Penis Ultrasound (Part 2) Notes
Peyronie's Disease
Most common request in general ultrasound practice.
Etiology
Fibrosis of the fibrous sheaths covering the corpora cavernosa.
Occurs due to inflammation and scarring of the tunica albuginea (inner lining that allows the penis to become hard during erections).
Fibrotic area usually located in the dorsum of the penis but can involve the septum and/or the lateral area.
Believed to originate from trauma or repeated microtrauma to the erect penis in genetically susceptible men.
Clinical Presentation
Early acute phase may present with some or all of these:
Painful erections.
Palpable plaque.
Curvature deformity of erect penis.
Late or chronic disease phase:
Occurs approximately 12-18 months post disease onset.
Pain and inflammation resolve.
Plaque and penile deformity become stable.
Extensive fibrosis and occasional plaque present.
Penile curvature deformity may worsen in some and will not resolve in the later disease stages.
Diagnosis of Peyronie's disease can be made by history and physical examination in most patients; however, in some patients, the plaque is non-palpable, making them a candidate to be diagnosed with a penile ultrasound.
Ultrasound Examination
In addition to what was discussed in lecture 1
Comment on size and location of plaque if found.
Describe the plaque found, such as:
No acoustic shadowing, hyperechoic.
Multiple calcified shadowing lesions.
Dense thick plaque with acoustic shadowing.
Important as this may be used to follow patients undergoing medical treatment in the evaluation of plaque regression.
Assessment of the cavernosal artery and its patency is important, especially if plaque appears to be extending into the corpus cavernosum.
Further doppler studies may be needed by an experienced facility to evaluate erectile dysfunction.
Sonographic Features
Echogenic plaques can be seen, usually in the dorsal aspect but can also be seen in the ventral aspect.
Calcifications can often be seen.
Non-palpable plaque can also appear as isolated septal scarring and punctate scarring.
Fibrosis and plaque may extend into the corpus cavernosum and occlude the cavernosal artery, leading to arteriogenic impotence (erectile dysfunction).
During an induced erection, plaques are seen as localized or diffuse thickening of the tunica albuginea.
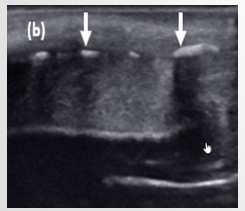
Dorsal plaque with no calcification. No acoustic shadowing present
Dense calcified dorsal plaque. Red arrow indicates acoustic shadowing
Patient presenting with curvature of the erect penis and erectile dysfunction for 1 year
Transverse view: Echogenic plaque, Acoustic shadowing.
Longitudinal view: Multiple linear calcific plaques, Acoustic shadowing
Treatment
Acute Phase:
Medical therapy (oral, topical, injectable, combination) used to:
Stabilize scar formation.
Improve deformity.
Reduce pain.
Stable Phase:
Surgery in order to:
Provide a functionally straight penis (20 degrees or less).
Correct the deformity when there is failure of non-surgical treatments.
Penile Trauma
Etiology
Trauma can be classified as penetrating (knife or bullet) or blunt.
Blunt trauma usually occurs in an erect penis during vigorous sex (erect penis can slip from the vagina and strike partners extra-vaginal sites such as perineum and pubic symphysis).
Penile fracture due to the rupture of the tunica albuginea and the corpus cavernosa.
Other causes include:
Fall.
Forceful masturbation.
Rolling over in bed with an erection.
Can be associated with a urethral tear.
Clinical Presentation
After penile trauma, patients report hearing a ‘cracking’ or ‘popping’ sound.
Most often present to the emergency department with:
Sharp pain.
Decrease in erection.
Swelling.
Deformity of the penis.
Bruising/discoloration due to ruptured blood vessels from trauma.
Ultrasound Examination
Measurement and location of possible hematoma.
Correct labeling of anatomy involved in order to describe location of fracture/hematoma.
Measurement of defect in longitudinal if a fracture is found.
Assessment with color doppler to rule out possible vascular injury to cavernosal artery.
Sonographic Features
Penile fracture can present as a ‘defect’ in the tunica albuginea with adjacent hematoma.
Doppler of both cavernosal arteries can demonstrate if intact or not.
If penis is not fractured, ultrasound typically demonstrates:
a) Rupture or thrombosis of dorsal vein of the penis (hematoma with intact tunica albuginea).
b) Intra cavernosal hematoma (occurs secondary to injury of sub-tunical venous plexus or smooth muscle without disruption to the tunica albuginea).
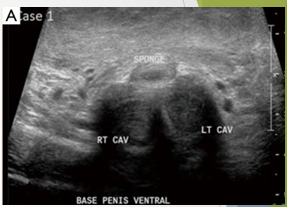
Patient attempting to urinate whilst penis erect. Heard ‘crack’ followed by acute pain
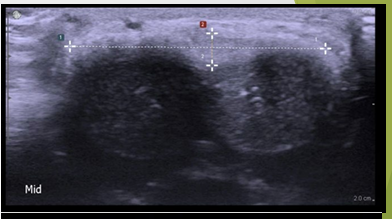
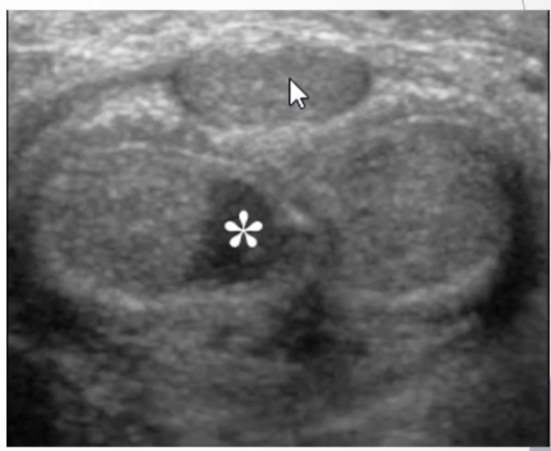
Normal anatomy at the base of the penis: Bilateral homogenous CC, Thin line of intact Tunica albuginea, Corpus spongiosm well demarcated
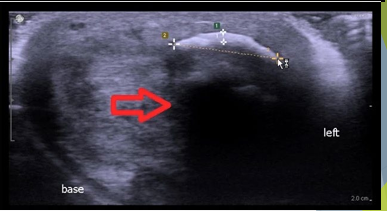
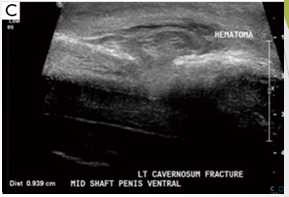
Mid shaft of penis defect noted with disruption of ventral tunica albuginea and left corpus cavernosum. Complex echogenic collection noted along left side of penile shaft

Defect in longitudinal measures 9.4mm. Hematoma noted ventral aspect.
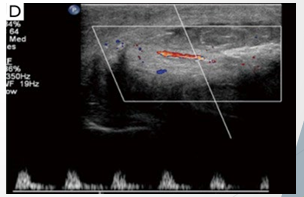
Normal arterial flow noted in left cavernosal artery. Important to rule out vascular injury
Indirect blunt trauma to flaccid penis crushing penile shaft against gas tank
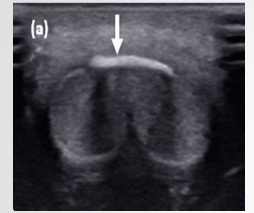
Scan through ventral aspect shows hypoechoic area within Rt corpus cavernosum, representing hematoma. Echogenic line of tunica albuginea intact representing no penile fracture
Penile Carcinoma
Etiology
Squamous cell carcinoma (SCC) accounts for the majority (>95%) of penile cancers.
Rare in the USA (%), however up to % of malignant neoplasms for men in Asia, Africa, and South America.
Risk factors include:
Human papilloma virus (HPV).
Smoking.
Increased number of sexual partners.
Chronic inflammation of penile skin.
Obesity.
Tight foreskin (circumcision protects from this).
Most commonly occurs in men 50-70 years of age.
Clinical Presentation
Patient usually presents with a palpable penile lesion.
Can be associated with:
Pain.
Discharge.
Bleeding.
Foul odor.
Lesion can be nodular, ulcerating, or fungating in appearance.
Mostly located on the glans of the penis but can also occur (less commonly) on the foreskin or shaft.
Many are associated with palpable inguinal lymph nodes indicating either metastatic spread or inflammatory reaction.
Ultrasound Examination
Measurement in long and trans the lesion and assess with color doppler.
Delineate local spread of tumor for possible extension into corpus cavernosum or urethra.
Evaluate and describe the possible presence of abnormal lymph nodes in the inguinal region (i.e., extend the examination if there is an indication of palpable nodes).
Sonographic Features
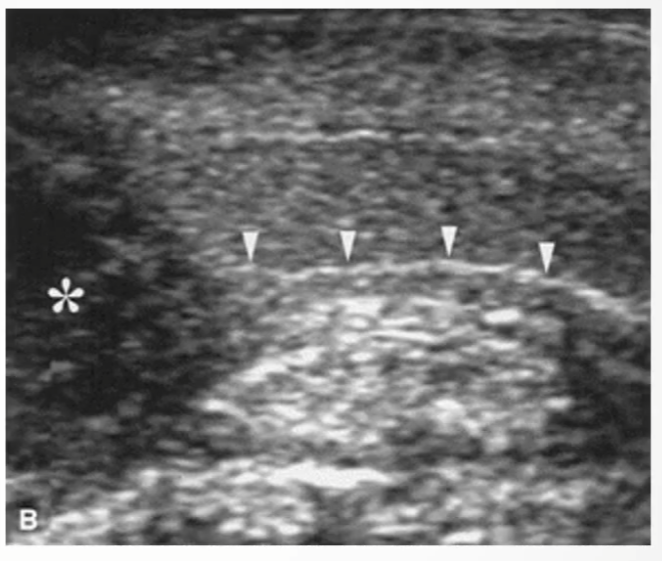
Typically presents as a hypoechoic lesion with a heterogeneous appearance.
If ulcerated, can produce hyperechogenic spots due to entrapped gas bubbles.
If infiltrated through the tunica albuginea, seen as an interruption of the thin echogenic line.
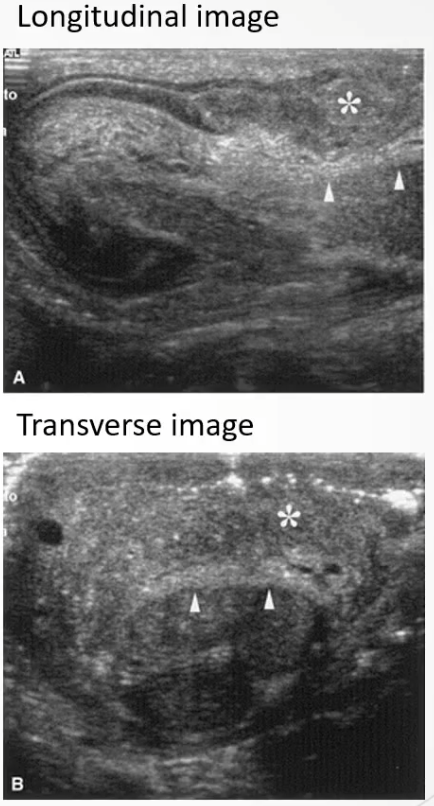
Longitudinal and Transverse images: Asterisk () demonstrates hypoechoic tumor which is confined to the subepithelial connective tissue and does not penetrate through or invade the tunica albuginea of the corpus cavernosa (arrows)*
Longitudinal view demonstrating hypoechoic SCC () invading through the echogenic line of the tunica albuginea (arrowheads)*