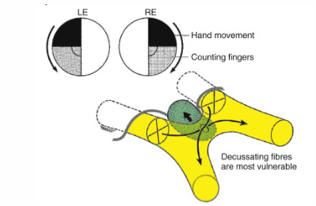
Infero-nasal fibers traverse chiasm inferiorly and anteriorly
making them vulnerable to pituitary lesions growing upward towards the chiasm.
Impacts superior temporal quadrants first.
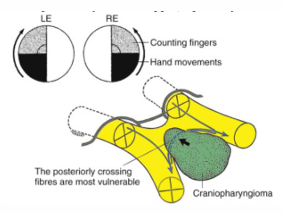
Superior nasal fibres cross higher and posteriorly
generally being involved first in lesions that expand from above the chiasm (e.g., craniopharyngioma).
Inferior temporal quadrants are often affected first in these cases
Causes of Optic chiasmal disease
Tumours:
pituitary adenoma
craniopharyngioma
meningioma
Non-neoplastic compressive:
aneurysms
intracranial cysts
Other:
MS
Trauma
infiltrative disease
inflammatory disease
Pituitary chromophobe adenoma
most common tumour affecting the chiasm, usually occurring in early adulthood to middle age.
Can secrete prolactin (prolactinomas) leading to excess levels of prolactin, causing:
Amenorrhea, infertility, and galactorrhea in women.
Hypogonadism, impotence, decreased libido, gynecomastia, and galactorrhea in men
Associated headaches due to the involvement of pain-sensitive fibers in the diaphragma sellae, typically non-specific headaches without related raised ICP symptoms.
Headache: involvement of pain sensitive fibres in diaphragma sellae
non-specific HA
generally without other features associated with raised ICP
Craniopharyngioma:
A slow-growing tumour derived from remnants of Rathke’s pouch along the pituitary stalk.
Children’s Effects:
Dwarfism, delayed sexual development, obesity.
Adults’ Effects:
Visual impairment and VF defects
Visual field loss initially usually IT, later spreads to ST fields (compresses chiasm from above and behind)
Tumour may involve ONs, chiasm or tract, so VF will depend on actual location
Meningioma:
Common in middle-aged women, often compressing the optic nerve.
Visual field signs vary based on location:
Tuberculum sellae meningioma compresses at the junction of the optic nerve and chiasm leading to a junctional scotoma.
superior temporal junctional scotoma
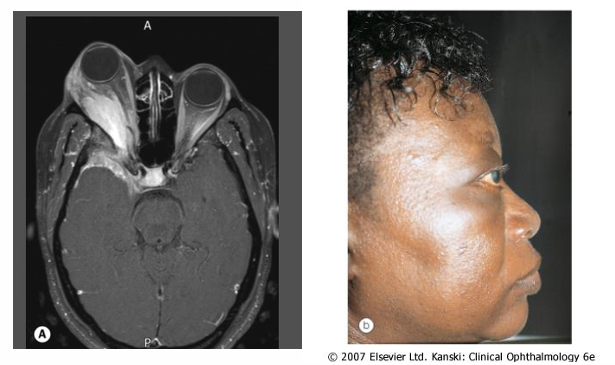
Sphenoidal ridge meningioma compresses the optic nerve early, and later affects the lateral aspect of sphenoid bone leading to fullness in the temporal fossa (hyperostosis) and proptosis.
Olfactory groove meningioma may impair the sense of smell and compress the optic nerve, leading to the Foster Kennedy syndrome with optic atrophy in one eye and papilledema in the other.
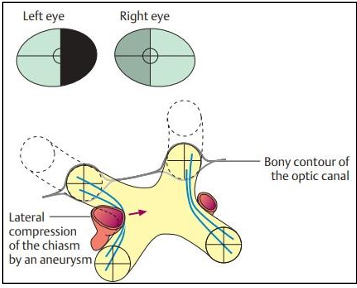
Aneurysms Affecting the Optic Chiasm
Internal Carotid Aneurysms:
Can cause chiasm compression on one side, which may lead to displacement towards the opposite internal carotid artery.
The lateral sides of the chiasm contain axons from the retina temporal to the fovea continuing uncrossed.
Resulting field defect is termed binasal hemianopia, typically worse on the side where the aneurysm resides.
Management of Visual Pathway Lesions
Pituitary region masses are sight and life threatening
Early diagnosis is associated with a good visual prognosis, and minimizes risk of systemic impairment
Patients suspected of chiasmal disease require urgent referral to neuro-ophthalmology for Neuro-imaging
Often rapid recovery of vision following surgery for pituitary adenoma, unless optic atrophy (other tumours, prognosis is less certain)
Regular follow up is required (visual fields) to check for tumour recurrence