4. Angle Closure Glaucoma
Predisposing factors for angle closure glaucoma
Age: Older
Sex: Female
Race: Asian
Refractive error: Hyperopia
Family history: Positive (+ family history)
Essentially, predisposing factors are those which predispose to a small eye and a small/shallow anterior chamber (AC)
Emergency referral during an acute ACG attack
Mechanisms of angle closure
1) Pupillary block: contact between the lens and iris blocks aqueous outflow
2) Peripheral apposition of iris to the trabecular meshwork (TM) or cornea leading to angle closure
3) Primary angle-closure glaucoma (ACG) is generally attributed to pupillary block causing the iris to bow forward (iris bombé)
4) A very small percentage due to anatomical anomaly of plateau iris, causing TM blockage on dilation
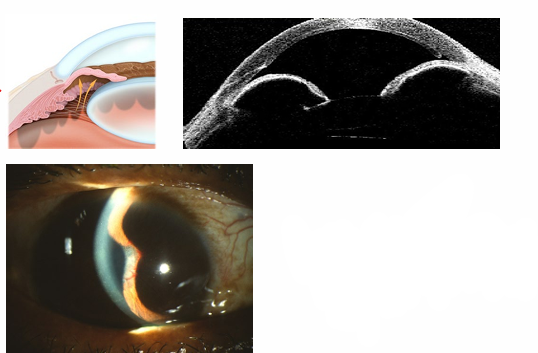
Pupil block and iris bombe
Pupillary block: root of the iris cuts off aqueous outflow
Iris bombe: iris billows anteriorly, blocking off the angle
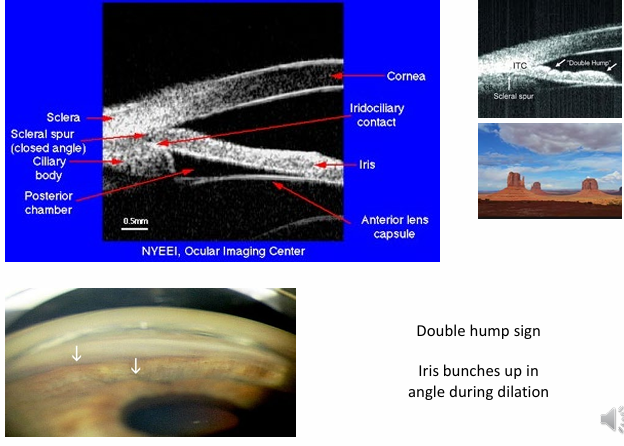
Plateau iris
Double hump sign: iris demonstrates two convexities in the angle, indicating plateau iris configuration
Clinical presentation
Subacute (intermittent)
Acute
Chronic
Subacute/intermittent angle closure
can present without symptoms
Important to elicit history of previous attacks and symptoms
Triggers: semi-mydriasis causing irido-corneal contact due to emotion, dim illumination, stress, or drugs
Symptoms of subacute ACG
Pain
Redness: conjunctival and ciliary injection
Aching pain in the globe, radiating to temples along the ophthalmic division of the trigeminal nerve
Haloes, misty, foggy, or steamy vision
Nausea and vomiting
Photophobia
Signs of subacute ACG
Evidence of previous attacks:
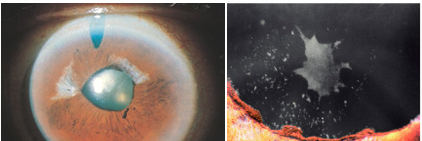
Iris stromal atrophy
Glaucomflecken (glaucoma flecks): mechanical insult to crystalline lens epithelium after elevated IOP
May progress to acute ACG or chronic ACG
Acute angle-closure glaucoma (ACG)
Presentation includes a painful red eye with ciliary flush and vision loss
More intense pain, with nausea and vomiting
Marked vision loss due to corneal edema and vascular compromise of the optic nerve (ON): typically from about to
Exam shows a fixed, sluggish mid-dilated pupil (iris sphincter paralysis with ↑ IOP)
Intraocular pressure (IOP) is raised, often very high: 50-60 mmHG
History may show evidence of previous attacks: glaucomflecken, iris stromal atrophy
The fellow eye commonly has a shallow angle/AC
Case example (acute presentation)
65-year-old female
1/52 painful left eye
Vision: VA down
IOP: 65 mmHg
Shallow AC
Fixed, semi-dilated pupil
Corneal edema
Glaucomflecken

Chronic angle-closure glaucoma (ACG)
Develops insidiously and can be asymptomatic
Gradual creeping closure of the angle
Shares changes with primary open-angle glaucoma (POAG): optic disc cupping and visual field (VF) defects