Emergency Care and Transportation of the Sick and Injured: Airway Management
CHAPTER 11: Airway Management
Introduction
Primary component of caring for patients is ensuring that they can breathe adequately.
Disruption of the ability to breathe compromises oxygen delivery to tissues and cells.
Oxygen reaches body tissues and cells through breathing and circulation.
Anatomy of the Respiratory System
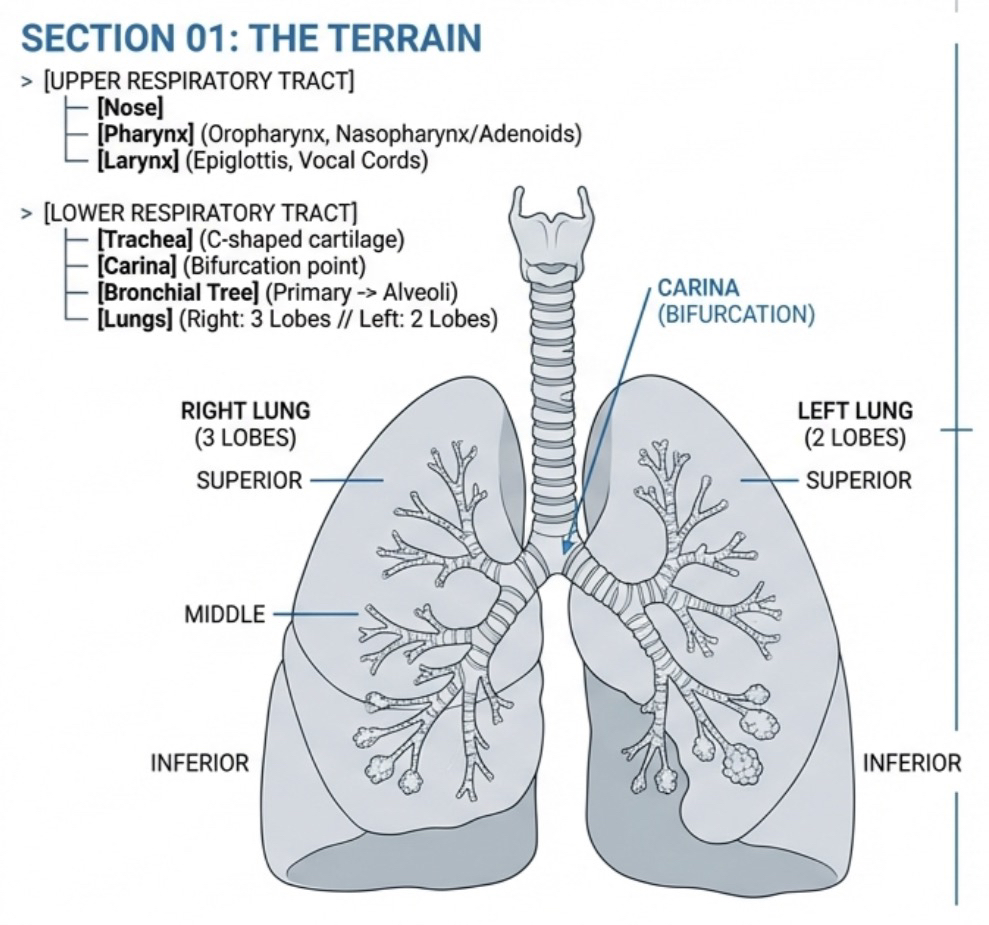
The respiratory system consists of all the structures that make up the airway and help in breathing (ventilation).
The airway is divided into the upper and lower airways.
Anatomy of the Upper Airway
Components:
Nose
Mouth
Oral cavity
Pharynx
Larynx
Main Function: The upper airway warms, filters, and humidifies air as it enters the body.
Pharynx
Muscular tube that extends from the nose and mouth to the level of the esophagus and trachea.
Parts:
Nasopharynx
Oropharynx
Laryngopharynx
Nasopharynx
Filters out dust and small particles.
Warms and humidifies air as it enters the body.
Oropharynx
Description: The posterior portion of the oral cavity.
The epiglottis is superior to the larynx.
Larynx
Complex structure formed by many independent cartilaginous structures.
Marks the endpoint of the upper airway and the beginning of the lower airway.
Key Structures:
Thyroid cartilage: forms a “V” shape anteriorly.
Cricoid cartilage: first ring of the trachea.
Glottis: area between the vocal cords.
Anatomy of the Lower Airway
Function: Deliver oxygen to the alveoli; includes:
Trachea
Bronchi
Lungs
Trachea
Conduit for air entry into the lungs.
Divides at the carina into two main stem bronchi, right and left, which are supported by cartilage to distribute oxygen to the lungs.
Bronchioles and Alveoli
Bronchioles are made of smooth muscle and connect to alveoli.
Oxygen is transported back to the heart from the alveoli for distribution.
Transport Mechanism: Oxygen is sent via the circulatory system to the rest of the body.
Thoracic Cavity
Contains important structures for ventilation, oxygenation, and respiration:
Lungs
Bronchi
Heart
Great vessels (the vena cava and aorta)
Trachea
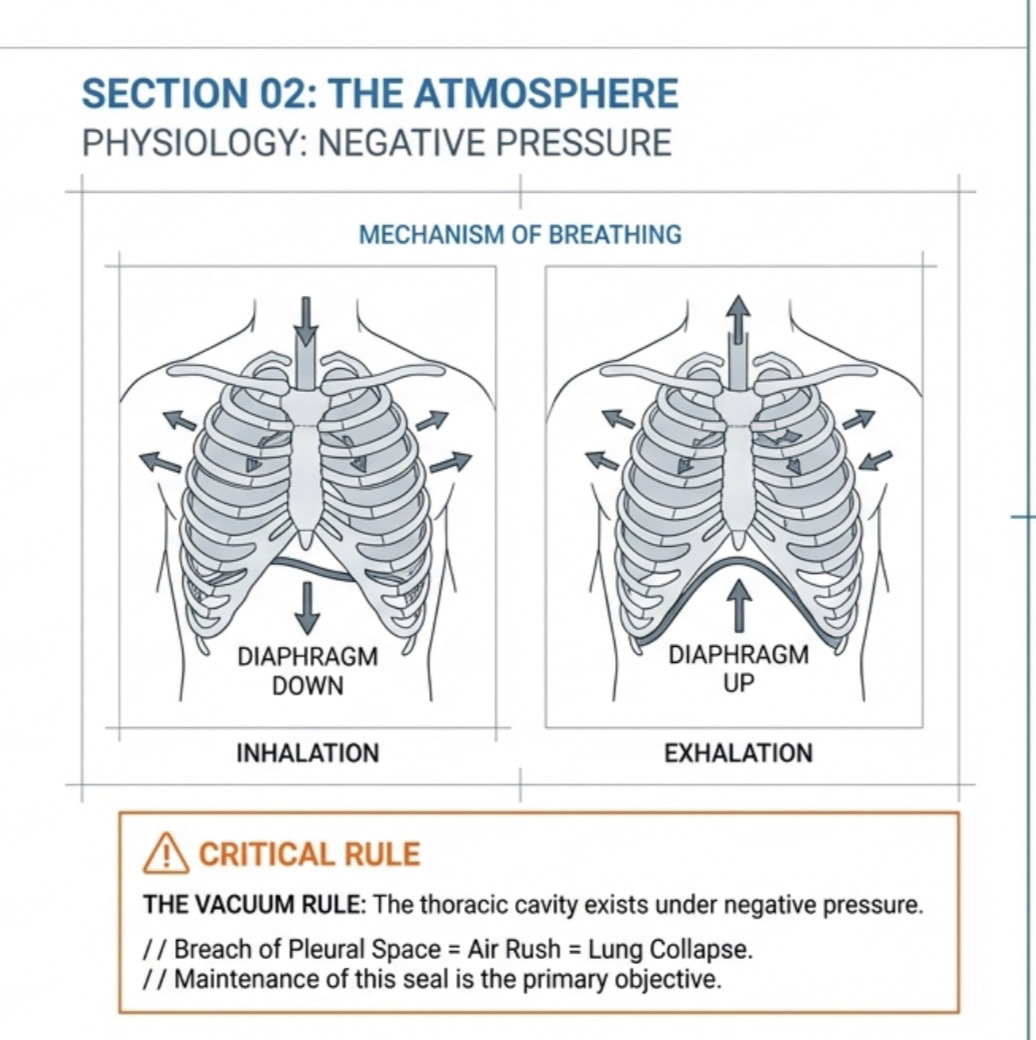
Ventilation Mechanism
Illustrated by bell jar mechanism demonstrating inhalation and chest expansion.
Physiology of Breathing
The respiratory and cardiovascular systems work in tandem to ensure oxygen and nutrients are delivered to cells and waste products are removed.
Difference between Oxygenation and Ventilation
Oxygenation:
Measured with Pulse Oximetry (normal range 94-99%).
Ventilation:
Measured with Capnography (normal range 35-45 mmHg).
Ventilation
Definition: Physical act of moving air into and out of the lungs.
Inhalation:
Active, muscular part of breathing involving contraction of the diaphragm and intercostal muscles.
Creates a negative pressure in the thorax, allowing air to enter.
Necessitates chest movement for lung expansion.
Concepts:
Partial Pressure: The amount of gas in or the air or dissolved in fluid (blood).
Oxygen and carbon dioxide diffuse until partial pressures are equal in air and blood.
Tidal Volume and Dead Space
Tidal Volume: Average of 500 mL in adults.
Dead Space: Portion of air that does not reach the alveoli.
Exhalation
Normally a passive process that does not require muscular force, relaxing diaphragm and intercostal muscles to compress air within the lungs.
Regulation of Ventilation
Involves complex receptors and feedback loops.
Failure to meet oxygen needs can result in hypoxia, often regulated by changes in pH of blood and cerebrospinal fluid.
Hypoxic Drive: Recognized in patients with end-stage COPD.
Oxygenation
Process: Loading of oxygen molecules onto hemoglobin in the bloodstream is critical for internal respiration, but does not guarantee it is occurring.
Respiration
Definition: Exchange of oxygen and carbon dioxide in alveoli and body tissues.
Types of Respiration:
External Respiration (Pulmonary Respiration):
Fresh air enters the respiratory system, facilitating gas exchange between alveoli and pulmonary capillaries.
Internal Respiration:
Exchange of gases between systemic circulatory system and cells.
Pathophysiology of Respiration
Nervous System Factors: The nervous system uses chemoreceptors to monitor levels of oxygen, carbon dioxide, hydrogen ions, and pH in cerebrospinal fluid, feeding back to respiratory centers.
Ventilation/Perfusion Mismatch
Must ensure air and blood flow to coincide.
Mismatched ventilation and perfusion results in inadequate gas exchange leading to severe hypoxemia.
Factors Affecting Pulmonary Ventilation
Intrinsic Factors:
Infections
Allergic reactions
Unresponsiveness (e.g., tongue obstruction)
Extrinsic Factors:
Trauma, including tension or simple pneumothorax, open pneumothorax, hemothorax, hemopneumothorax.
Circulatory Compromise
Trauma and airway obstructions can lead to reduced blood flow, increasing risk of hypoxia.
Causes include blood loss, anemia, or types of shock (hypovolemic, vasodilatory).
Patient Assessment
Aerosol-generating procedures (AGPs): include CPR, nebulizer treatments, endotracheal intubation, and CPAP.
Recognizing Adequate Breathing
Between 12 and 20 breaths/min, regular inhalation/exhalation patterns, bilateral clear and equal lung sounds, and adequate depth of breathing (tidal volume).
Recognizing Abnormal Breathing
Fewer than 12 or more than 20 breaths/min, irregular rhythm, diminished auscultated breath sounds, or cyanosis.
Increased effort of breathing and abnormal skin conditions may signal inadequate breathing.
Additional Signs of Inadequate Breathing
Agonal gasps may appear when the heart stops; recognizing Cheyne-Stokes respirations in patients with strokes or head injuries is critical.
Ataxic and Kussmaul Respirations
Ataxic: Irregular or unpredictable pattern often following serious head injuries.
Kussmaul: Deep, rapid respirations commonly seen in metabolic acidosis.
Airway Opening Techniques
Emergency care begins with ensuring an open airway, particularly for unconscious patients. The supine position is most effective for assessment.
The tongue is identified as the most common airway obstruction in an unconscious state.
Head Tilt–Chin Lift Maneuver
Effective method to open the airway in non-traumatized patients. Steps include:
Position beside the patient’s head.
Apply firm backward pressure on the forehead.
Lift the chin with the other hand.
Jaw-Thrust Maneuver
Recommended if cervical spine injury is suspected; uses upward force on the lower jaw.
Mouth Opening Techniques
Use the cross-finger technique when the mouth is closed to achieve airway access.
Suctioning Techniques
Essential to keep the airway clear and enable proper ventilation.
Suction equipment should be portable, with compatible tubing and suction tips.
Frequency and duration of suctioning depend on patient demographics (e.g., adult vs. children).
Care should be exercised not to activate the gag reflex or over-suction.
Airway Adjuncts
Oropharyngeal Airways:
Prevent tongue obstruction and facilitate suctioning; used in unresponsive patients without a gag reflex.
Contraindicated in conscious patients with an intact gag reflex.
Nasopharyngeal Airways:
Used in patients who are unresponsive or have impaired levels of consciousness but possess a gag reflex.
Contraindicated in patients with severe head trauma or facial abnormalities.
Maintaining the Airway
Utilize the recovery position to maintain a clear airway in conscious patients who are breathing normally.
Supplemental Oxygen
Always administer to hypoxic patients. Safety and handling of oxygen equipment is critical.
Oxygen Delivery Systems
Nonrebreathing Masks: Provide high oxygen concentration to adequately breathing patients suspected of hypoxia.
Nasal Cannulas: Deliver moderate oxygen concentration; effective for patients with mild hypoxemia.
Tracheostomy Considerations
Mask or adjunct method needed to ventilate patients with tracheostomy; improvisation may be necessary in emergency situations.
Assisted and Artificial Ventilation
Indicated when basic airway techniques are ineffective; one breath every 6 seconds is standard.
Signs of Inadequate Ventilation
Altered mental status, inadequate minute volume, excessive accessory muscle use.
Techniques for Bag-Mask Ventilation
Proper positioning, explaining the procedure, and ensuring adequate tidal volume are paramount.
Continuous Positive Airway Pressure (CPAP)
Noninvasive ventilation technique for patients in respiratory distress;
Utilizes back pressure to keep airways open and improve oxygenation.
CPAP Indications and Contraindications
Useful for alert patients exhibiting significant respiratory distress but contraindicated in certain conditions, such as respiratory arrest or significant trauma.
Airway Obstruction Management
Complete obstruction is a life-threatening scenario that requires immediate action, often seen in adults during meals and in children with small toys.
Understanding Obstruction Types
Mild: Patients can exchange air but may exhibit respiratory distress. Treatment involves allowing the patient to expel the object if able.
Severe: Patients cannot breathe, talk, or cough. Recognizable signs include cyanosis and distress.
Foreign Body Management
Uses modifications of clearance techniques, including abdominal thrusts to dislodge foreign bodies.
Dental Appliances and Facial Bleeding
Awareness of how dental appliances can interfere with ventilation and management of facial trauma is critical for maintaining airway patency.
Control any significant facial bleeding impacting the airway.
Assisting with ALS Airway Procedures
Incorporate advanced techniques and equipment setup for effective airway management for patients requiring more than basic interventions.
Review Questions
Breathing control mechanisms identified with responses contextualizing anatomy related to respiratory functionality.
E.g., control centers in the brainstem manage normal ventilation cycles via feedback from various blood gas levels.
Additional queries assessing conditions and identifying case-specific ventilation techniques.